Review Article
A Brief overview of Genetics of EsophagealSquamous Cell Carcinoma
Indranil Chattopadhyay*
Corresponding author: Indranil Chattopadhyay, Assistant Professor, Department of Life Sciences, Central University of TamilNadu, Thanjavur Road, Thiruvarur-610004, Tamil Nadu, India,; E-mail: indranil@cutn.ac.in
Citation: Chattopadhyay I. A Brief overview of Genetics of Esophageal Squamous Cell Carcinoma. J Cell Sci Molecul Biol. 2014;1(1): 103.
Copyright © 2014 Indranil Chattopadhyay. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Cell Science & Molecular Biology | Volume: 1, Issue: 1
Abstract
Esophageal Cancer (EC) is the eighth most common incident cancer in the world because of its extremely aggressive nature and poor survival rate. Cancer of the esophagus typically occur in one of two forms, squamous cell carcinomas arising from the stratified squamous epithelial lining of the organ, and adenocarcinomas affecting columnar glandular cells that replace the squamous epithelium. Squamous Cell Carcinoma (SCC) is the predominant histologic type of esophageal cancer worldwide. Esophageal cancer occurs at a rate 20 to 30 times higher in China than in the United States. An esophageal “cancer belt,” primarily squamous cell cancers, extends from northeast China to the Middle East. Population-based and hospital –based cancer registries in India, have reported the highest incidence of esophageal cancer in Assam in the north east region of the country, followed by Bangalore and Bombay. Evidence of an association between environment and diet and esophageal cancer comes from the profound differences in incidence observed in various parts of the world. The genetic and molecular changes underlying the development of ESCC remain poorly understood. In the past decade, efforts have been made to use candidate gene approaches to identify genetic susceptibility factors for ESCC. The identification of signature gene mutations in ESCC was recognized as a valuable starting point, providing a conceptual framework to guide the future analysis of complex aspects of this disease. How these genetic changes translate into the classical biological features of ESCC cells stands as a key area for increased active investigation. So how can information and technological advances are integrated to create a ‘roadmap’ for an improved understanding of ESCC biology, and how might such systems lead to more effective treatments?
Keywords: Esophageal cancer; High risk area; SNP; Mutation
Introduction
Cancer is a highly complex disease which can encompass multiple genomic alterations, including point mutations, translocations, gene amplifications, epigenetic modifications, deletions, aberrant splicing, and altered gene expression. These changes may be inherited or somatically acquired during progression from a normal to a malignant transformed cell. Among human cancer, esophageal carcinogenesis appears to be a complex multi-step process with a multi-factorialetiology, where environmental, geographical and genetic factors appear to play major role [1,2].
Description of study area, climate and vegetation
Esophageal cancer is among the ten most common malignancies worldwide and ranks as the sixth leading cause of death from cancer. It constitutes 7% of all gastrointestinal cancers and is one of the most lethal of all cancers [3]. Globally esophageal cancer ranks as the sixth most common cancer among males and ninth most common cancer among females. However, in India, it is the second most common cancer among males and the fourth most common cancer among females [4]. The incidence of esophageal cancer varies greatly between developed and developing countries and a 50-fold difference has been observed between high and low-risk populations. It is more common in Asian than in western countries. The esophageal cancer belt is a geographic area of high incidence, which stretches from northcentralChina westward through Central Asia to northern Iran [3]. Ahigh frequency of esophageal cancer has been reported from certain parts of China, Iran, South Africa, Uruguay, France and Italy [5]. The uneven geographical distribution of esophageal cancer reflects the influence of local environmental conditions, lifestyle factors andgenetic predisposition in the development of this cancer [6].
Histological subtypes of esophageal cancer
Esophageal cancer exists in two main forms with distinct etiological and pathological characteristics, squamous cell carcinoma (SCC) and adenocarcinoma. More than 90% of esophageal cancers worldwide are SCCs, although adenocarcinomas are more prevalent in the USA. SCC is often preceded by increased proliferation ofesophageal epithelial cells leading to basal cell hyperplasia, dysplasia, and carcinoma in situ [5]. Several predisposing factors that lead to esophageal squamous cell carcinoma (ESCC) include tylosis, lye ingestion, achalasia and Plummer-Vinson syndrome [7].
Risk Factors of esophageal cancer
Tobacco and alcohol, known to be involved in the carcinogenesis of esophageal cancer, have been reported to interact in a multiplicative way in the etiology of this neoplasm [8]. Tobacco smoking and alcohol drinking are strongly associated with the risk of esophageal SCC and to a lesser degree with the risk of esophageal adenocarcinoma. Reports from Southern India suggest that ESCC occurs in more than 80% of cases in chronic tobacco smokers that is further potentiated by heavy use of alcohol and additional prevailing risk factors, including nutritional factors and vitamin deficiencies [1]. Areca nut chewing, or betel quid chewing, a common habit in Southeast Asia, has been found recently by epidemiological studies from India, Taiwan and Thailand, to increase the risk of developing esophageal cancer by 4.7–13.3-fold, although other exogenous risk factors may be also have contributed to the development of the disease [8]. In South America, Central and Southeast Asia, the consumption of hot beverages is also considered as a risk factor. Many other factors such as dietary nitrosamine, micronutrient deficiency, HPV, opium, and spicyfood have been suggested as possible additional factors [6]. ESCC in the Indian population is associated with poor nutritional status, low socioeconomic conditions, bidi smoking and consumption of smokeless tobacco products, besides alcohol drinking and cigarette smoking [4].
