Research Article
The Effectiveness of Task-Oriented Functional Electrical Stimulation (FES) in Guillain-Barré Syndrome –A Scoping Review and Case Study
Borah AK1*, Goswami P2 and Saikia H3
1Department of Physiotherpy and Neurological Science, Mahatma Gandhi University, Ri-Bhoi Meghalaya, India,
2Department of Physiotherapy, Mahatma Gandhi University, Ri Bhoi, Meghalaya, India.
3Department of Orthopedics and Rehabilitation, Physiotherapy, Sanjevani Hospital, A T Road, Malegaon, Guwahati, India.
2Department of Physiotherapy, Mahatma Gandhi University, Ri Bhoi, Meghalaya, India.
3Department of Orthopedics and Rehabilitation, Physiotherapy, Sanjevani Hospital, A T Road, Malegaon, Guwahati, India.
*Corresponding author:Arup Kumar Borah, Department of Physiotherpy and Neurological Science, Mahatma Gandhi University, Ri-Bhoi Meghalaya, India. E-mail Id: barup614@gmail.com
Article Information:Submission: 24/02/2026; Accepted: 12/03/2026; Published: 14/03/2026
Copyright: © 2026 Borah AK, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Guillain-Barré Syndrome is an autoimmune disorder characterized by immune-mediated damage to the peripheral nervous system [Nguyen TP, StatPearls Publishing; 2024 Jan.]. GBS affects sensory, motor and autonomic nerves. There occurs temporary inflammation and demyelination of peripheral
nerve myelin sheaths resulting in axonal degeneration. It is the most common cause of rapidly progressive flaccid paralysis. It is believed to be one of a number of related conditions, all sharing a similar underlying autoimmune abnormality, as a group known as anti-GQ1b IgG antibody syndrome. Chronic inflammatory demyelinating (CIDP) is considered the chronic counterpart to Guillain-Barré syndrome [Radiopedia, Guillain-Barré syndrome, available: https://radiopaedia.org/articles/guillain - barre syndrome -2 ].
Keywords:Guillain−Barré Syndrome; Functional electrical stimulation; Neurorehabilitation; Pathogenesis; Acute motor axonal neuropathy
Objective
Functional Electrical Stimulation (FES) helps Guillain-Barré
Syndrome patients by strengthening weak muscles, improving
functional movement, reducing atrophy, boosting neuroplasticity,
and promotes beneficial changes in the nervous system, aiding
the brain in regaining control over movement and increasing
independence and quality of life, by activating muscles during tasks
or rest, aiding recovery from paralysis and sensory deficits, and can
even help manage pain, but it requires tailored, consistent therapy.
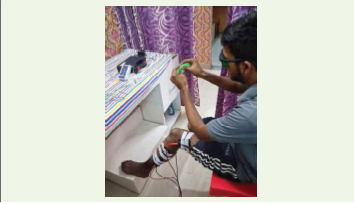
With a focus on these goals, FES was applied bilaterally to
improve hand closure and pinch grip. Based on principles of motor
learning FES was executed together with task-oriented movements.
The hand closure distance (cm) between the tip of the middle finger
and the palmar side of the hand was measured and the achievement
of personal, predefined goals evaluated.
Introduction
GBS Outbreak in 2024 and 2025 − While GBS is generally a rare,
non-communicable, autoimmune neurological disorder with an
estimated annual incidence of 1.75 to 2 cases per 100,000 populations
in India; the reported cases saw a notable increase in certain areas.
Pune Outbreak (Early 2025):
The city of Pune experienced an “unprecedented surge” in GBS
cases starting in January 2025. Pune reported 198 GBS cases in all of
2023 and 205 in all of 2024, but logged 141 cases in just the first two
months of 2025 alone, with nine suspected deaths. By February 2025,
Maharashtra had a total of around 211 cases, with fatalities reported.
The outbreak was primarily linked to contaminated water sources in
areas like Sinhgad Road, Nanded Gaon, and Khadakwasla, with the
identified pathogens including Campylobacter jejuni and Norovirus.Other States (2024-2025) - Cases were also reported in other
states, including Andhra Pradesh, Telangana, Assam, Tamil Nadu,
and Delhi.. Andhra Pradesh reported 53 cases between November
2024 and February 2025, with two confirmed deaths.