Population-based and hospital –based cancer registries in India, have reported the highest incidence of esophageal cancer in Assam in the north east region of the country, followed by Bangalore and Bombay [9]. Assam, the largest state in this region, has a diverse population structure comprising many ethnic and linguistic groups, each having its own life styles, cultures and customs. The dietary patterns are also quite different from the rest of the country. The ethnic groups who had migrated several centuries ago from South China, Thailand, Myanmar and other Southeast Asian countries are now living as indigenous people. With the diverse tribal and nontribal mix of life styles and cultures, this region is the paradise for epidemiologists who seek the etiological clues from the geographic variations in the occurrence of the various diseases and the relationship between the genetic and environmental factors in this area. This is especially true in the case of esophageal cancer. Betel nut chewing with or without tobacco has been shown to be independently associated with the development of esophageal cancer in Assam [9]. More than 80% of the people of Assam chew typical raw (green) ripe betel nuts after being specially fermented underground for more than a month. The impact of these differences in risk factors for ESCC in North-east Indian population, in comparison with Chinese and Western population, on the molecular pathogenesis of the diseaseremains to be determined.
Genetic factors (family history) responsible for esophagealcancer
Within these high-risk regions, studies have shown a strong tendency toward familial aggregation, suggesting that genetic susceptibility, in conjunction with potential environmental exposures, may be involved in the etiology of this cancer [10]. The aggregation of esophageal cancer in families is a long-observed and well-documented phenomenon, but it is still subject to explore. Genetic predisposition is based on individual types of carcinogen activation or detoxification and DNA repair in a population at risk [6]. A positive family history was found to be associated with an increased risk of esophageal cancer in several case-control and cohort studies in China, Iran and Japan [11]. The familial aggregation of esophageal cancer among the Turkmen population in northern Iran may reflect the influence of environmental factors operating on individuals who are already genetically susceptible [12]. Environmental factors are probably the main contributor to the familial aggregation of cervical, lung and upper aerodigestive tract cancer [13].
The role of genetics in the development of esophageal cancer is also supported by previous reports of familial aggregation of esophageal cancer and by one segregation analysis of esophageal pedigrees that suggested an autosomal recessive Mendelian inheritance pattern. Preliminary studies have shown high frequencies of loss of heterozygosity (LOH), characteristic patterns of gene expression andsignificant differences in both LOH and gene expression by family history in ESCC tumors from a high-risk population in neighboring Shanxi Provinces of China [14]. Molecular profiles in ESCC are highly consistent and expression patterns in familial cases were different from those in sporadic cases of high-risk area of China [10]. Esophageal cancer was significantly more common in the first degree relatives of the cases than the relatives of unaffected controls in the Turkmen population of Iran. This suggests that genetic factors contribute significantly to the high incidence rate of esophageal cancer among Turkmen [15]. Familial clustering of cancer has been one of the main avenues to the understanding of cancer etiology and the signal to the involvement of heritable genes [16].
Previous studies of ESCC have shown a high frequency of allelic loss on chromosome 13q, infrequent somatic mutations in BRCA2, and a suggested association between a positive family history (FH+) of upper gastrointestinal cancer and germ line BRCA2 mutations [17]. An earlier study from China and Iran suggested that BRCA2 may play a role in the etiology of ESCC. Recent studies reveal that the BRCA2 protein is required for maintenance of chromosomal stability in mammalian cells and functions in the biological response to DNA damage, as evidenced by the finding that mutations in BRCA2 lead to chromosomal instability due to defects in the repair of double-strand and single-strand DNA breaks [17,18]. Several studies have made efforts to understand the role of genetics in the etiology of SCC of the esophagus by attempting to identify molecular events associated with the development of precursor and invasive lesions.
Molecular alterations in human esophageal SCC
Molecular studies of human esophageal tumors have revealed frequent genetic abnormalities. Regardless of patient origin and suspected etiological factors, genetic changes that are consistently observed in esophageal SCC are: (i) alterations in tumor suppressor genes, specifically p53, leading to altered DNA replication and repair, cell proliferation and apoptosis; (ii) disruption of the G1/S cell cycle checkpoint and loss of cell cycle control; (iii) alterations in oncogene function leading to deregulation of cell signaling cascades [5].
Over expression of Cyclin B1 in ESCC has been reported to induce tumor cell invasive growth and metastasis [19]. PTEN may play a role in carcinogenesis and progression of ESCC in a high incidence area of northern China [20]. Most commonly used serum markers of ESCC include cytokeratin 19-fragment, squamous cell carcinoma antigen, and carcinoembryonic antigen, which show poor sensitivity of 43.9%, 26.8% and 17% respectively. Despite advancement in therapy, the overall 5-year survival rate of esophageal cancer still remains less than 30%. This has been largely attributed to the lack of an early diagnostic marker with desired sensitivity and specificity [7]. Additional markers that are known to be over expressed in early stages of ESCC include ALCAM, BPA-2, MMP13, MMP7 and MMP9. Coexpression of MMP7, MMP9, and MMP13 has also been associated with poor outcome in ESCC [7]. It has been previously reported that E-cadherin is commonly down regulated by CpG island hypermethylation in ESCC that predicts the poor prognosis of patients [21,22]. Reduced expression of TGM3 may play an important role in esophageal carcinogenesis [23,24]. Altered Ras function can contribute to human esophageal SCC development [5]. Up-regulation of Aurora-A expression may reflect the malignant behavior of ESCC and may prove useful information as a prognostic factor for ESCC patients [25,26]. Over expression of oncogenes Fra-1 and Neogenin and cell cyclerelated genes Id-1 and CDC25B were reported in ESCC [27]. VEGF-C may also play a role in tumor progression via lymphangiogenesis and angiogenesis in human esophageal carcinoma [28-30]. It has been demonstrated that COX-2 is expressed in the majority of esophageal SCCs and COX-2 derived prostaglandins play an important role in the regulation of proliferation and apoptosis of esophageal tumor cells [31,32]. EMP3 may be a tumor suppressor gene at the last step of esophageal carcinogenesis [33]. Down-regulation of RUNX3 may play a role in disease progression of ESCC [34]. mRNA and protein level of CDC25B and LAMC2 were over expressed in esophageal squamous cell carcinomas and premalignant lesions in subjects from a high-risk population in China [35]. A loss of FHIT expression is associated not only with alcohol-induced esophageal carcinogenesis, but also with multicentric carcinogenesis [36]. Stefin A plays an important role in the growth, angiogenesis, invasion, and metastasis of esophageal cancer suggesting that stefin A may be useful in its therapy [37].
An earlier study has reported that Arachidonic acid metabolism pathway and its altered expression may contribute to esophageal squamous cell carcinogenesis [38]. Detection of DDH over expression in ESCC cells would then provide an alternative link between chronic inflammation and carcinogenesis of esophagus, and, possibly, the disease progression of ESCC [39]. Survivin mRNA expression in ESCC has been reported as a good biomarker for identifying patients with high risk of cancer recurrence [40]. It has been reported earlier that OPN is associated with esophageal tumorigenesis and progression, but not patients’ survival [41]. Up-regulation of MAP3K3, AKAP13, ZnT7 and TG2 and deregulation of genes associated with zinchomeostasis were reported in ESCC of low-risk region of India [4]. Studies on differential global gene expression profiling in ESCCs using cDNA and oligonucleotide arrays have been performed in Chinese, Japanese and Western population. These studies revealed the complex nature of molecular changes associated with development of ESCC and suggested deregulation of differentiation associated genes and arachidonic acid metabolism in ESCC [4].
Chromosomal or gene copy number alterations are one of the main important mechanisms that perturb normal gene function by inducing changes reflected in gene expression [42]. Gene amplifications and deletions are frequently contributed to tumorigenesis [43]. Earlier studies have shown a very high level of chromosomal instability in ESCC from this high-risk area of China. Frequent allelic deletions and other genetic abnormalities affecting individual tumor suppressor genes have been detected in these tumors. Chromosomal regions with frequent allelic loss may point to major susceptibility genes that will assist in understanding molecular events involved in esophageal carcinogenesis and serve as the basis for the development of markers for genetic susceptibility testing and screening for the early detection of cancer [44]. Genomic alterations include various types of mutations, translocations, and copy number alterations. The last category involves chromosomal regions with either more than two copies (amplifications), one copy (heterozygous deletions), or zero copies (homozygous deletions) in the cell. Genes contained in amplified regions are natural candidates for cancercausing oncogenes, while those in regions of deletion are potential tumor-suppressor genes. Thus, the localization of these alterations in cell lines and tumor samples is a central aim of cancer research [45]. Comparative Genome Hybridization (CGH) and loss of heterozygosity (LOH) analysis are standard approaches used to characterize copy number changes on a whole-genome or candidate gene level. LOH studies and conventional comparative genomic hybridization (CGH) analyses have demonstrated genetic complexity in ESCC and have identified multiple recurrent copy number alterations, namely gains of 1q, 2q, 3q, 5p, 7p, 7q, 8q, 11q, 12p, 12q, 14q, 17q, 20p and 20q. Amplifications of regions harboring oncogenes e.g. 7p12 (EGFR), 8q24 (MYC), 17q21 (FGFR) and 11q13 (CCND1, FGF4/3, and EMS1) have consistently been observed. Losses, albeit at a lower frequency than gains, have recurrently involved 3p, 5q, 9p, 13q, 18q and 21q and include target genes such as FHIT, APC, RB1 and CDKN2A [46]. Frequent deletions were found on chromosome arms 1p, 3p, 4p, 5q, 8p, 9p, 9q, 11q, 13q, 16p, 17p, 18q, 19p, and 19q in ESCC [47]. Some of the changes identified, e.g. gain of 8q24, 11q13, 12p and 20q12 and loss of 3p have been associated with poor prognosis, but genetic alterations and biological characteristics have so far had a limited impact on clinical prognostication and treatment [46].