Method
Functional Electrical stimulation (FES) in Guillian-Barré
syndrome (GBS) low energy electrical current applied via surface
electrodes to stimulate peripheral nerves, inducing contraction in
paralyzed or weakened muscles. It is used to reduce atrophy, improve
motor function and retrain muscles, such in the hand or ankle during
rehabilitation particularly in chronic cases. Stimulation levels are
personalized based on patient tolerance and the level of contraction
achieved, focusing on strengthening and maintaining muscle tissue.
FES is effective for strengthening, its application in GBS requires
careful assessment of nerve damage to ensure effective stimulations.
The role of the immune system in the development of GBS originates:
Among the others from the fact that 70% of the GBS patients
reports a preceding infection prior to the onset symptoms.
Furthermore, the course of the disease can be influenced by immune modulating
therapies as plasmapheresis (PE) and intravenous
immunoglobulins (IVIg). Finally, with the finding of antibodies
directed against structures in the peripherals nerves, the role of the
immune system seems to be indisputable.In most cases in nerve damage is primarily caused by demyelination. Pathophysiological studies show lymphocytic infiltrates in spinal roots and peripheral nerves followed by macrophage-mediated segment stripping of the myelin (Asbury, AK et al.1969) [1]. As a consequence, electrical nerve impulses are disrupted leading to showing of nerve conduction and in some cases to conduction block (Hughes et al., 1999) [2]. In some cases, mostly severely affected patients, the inflammatory demyelination is accompanied by destruction and loss of axons (Berciano et al., 1993; Fuller JN et al., 1992; Hall, SM et al., 1992) [3-5]. It is difficult to distinguish these cases from the primary axonal forms in which the primary immune attack is directed against the nerve axons (Feasby, TS et al., 1986; Griffin, JW et al., 1996; Haefer-Maco, C et al., 1996) [6-8]. In these cases macrophages penetrate the basal lamina of the Schwann cell resulting in destruction of the axons. This process is without significant demyelination and lymfocytic infiltrates are scarcely present (Feasby, TS et al., 1986) [6]. But, the clinical phenotype of the primary axonal form and primary demyelinating form followed by secondary axonal degeneration is similar. Since pathological material from GBS patients is scarce and electrophysiological techniques are not able discriminate between primary or secondary axonal degeneration, the discrimination between these two groups is generally not possible in daily practice.
It is not exactly known when and how nerve tissue becomes
involved in the immune response and that has been major subject
of GBS research over last years. At present the theory of molecular
mimicry draws the attention and up to now it appears to be the most
attractive hypothesis in the development of GBS. As reaction to the
presence of a microbial agent, antibodies and / or T cells are produced
to act directly against the microbial antigens. Due to the structural
resemblance of the antigens and host tissue, the antibodies and/or
T cells not only destruct the pathogen but also cause damage to the
host tissue.
In GBS, the most extensively described relation between a pathogen, host tissue and antibodies are the relation between a preceding infection with Campylobacter jejuni (C. jejuni) and the presence of serum antiganglio-side antibodies cross-reacting with lipopolysac-charides from C. jejuni (Ang, CW et al., 2001; Gregson, NA et al., 1997; Vander pol, WL et al., 2000; Koga, M et al., 2000) [9-12]. Gangliosides are a subgroup of membrane glycolipids present in the nervous system. Different types of gangliosides are described. The composition of gangliosides in axons or myelin, but also in motor and sensory nerves and in ventral and dorsal nerve roots, varies (Ang, CW et al., 2001) [9].
In GBS, the most extensively described relation between a pathogen, host tissue and antibodies are the relation between a preceding infection with Campylobacter jejuni (C. jejuni) and the presence of serum antiganglio-side antibodies cross-reacting with lipopolysac-charides from C. jejuni (Ang, CW et al., 2001; Gregson, NA et al., 1997; Vander pol, WL et al., 2000; Koga, M et al., 2000) [9-12]. Gangliosides are a subgroup of membrane glycolipids present in the nervous system. Different types of gangliosides are described. The composition of gangliosides in axons or myelin, but also in motor and sensory nerves and in ventral and dorsal nerve roots, varies (Ang, CW et al., 2001) [9].