Traditional techniques, such as microsatellite analysis and BAC-CGH, are laborious, have limited whole-genome resolution, and represent challenges to data standardization initiatives. Gene Chip oligonucle tide arrays provide a standard platform to enable data standardization, as well as higher resolution, to detect smaller changes and map genetic boundaries. Furthermore, single nucleotidepolymorphism (SNP) arrays offer significant advantages over traditional methods by combining copy number, LOH, and SNP genotyping analysis into a single assay, thereby enabling the detection of copy neutral LOH events.
Cancer development is a complex multi-step process, involving various genetic and epigenetic changes. Progress of phenotypes from normal to advanced carcinoma is controlled by a transcriptional hierarchy that coordinates the action of hundreds of genes [48]. During the past decade, increasingly research results have distinguished how these genomic perturbations drive cancer cell survival by alteration the mechanism for cell cycle control, DNA repair, differentiation, apoptosis, tumor vascularization, and metabolism. By improving the understanding of these molecular mechanisms, scientists have gained insight into the initiation of cancer, its progression and its sensitivity to different therapeutics. Conventional approaches investigating one or several candidate genes at a time can not show the whole story of carcinogenesis. The generation of vast amounts of DNA sequence information, coupled with advances in technologies developed for the experimental use of such information, allows the description of biological processes from a view of global genetic perspective. However, little is known about the exact expression changes in each stage of tumorigenesis, which will help us to identify the exact series of events that leads to the initiation and progression of cancer development. As a step toward understanding the complicated changes between normal and malignant cells, this report focused on gene expression profile variations among normal and abnormal esophageal epithelium tissues. To illustrate the mechanisms controlling malignant changes at molecular level may provide a further understanding of tumorigenesis, as well as new approaches in early detection and treatment of esophageal cancer. One such technology, DNA microarray, permits simultaneous monitoring of thousands of genes [48]. Global expression analysis using microarrays now allows for simultaneous interrogation of the expression of thousands of genes in a high-throughput fashion and offers unprecedented opportunities to obtain molecular signatures of the state of activity of diseased cells and patient samples. cDNA microarray technology is a useful tool to discover genes frequently in esophageal neoplasia and provides novel clues to diagnosis, early detection and intervention of SCC [49].
Genetic alterations reported in ESCC of High-risk region in India
Gene expression profiles of esophageal cancer in a high-risk region of Assam in India identified down regulated genes involved in structural constituents of ribosome and up regulated genes involved in cation transporter activity, GPCR activity and MAPK activity in non-familial ESCC cases with history of tobacco andbetel quid consumption [50]. Familial clustering of cancer in these patients of high-risk region of India may be more due to shared environmental factors rather than shared genes by family members [51]. Copy number alteration study revealed that candidate genes in the potential signaling pathways (focal adhesion, tight junction, the MAPK signaling pathway and the neuroactive ligand receptor interaction pathway) might be used as molecular biomarkers in the early detection of ESCC in high-risk area of India in association with tobacco and betel quid use [52]. Nonsynonymous variants in exon 18 (K2729N) and exon 27 (I3412V) of BRCA2 gene were found in 3 of 20 patients with familial ESCC. No sequence alterations were found in 80 non-familial ESCC cases (P = 0.01) and 100 healthy controls (P = 0.0037), suggesting that germ line BRCA2 gene mutation may play a role in familial aggregation of ESCC in high-risk region of India [53]. EPHX1 exon 4 139His/Arg and 139Arg/Arg genotypes were associated with a higher risk of esophageal cancer in a high-risk area of India [54]. Significant association of GSTM1 null genotype in Assam was observed between cancer cases and controls in fermented betel nut chewers only (OR-2.8, 95%CI, 1.19–6.72),whereas, smoking and alcohol failed to show any correlation with GSTM1/GSTT1 genotypes [55].
TNFA-308GA genotype was associated with increased risk of ESCC specifically in females and in patients with regional lymph node involvement, while, NFKBIA -826CT+TT genotype conferred decreased risk of ESCC in females. Haplotypes of NFKBIA -826C>T and 3’UTRA>G polymorphisms, C-826G3’UTR and T-826A3’UTR, were associated with reduced risk of ESCC. TNFA-308 and NFKBIA (-826C>T and 3’UTRA>G) polymorphisms may play role in susceptibility but not in prognosis of ESCC patients in northernIndian population [56].
Esophageal cancer-related gene 1 (ECRG1) is a novel tumor suppressor gene known to affect matrix remodeling, cell growth, and differentiation. ECRG1 Arg290Gln polymorphism significantly affects the susceptibility but not the prognosis of ESCC patients in low-risk north Indian population [57]. CASP8 IVS12-19 G>A but not CASP8 -652 6N del polymorphism may modulate risk of ESCC and its survival outcome in northern Indian population [58]. GSTP1val/val and CYP2E1c1c2 genotypes/c2 allele increased the risk of ESCC and EADC, respectively, in the Kashmiri population; whereas GSTM3AB genotype imparted lower risk for both ESCC and EADC [59]. NAT2 slow acetylator genotype may increase susceptibility to ESCC, and NAT2 haplotypes (C(481)A(590)G(857) and T(481)A(590)G(857)) may predict susceptibility to Esophageal cancer and Gastric cancer in the Kashmir Valley [60]. COX-2 -765G>C polymorphism confers ESCC susceptibility particularly in females and patients with middle third anatomical location of the tumor. Interaction of COX-2-1195GA and -765C carrier genotypes also modulates ESCC risk [61].
Genetic Polymorphism reported in ESCC from High-risk region of China
Esophageal squamous cell carcinoma (ESCC), one of the leading causes of cancer death worldwide, occurs at a relatively high frequency in China. Genetic variations in the ERCC2 gene were associated with risk of ESCC, and there was a significant interaction between gene polymorphisms and family history of cancer in the etiology of ESCC [62]. Genome-wide association studies of ESCC identified a susceptibility locus in phospholipase C epsilon 1 (PLCE1) in Chinese Han populations, few studies further confirmed these findings in pure Kazakh population in which there are higher incidence and mortality of ESCC. Only 4 SNPs (rs753724, rs11187842, rs2274223, and rs12263737) of PLCE1 confer significantly increased risk of ESCC. The risk effects of rs2274223 of PLCE1 were more evident in poor differentiation and advanced clinical stages of Kazakh ESCC [63]. A significantly decreased risk of ESCC associated with the IL17A rs4711998 A>G polymorphism was evident among younger patients and patients who never smoking or drinking in a Chinese population [64]. The frequency of PIK3CA mutation was higher in female ESCC patients than in males, and higher in patients with non-lymph node metastasis than in patients with lymph node metastasis in Chinese ESCC patients [65]. TGF-β1 RS#1800471G>C polymorphism may be a genetic modifier for developing ESCC in Zhuangese population of China [66]. IL3 rs2073506 G>A polymorphism was associated with an increased risk for ESCC higher TNM stages in Chinese population [67]. Overexpression of HLA-G was a characteristic feature of Kazakh ESCC; HLA-G may be involved in Kazakh ESCC carcinogenesis and HPV infection [68]. CHRNA5-A3-B4 rs667282 TT/TG genotypes were associated with significantly increased risk of ESCC among younger subjects in Chinese population [69]. SMUG1, TDG, TP53, GTF2H3, FEN1, POLQ, HEL308, RAD54B, MPG, FANCE and BRCA1 genes were associated with ESCC in Chinese population [70].
Present Scenario of ESCC in Iran
High intake of nutrients primarily found in plant-based foods is associated with a reduced esophageal cancer risk. Some nutrients such as folate, vitamin E and selenium might play major roles in the etiology of ESCC and their status may eventually be used as an epidemiological marker for esophageal cancer in Iran, and perhaps other high-risk regions [71]. ESCC tumors in people from Golestan Province of Iran show the highest rate of TP53 mutations ever reported in any cancer anywhere. The heterogeneous mutation pattern is highly suggestive of a causative role for multiple environmental carcinogens, including PAHs. The temperature and composition of tea may also influence mutagenesis [72]. Several studies have indicated the association between intake of foods high in dietary glycemic index (GI) and glycemic load (GL) with an increased risk of digestive tract cancers. GI and GL may be associated with risk of esophageal squamous cell carcinoma (ESCC) in a high-risk population in Iran. Diets with high GI and GL might have potentially unfavorable effects on ESCC risk and suggest a possible role for excess circulating insulin and related insulin-like growth factor 1 in esophageal cancer development [73].
Conclusion
Familial clustering of cancer may be a result of shared environmental factors or shared genes by family members. Environmental factors, which are probably the major contributor for the familial aggregation of upper aerodigestive tract cancers,can significantly modify cancer risk in the presence of an inherited cancer-susceptibility gene. The use of high throughput genomic technology in clinical specimens from well characterized populations that have familial clustering of cancer may lead to identification of molecular mechanism associated with progression of esophageal cancer. Functional analyses of these genes Table 1 will lead to betterunderstanding of the development and progression of ESCC.
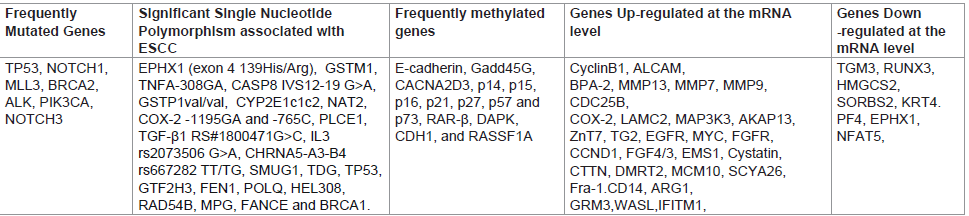
Table 1: Genetic Alterations reported in ESCC.
References
- Murtaza I, Mushtaq D, Margoob MA, Dutt A, Wani NA, et al. (2006) A study on p53 gene alterations in esophageal squamous cell carcinoma and their correlation to common dietary risk factors among population of the Kashmir valley. World J Gastroenterol 12: 4033-4037.
- Katiyar S, Hedau S, Jain N, Kar P, Khuroo MS, et al. (2005) p53 gene mutation and human papillomavirus (HPV) infection in esophageal carcinoma from three different endemic geographic regions of India. Cancer Lett. 218: 69-79.
- Akbari MR, Malekzadeh R, Nasrollahzadeh D, Amanian D, Sun P, et al. (2006) Familial risks of esophageal cancer among the Turkmen population of the Caspian littoral of Iran. Int J Cancer 119: 1047-1051.