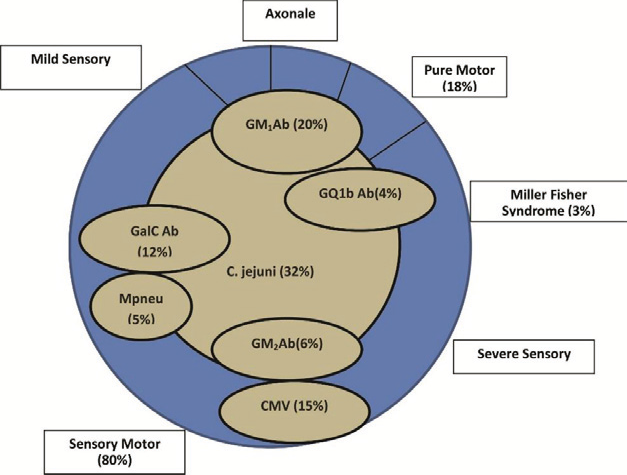
Subgroups
Guillain-Barré Syndrome is considered to be a heterogeneous
disorder. The pathophysiological mechanism has not been fully
elucidated, and the exact contribution is of preceding infections and
the presence of anti-ganglioside antibodies remain unclear. Recent
studies reporting on the relation with certain immune-response
gene polymorphisms have revitalised the thought that host factors
are likely to play a role (Vander pol, WL et al., 2000) [11]. It is not
known if the subgroups are completely based on similar underlying
pathophysiologic mechanisms and consequently, the diversity of
clinical picture of GBS is fully determined by the preceding infection,
presence of anti-gangliosides antibodies and/or host factors. Another
possibility is that different mechanisms play a vital role, which results
in a similar clinical picture.
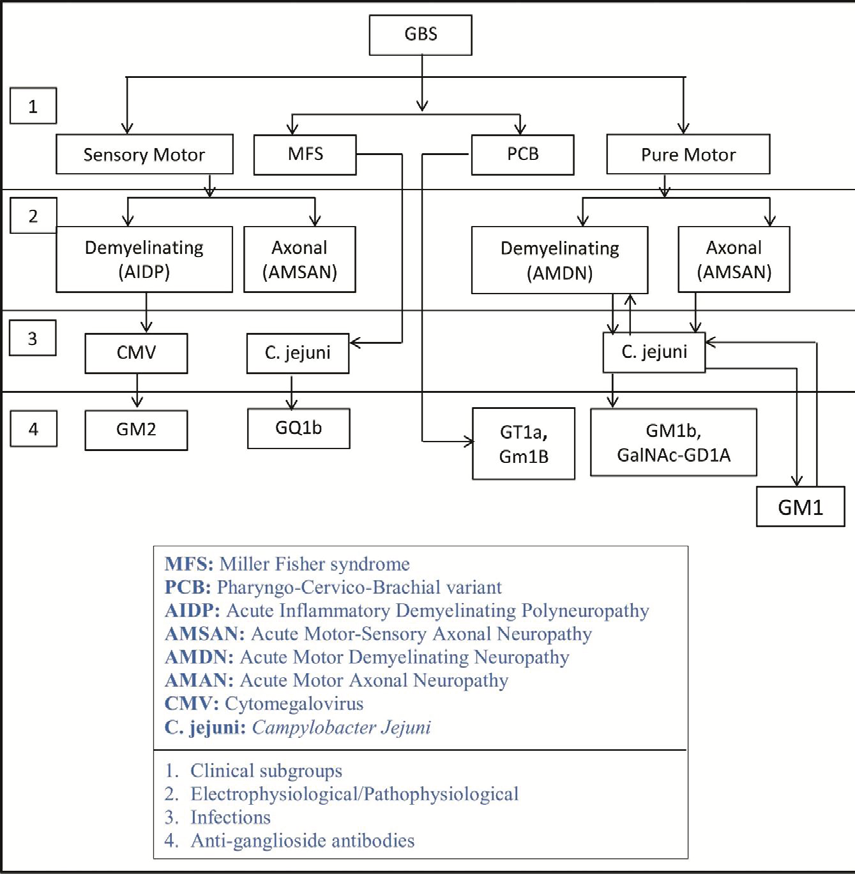
Classification of subgroups is possible on different levels of the disease and characteristic on several levels of the disease can be found in one subgroup (Table 2) and Figure 2(a). Moreover, it has been described between PCB and antibodies against GT1a and GM1b (Koga, M et al., 2000; Mizoghichi, K et al., 1994; Koga, M et al., 1998;Koga, M et al.,1999). [12-15]
In a study concerning these cranial variants, significant overlap was found between the variants and the classical GBS. In 59% of the cases, where symptoms started in the oculomotor-region, difficulty in swallowing followed, indicating involvement of the lower cranial nerves. In 33% of the cases, where symptoms started in the lower cranial nerve region, the oculomotor nerves become involved. In both variants, about half of the patients developed a descending weakness in the extremities (J.P. ter Bruggen et al., 1998) [16].