- Kumar A, Chatopadhyay T, Raziuddin M, Ralhan R (2007) Discovery of deregulation of zinc homeostasis and its associated genes in esophageal squamous cell carcinoma using cDNA microarray. Int J Cancer 120: 230-242.
- Stoner GD, Gupta A (2001) Etiology and chemoprevention of esophageal squamous cell carcinoma. Carcinogenesis 22: 1737-1746..
- Mir MM, Dar NA, Gochhait S, Zargar SA, Ahangar AG, et al. (2005) p53 mutation profile of squamous cell carcinomas of the esophagus in Kashmir (India): a high incidence area. Int J Cancer 116: 62-68.
- Kashyap MK, Marimuthu A, Kishore CJ, Peri S, Keerthikumar S, et al. (2009) Genome wide mRNA profiling of esophageal squamous cell carcinoma for identification of cancer biomarkers. Cancer Biol Ther 8: 1-11.
- Lee CH, Lee JM, Wu DC, Hsu HK, Kao EL, et al. (2005) Independent and combined effects of alcohol intake, tobacco smoking and betel quid chewing on the risk of esophageal cancer in Taiwan. Int J Cancer 113: 475-482.
- Phukan RK, Ali MS, Chetia CK, Mahanta J (2001) Betel nut and tobacco chewing; potential risk factors of cancer of oesophagus in Assam, India. Br J Cancer 85: 661-667.
- Su H, Hu N, Shih J, Hu Y, Wang QH, et al. (2003) Gene expression analysis of esophageal squamous cell carcinoma reveals consistent molecular profiles related to a family history of upper gastrointestinal cancer. Cancer Res 63: 3872-3876.
- Nyren O, Adami H-O (2002) Esophageal Cancer.): Text Book of Cancer Epidemiology, editors: Hans-Olov Adami, David Hunter, Dimitrios Trichopoulos (Eds), Oxford University Press, 137-155.
- Ghadirian P, (1985) Familial history of esophageal cancer. Cancer 56: 2112-2116.
- Hemminki K, Rawal R, Chen B, Bermejo JL (2004) Genetic epidemiology of cancer: from families to heritable genes. Int J Cancer 111: 944-950.
- Tran GD, Sun XD, Abnet CC, Fan JH, Dawsey SM, et al. (2005) Prospective study of risk factors for esophageal and gastric cancers in the Linxian general population trial cohort in China. Int J Cancer 113: 456-463.
- Akbari MR, Malekzadeh R, Nasrollahzadeh D, Amanian D, Islami F, et al. (2008) Germline BRCA2 mutations and the risk of esophageal squamous cell carcinoma. Oncogene 27: 1290-1296.
- Hemminki K, Li X (2004) Familial risks of cancer as a guide to gene identification and mode of inheritance. Int J Cancer 110: 291-294.
- Hu N, Wang C, Han XY, He LJ, Tang ZZ, et al. (2004) Evaluation of BRCA2 in the genetic susceptibility of familial esophageal cancer. Oncogene 23: 852-858.
- Yang H, Jeffrey PD, Miller J, Kinnucan E, Sun Y, et al. (2002) BRCA2 function in DNA binding and recombination from a BRCA2-DSS1-ssDNA structure. Science 297: 1837-1848.
- Song Y, Zhao C, Dong L, Fu M, Xue L, et al. (2008) Overexpression of cyclin B1 in human esophageal squamous cell carcinoma cells induces tumor cell invasive growth and metastasis. Carcinogenesis 29: 307-315.
- Chang D, Wang TY, Li HC, Wei JC, Song JX (2007) Prognostic significance of PTEN expression in esophageal squamous cell carcinoma from Linzhou City, a high incidence area of northern China. Dis Esophagus 20: 491-496.
- Si HX, Tsao SW, Lam KY, Srivastava G, Liu Y, et al. (2001) E-cadherin expression is commonly downregulated by CpG island hypermethylation in esophageal carcinoma cells. Cancer Lett 173: 71-78.
- Lin YC, Wu MY, Li DR, Wu XY, Zheng RM (2004) Prognostic and clinicopathological features of E-cadherin, alpha-catenin, beta-catenin, gamma-catenin and cyclin D1 expression in human esophageal squamous cell carcinoma. World J Gastroenterol 10: 3235-3239.
- Liu W, Yu ZC, Cao WF, Ding F, Liu ZH (2006) Functional studies of a novel oncogene TGM3 in human esophageal squamous cell carcinoma. World J Gastroenterol 12: 3929-3932.
- Uemura N, Nakanishi Y, Kato H, Saito S, Nagino M, et al. (2009) Transglutaminase 3 as a prognostic biomarker in esophageal cancer revealed by proteomics. Int J Cancer 124: 2106-2115.
- Tanaka E, Hashimoto Y, Ito T, Okumura T, Kan T, et al. ( 2005 ) The clinical significance of Aurora A/STK15/BTAK expression in human esophageal squamous cell carcinoma. Clin Cancer Res 11: 1827-1834.
- Tong T, Zhong Y, Kong J, Dong L, Song Y, et al. (2004) Overexpression of Aurora-A contributes to malignant development of human esophageal squamous cell carcinoma. Clin Cancer Res 10: 7304-7310.