Classification of subgroups is possible on different levels of the disease and characteristic on several levels of the disease can be found in one subgroup (Table 2) and Figure 2(a). Moreover, it has been described between PCB and antibodies against GT1a and GM1b (Koga, M et al., 2000; Mizoghichi, K et al., 1994; Koga, M et al., 1998;Koga, M et al.,1999). [12-15]
In a study concerning these cranial variants, significant overlap was found between the variants and the classical GBS. In 59% of the cases, where symptoms started in the oculomotor-region, difficulty in swallowing followed, indicating involvement of the lower cranial nerves. In 33% of the cases, where symptoms started in the lower cranial nerve region, the oculomotor nerves become involved. In both variants, about half of the patients developed a descending weakness in the extremities (J.P. ter Bruggen et al., 1998) [16].
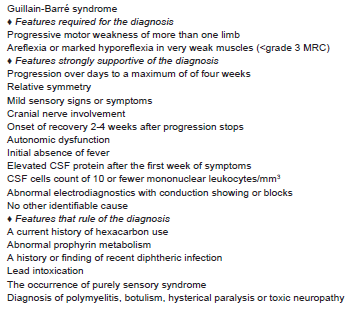
(Adapted from the Revised Version of the Diagnostic Criteria for
Guillain-Barre syndrome, set up the National Institute of Neurological
Disorder and Stroke.
Early signs and symptoms:
Guillain-Barré Syndrome signs start with tingling and weakness,
usually the legs that spreads upwards, affecting arms and face, leading
to difficulty walking, or swallowing and potentially rapid paralysis
and breathing problems requiring urgent care.The key symptoms including ascending weakness, loss of reflexes, intense pain, facial palsy, and autonomic issues like heart rate, blood pressure changes. Early detection is crucial as it can progress quickly to severe complications.
In frontline.thehindu.com F Packages – In India, more than 100 cases have been reported with hallmarks of the rare neurological disease that can cause paralysis (published Jan-30, 2025)
Therapeutic intervention:
All preliminary protocols have been completed to the hospital,
early rehabilitation was initiated. In the first observation – our aim
to maximize neuromuscular function and to gain back patient’s
functional independence, thereby improving quality of life.
Intravenous immunoglobulin (IVIg) was administered at a dose of
0.4/ kg body weight daily for 5 consecutive days.
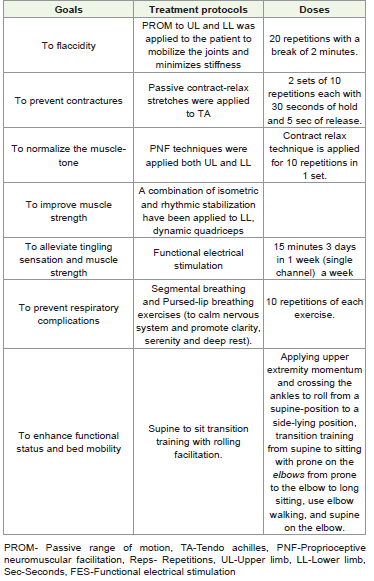
Moreover, relaxation was the basic pain management given in
(Table 3) provides a brief summary of the physiotherapy intervention
received by the patient.
Pre intervention (During 4 weeks) - Now, the ultimate outcome
of neurorehabilitation was to see improvement in a 18-year-old
(Male) boy suffering from GBS at the end of the session, which is
summarized in (Table 4) to (Table 6) as shown below: Moreover, the
outcome measures used are summarized in (Table 7).
(Hence, upper extremity prevention Day 1 refers to the (using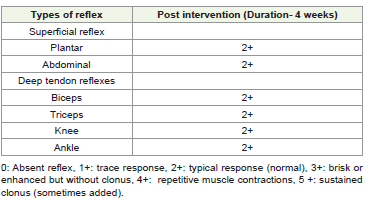



DASH questionnaire), 1/5 on day 1 indicates a positive indicator,
suggesting a good initial function or minimal problems with the
upper extremity at the start of our assessment.
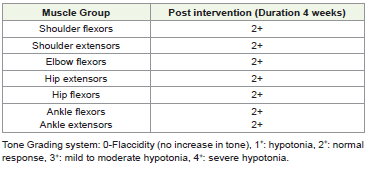
Moreover, Pre intervention in 4 weeks in Lower extremity which
indicates as good, and can complete a full range of motion against
gravity plus tolerate a moderate amount of resistance with a good
strength).
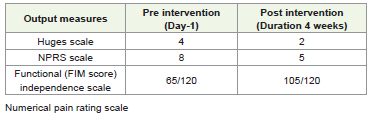
Huges scale grading breakdown (Huges Functional Grading scale
for Guillain-Barré syndrome patients):
0: no pain, 1: minor symptom but can run (can be problematic
for some GBSs’ patient), 2: able to walk 10 meters unaided, 3: needs
help to walk 10 meters, 4: Bedridden or chairbound, 5: need assisted
ventilation breathing and 6: Death.
The 2025 Pune, Outbreak:
Timing: Started February 2025, spreading to other states like
Andhra Pradesh.• Scale: High-profile cluster with 180 hospitalizations and 14 deaths reported, notes Gavi.
• Cause: Linked to contaminated municipal water (organochlorine pesticides), showing environmental factors are critical, not just infections.
Impact: Highlighted gaps in water quality monitoring and public health response beyond traditional infection surveillance.
Recent Trends and Challenges::
• COVID-19 Era: Studies analyze GBS trends pre and postpandemic,
noting potential links to vaccines and infections.• Need for Preparedness: The Pune outbreak stressed the need for integrated surveillance (water, infection, GBS) and improved infrastructure to prevent future crises.
Epidemiology of GBS
Incidence rates:
GBS can affect all people and is not restricted to specific area nor
related to factors as gender, age, race, standard of living or climate.
Over the years 25 studies were assessed on the epidemiology of GBS
in (Table 1).
In the year 2025, 9 January, the first case of Guillain-Barré
syndrome was reported in Pune, a major city in Maharasthtra, the
number of cases surged dramatically, peaking on January 22, with
35 new cases detected that day (35 Suspected Cases of Guillain-Barré
Syndrome Deccan Herald. March 8, 2025) [19].
Moreover, by Mid of March, 2025, 230 cases and 12 deaths
(case fatality rate, 5.2%) were reported across the entire state of
Maharasthtra, with Pune being the epicenter of the Guillain-Barré
syndrome outbreak with 215 cases and 10 deaths, fatality rate 4.6% .
Hence, the outbreak in Pune was declared over after 27 days without
any new cases of GBS following February 18, 2025 (Dolare R. GBS
outbreak in Pune declared over as No New Cases reported since
February 18. Punekar News; 2025). However, approximately 90% of
cases were under 60 years of age, with more than 55% being younger
than 30 years. A male predominance was observed, accounting for
68% of the cases in the GBS outbreak (Bureau TH, Suspected Guillain-
Barré syndrome cases rise to 163 in Maharashtra. The Hindu; 2025;
Kandi V (2025) [17]; Pune Guillain Barré Syndrome Caseload at 130;
55% of patients are below 30-Pune News, The Times of India, 2025)
Hence, outbreak continued, additional cases, were reported in
Andhra Pradesh, (AP) Telangana, Tamil Nadu, Kerala, Assam and
West Bengal, raising the national total to over 300 cases and 21 deaths
(case fatality rate 7%) (Lateef S, 2025) [18].