- Hu YC, Lam KY, Law S, Wong J, Srivastava G (2001) Identification of differentially expressed genes in esophageal squamous cell carcinoma (ESCC) by cDNA expression array: overexpression of Fra-1, Neogenin, Id-1, and CDC25B genes in ESCC. Clin Cancer Res 7: 2213-2221.
- Ding MX, Lin XQ, Fu XY, Zhang N, Li JC (2006) Expression of vascular endothelial growth factor-C and angiogenesis in esophageal squamous cell carcinoma. World J Gastroenterol 12: 4582-4585.
- Krzystek-Korpacka M, Matusiewicz M, Diakowska D, Grabowski K, Blachut K, et al. (2007) Up-regulation of VEGF-C secreted by cancer cells and not VEGF-A correlates with clinical evaluation of lymph node metastasis in esophageal squamous cell carcinoma (ESCC). Cancer Lett 249: 171-177.
- Matsumoto M, Natsugoe S, Okumura H, Arima H, Yanagita S, (2006). Overexpression of vascular endothelial growth factor-C correlates with lymph node micrometastasis in submucosal esophageal cancer. J Gastrointest Surg 10: 1016-1022.
- Nozoe T, Ezaki T, Kabashima A, Baba H, Maehara Y (2005) Significance of immunohistochemical expression of cyclooxygenase-2 in squamous cell carcinoma of the esophagus. Am J Surg 189: 110-115.
- Zhi H, Wang L, Zhang J, Zhou C, Ding F, et al. (2006) Significance of COX-2 expression in human esophageal squamous cell carcinoma. Carcinogenesis 27: 1214-1221.
- Fumoto S, Hiyama K, Tanimoto K, Noguchi T, Hihara J, et al. (2009) EMP3 as a tumor suppressor gene for esophageal squamous cell carcinoma. Cancer Lett 274: 25-32.
- Sugiura H, Ishiguro H, Kuwabara Y, Kimura M, Mitsui A, et al. (2008) Decreased expression of RUNX3 is correlated with tumor progression and poor prognosis in patients with esophageal squamous cell carcinoma. Oncol Rep 19: 713-719.
- Shou JZ, Hu N, Takikita M, Roth MJ, Johnson LL, et al. (2008) Overexpression of CDC25B and LAMC2 mRNA and protein in esophageal squamous cell carcinomas and premalignant lesions in subjects from a high-risk population in China. Cancer Epidemiol Biomarkers Prev 17: 1424-1435.
- Morita M, Oyama T, Nakata S, Ono K, Sugaya M, et al. (2006) Expression of FHIT in esophageal epithelium and carcinoma: reference to drinking, smoking and multicentric carcinogenesis. Anticancer Res 26: 2243-2248.
- Li W, Ding F, Zhang L, Liu Z, Wu Y, et al. (2005) Overexpression of stefin A in human esophageal squamous cell carcinoma cells inhibits tumor cell growth, angiogenesis, invasion, and metastasis. Clin Cancer Res 11: 8753-8762.
- Zhi H, Zhang J, Hu G, Lu J, Wang X, et al. (2003) The deregulation of arachidonic acid metabolism-related genes in human esophageal squamous cell carcinoma. Int J Cancer 106: 327-333.
- Wang LS, Chow KC, Wu YC, Lin TY, Li WY (2004) Inverse expression of dihydrodiol dehydrogenase and glutathione-S-transferase in patients with esophageal squamous cell carcinoma. Int J Cancer 111: 246-251.
- Albertson DG (2006) Gene amplification in cancer. Trends Genet 22: 447-455.
- Wu IC, Wu MT, Chou SH, Yang SF, Goan YG, et al (2008) Osteopontin expression in squamous cell cancer of the esophagus. World J Surg 32: 1989-1895.
- . Albertson DG (2006) Gene amplification in cancer. Trends Genet 22: 447-455.
- Pollack JR, Perou CM, Alizadeh AA, Eisen MB, Pergamenschikov A, et al. (1999) Genome-wide analysis of DNA copy-number changes using cDNA microarrays. Nat Genet 23: 41-46.
- Hu N, Roth MJ, Emmert-Buck MR, Tang ZZ, Polymeropolous M, et al. (1999) Allelic loss in esophageal squamous cell carcinoma patients with and without family history of upper gastrointestinal tract cancer. Clin Cancer Res 5: 3476-3482.
- LaFramboise T, Weir BA, Zhao X, Beroukhim R, Li C, et al (2005) Allele-specific amplification in cancer revealed by SNP array analysis. PLoS Comput Biol 1: e65.
- Carneiro A, Isinger A, Karlsson A, Johansson J, Jönsson G, et al. (2008) Prognostic impact of array-based genomic profiles in esophageal squamous cell cancer. BMC Cancer 8: 98.
- Yen CC, Chen YJ, Chen JT, Hsia JY, Chen PM, et al. (2001) Comparative genomic hybridization of esophageal squamous cell carcinoma: correlations between chromosomal aberrations and disease progression/prognosis. Cancer 92: 2769-2777.
- Zhou J, Zhao LQ, Xiong MM, Wang XQ, Yang GR, et al. (2003) Gene expression profiles at different stages of human esophageal squamous cell carcinoma. World J Gastroenterol 9: 9-15.