Since Guillain-Barré Syndrome is not contagious, no travel
restrictions were imposed during the outbreak, however, travellers
were advised to follow standard health precautions (Pune’s Guillain-
Barré Syndrome Cases cause Traveller Concerns, 2025; Practitioner
TI, 2025).
During the larger Guillain-Barré Syndrome outbreak in Peru
in the year 2023, the World Health Organization (WHO), did not
recommend any travel or trade restrictions in response to the outbreak
(Guillain-Barré Syndrome-Peru. Available from: https://www. who.
int/emergencies/disease-outbreak-news/item/2023-DON477, 2025).
Serological studies revealed a significantly higher prevalence of
anti-C.jejuni antibodies among GBS patients (immunoglobulin M
(IgM) 84%, IgG 87.5%) compared to healthy individuals (IgM 33%,
IgG 27%), indicating prior infection (Zhang, M et al., 2010) [19].
Molecular analyses suggested a common source, strongly implicating
C. jejuni as the primary trigger.In addition, clinical and electrophysiological assessment identified
acute motor axonal neuropathy as the predominant subtype, which is
associated with prolonged illness and poorer prognosis. Henceforth,
the outbreak was ultimately traced to contaminated drinking water,
underscoring the importance of environmental factors in C.jejuni
transmissions (Ye, Y et al., 2010) [20].
Moreover, a similar large-scale outbreak occurred in Peru in 2019, affecting nearly 700 individuals, with food borne transmission identified as the primary route (Guillain-Barré Syndrome–Peru. Available from: https://www.who.int/emergencies/disease-outbreaknews/ item/2023-DON477). In 2020, more recently, an outbreak of acute neurological illness in Eluru, Andhra Pradesh, India resulted in over 500 hospitalizations. Although, initially suspected to be infectious, investigations revealed that the cause was municipal water contamination with organochlorine-pesticides rather than a microbial agent (Sharma, S et al., 2023) [21]. In 2023, Peru declared a health emergency after a C.jejuni induced Guillain- Barré Syndrome outbreak (Quino, W et al., 2022) [22]. In Brazil, Zika and chikungunya viruses have been linked in spikes in GBS cases (Leonhard, SE, et al., 2021) [23] A study by the national Institute of Mental Health and neurosciences, found that between 2014 and 2019, nearly 80% of Guillain-Barré Syndrome in India were preceded by infections−most commonly with the chikugunya-virus (Dutta, D et al., 2021) [24-39]. Without a comprehensive surveillance system that integrates, human, animal, and environmental health data, such outbreaks will continue to blindside public health officials. An epidemic in most parts of the world, C. jejuni is a zoonotic pathogen, which can enter the food-chain through undercooked poultry, unpasteurized diary, and contaminated water sources. While infections with C.jejuni typically self-limiting, in some cases, the immune response goes away leading to GBS. This happens when the antibodies generated to fight the infection mistakenly attack the gangliosides that covers peripheral nerves, leading to axonal degradation and demyelination and eventual paralysis.
Moreover, a similar large-scale outbreak occurred in Peru in 2019, affecting nearly 700 individuals, with food borne transmission identified as the primary route (Guillain-Barré Syndrome–Peru. Available from: https://www.who.int/emergencies/disease-outbreaknews/ item/2023-DON477). In 2020, more recently, an outbreak of acute neurological illness in Eluru, Andhra Pradesh, India resulted in over 500 hospitalizations. Although, initially suspected to be infectious, investigations revealed that the cause was municipal water contamination with organochlorine-pesticides rather than a microbial agent (Sharma, S et al., 2023) [21]. In 2023, Peru declared a health emergency after a C.jejuni induced Guillain- Barré Syndrome outbreak (Quino, W et al., 2022) [22]. In Brazil, Zika and chikungunya viruses have been linked in spikes in GBS cases (Leonhard, SE, et al., 2021) [23] A study by the national Institute of Mental Health and neurosciences, found that between 2014 and 2019, nearly 80% of Guillain-Barré Syndrome in India were preceded by infections−most commonly with the chikugunya-virus (Dutta, D et al., 2021) [24-39]. Without a comprehensive surveillance system that integrates, human, animal, and environmental health data, such outbreaks will continue to blindside public health officials. An epidemic in most parts of the world, C. jejuni is a zoonotic pathogen, which can enter the food-chain through undercooked poultry, unpasteurized diary, and contaminated water sources. While infections with C.jejuni typically self-limiting, in some cases, the immune response goes away leading to GBS. This happens when the antibodies generated to fight the infection mistakenly attack the gangliosides that covers peripheral nerves, leading to axonal degradation and demyelination and eventual paralysis.
Participant description:
The study participant was an 18-year-old boy patient diagnosed
with GBS in March 2025. Moreover, previously he has gastritis
caused by an infection with campylobactus jejuni. Within 28 days,
progressive mild paralysis developed. It began distally in the feet and
hands that ended in a respiratory failure.Discussion, Conclusions and Direction of Future Research
The results of this case demonstrates that fine motor skills can
improve following of 16 week intense treatment of FES combined
with task oriented functional training in an individual with chronic
GBS with hyperreflexia. After finishing FES, the function persisted,
controlled and confirmed in the annual follow up performed by the
responsible therapists.
Positive effects of the combination of IVIg and MP (Mycoplasma Pneumoniae). It was shown that this effect was mainly achieved during the first three months after onset. Long term morbidity in GBS is still considerable. Hence, new treatment studies should therefore preferably focus on the reduction of long-term nerve damage due to Guillain-Barré Syndrome. With our present knowledge and insights, it has become clear that almost all diseases are multifactorially induced.
The results of the present study demonstrate that fine motor skills can improve following 24 weeks intense treatment of FES combined with task oriented functional training in an individual with Guillain- Barré Syndrome. After completing FES, the function persisted controlled, and confirmed in the annual follow-ups performed by the responsible therapist.
Task-oriented functional training supported by FES can lead to long - term improvements in the fine motor function of upper and lower extremities, even in chronic cases after GBS with preserved deep tendon reflexes.
Positive effects of the combination of IVIg and MP (Mycoplasma Pneumoniae). It was shown that this effect was mainly achieved during the first three months after onset. Long term morbidity in GBS is still considerable. Hence, new treatment studies should therefore preferably focus on the reduction of long-term nerve damage due to Guillain-Barré Syndrome. With our present knowledge and insights, it has become clear that almost all diseases are multifactorially induced.
The results of the present study demonstrate that fine motor skills can improve following 24 weeks intense treatment of FES combined with task oriented functional training in an individual with Guillain- Barré Syndrome. After completing FES, the function persisted controlled, and confirmed in the annual follow-ups performed by the responsible therapist.
Task-oriented functional training supported by FES can lead to long - term improvements in the fine motor function of upper and lower extremities, even in chronic cases after GBS with preserved deep tendon reflexes.
Statement of Ethics:
We certify that all applicable institutional and government
regulations concerning the ethical use of human volunteers were
followed during the course of this research.Competing Interest: The authors declare no competing interest.
The corresponding author, Arup Kumar Borah; E-mail: barup614@gmail.com is a Post-doctoral fellow and works as consultant in Spinal Life Physiotherapy clinic a multispecialty digital setup, Six Mile Jayanagar Road, Guwahati-781022, India.
The corresponding author, Arup Kumar Borah; E-mail: barup614@gmail.com is a Post-doctoral fellow and works as consultant in Spinal Life Physiotherapy clinic a multispecialty digital setup, Six Mile Jayanagar Road, Guwahati-781022, India.
Acknowledgements
The authors would like to express our deepest appreciation to
the Professor and Head of the Department of Neurology, All India
Institute of Medical Science, AIIMS, Dr. Masaraf Hussain Changsari
Guwahati-781011, for his invaluable contribution and collaborative
spirit throughout the research work, and Dr. Surajit Roy, Senior
Consultant of Spinal Life Physiotherapy Clinic, a multispecialty
digital setup, Community Based Rehabilitation, Six Mile, Jayanagar
Road, Guwahati-781022, Assam.
References
Citation
Borah AK, Goswami P, Saikia H. The Effectiveness of Task-Oriented Functional Electrical Stimulation (FES) in Guillain-Barré Syndrome –A Scoping Review and Case Study. J Immunol Vaccine Technol. 2026;4(1): 108.