- Lu J, Liu Z, Xiong M, Wang Q, Wang X (2001) Gene expression profile changes in initiation and progression of squamous cell carcinoma of esophagus. Int J Cancer 91: 288-294.
- Chattopadhyay I, Kapur S, Purkayastha J, Phukan R, Kataki A, et al. (2007) Gene expression profile of esophageal cancer in North East India by cDNA microarray analysis. World J Gastroenterol 13: 1438-1444.
- Chattopadhyay I, Phukan R, Singh A, Vasudevan M, Purkayastha J, et al. (2009) Molecular profiling to identify molecular mechanism in esophageal cancer with familial clustering. Oncol Rep 21: 1135-1146.
- Chattopadhyay I, Singh A, Phukan R, Purkayastha J, Kataki A, et al. (2010) Genome-wide analysis of chromosomal alterations in patients with esophageal squamous cell carcinoma exposed to tobacco and betel quid from high-risk area in India. Mutation Research 696: 130–138.
- Kaushal M, Chattopadhyay I, Phukan R, Purkayastha J, Mahanta J, et al. (2010) Contribution of germ line BRCA2 sequence alterations to risk of familial esophageal cancer in high-risk area of India. Disease of the Esophagus 23: 71-75..
- Ihsan R, Chattopadhyay I, Phukan R, Mishra AK, Purkayastha J, et al. (2010) Role of epoxide hydrolase 1 gene polymorphisms in esophageal cancer in a high-risk area in India. J Gastroenterol Hepatol 25: 1456–1462.
- Sharma A, Das BC, Sehgal A, Mehrotra R, Kar P, et al. (2013) GSTM1 and GSTT1 polymorphism and susceptibility to esophageal cancer in high- and low-risk regions of India. Tumour Biol 34: 3249-3257.
- Umar M, Upadhyay R, Kumar S, Ghoshal UC, Mittal B (2013) Association of Common Polymorphisms in TNFA, NFkB1 and NFKBIA with Risk and Prognosis of Esophageal Squamous Cell Carcinoma. PLoS One 8: e81999.
- . Umar M, Upadhyay R, Kumar S, Ghoshal UC, Mittal B (2013) Modification of risk, but not survival of esophageal cancer patients by esophageal cancer-related gene 1 Arg290Gln polymorphism: a case-control study and meta-analysis. J Gastroenterol Hepatol 28: 1717-1724.
- Umar M, Upadhyay R, Kumar S, Ghoshal UC, Mittal B (2011) CASP8 -652 6N del and CASP8 IVS12-19G>A gene polymorphisms and susceptibility/prognosis of ESCC: a case control study in northern Indian population. J Surg Oncol 103: 716-723.
- Malik MA, Upadhyay R, Mittal RD, Zargar SA, Mittal B (2010) Association of xenobiotic metabolizing enzymes genetic polymorphisms with esophageal cancer in Kashmir Valley and influence of environmental factors. Nutr Cancer 62: 734-742.
- Malik MA, Upadhyay R, Modi DR, Zargar SA, Mittal B (2009) Association of NAT2 gene polymorphisms with susceptibility to esophageal and gastric cancers in the Kashmir Valley. Arch Med Res 40: 416-423.
- Upadhyay R, Jain M, Kumar S, Ghoshal UC, Mittal B (2009) Functional polymorphisms of cyclooxygenase-2 (COX-2) gene and risk for esophageal squmaous cell carcinoma. Mutat Res 663: 52-59.
- Zhang Y, Wang L, Wang P, Song C, Wang K, et al. (2014) Association of single nucleotide polymorphisms in ERCC2 gene and their haplotypes with esophageal squamous cell carcinoma. Tumour Biol Jan 4.
- Cui XB, Chen YZ, Pang XL, Liu W, Hu JM, et al. (2013) Multiple polymorphisms within the PLCE1 are associated with esophageal cancer via promoting the gene expression in a Chinese Kazakh population. Gene 530: 315-322.
- Yin J, Wang L, Shi Y, Shao A, Tang W, et al. (2014) Interleukin 17A rs4711998 A>G polymorphism was associated with a decreased risk of esophageal cancer in a Chinese population. Dis Esophagus 27: 87-92.
- Hou J, Jiang D, Zhang J, Gavine PR, Xu S, et al. (2014) Frequency, characterization, and prognostic analysis of PIK3CA gene mutations in Chinese esophageal squamous cell carcinoma. Hum Pathol 45: 352-358.
- Tang RG, Huang YZ, Yao LM, Xiao J, Lu C, et al. (2013) Polymorphisms of transforming growth factor beta 1 (RS#1800468 and RS#1800471) and esophageal squamous cell carcinoma among Zhuangese population, China. Gene 512: 1-5.
- Zheng L, Yin J, Wang L, Wang X, Shi Y, et al. (2013) Interleukin 1B rs16944 G>A polymorphism was associated with a decreased risk of esophageal cancer in a Chinese population. Clin Biochem 46: 1469-1473.
- Hu J, Li L, Liu Y, Chen Y, Liu C, et al. (2013) Overexpression of HLA-G Is positively associated with Kazakh esophageal squamous cell carcinoma in Xinjiang, China. Viral Immunol 26: 180-184.
- Wang Y, Wu H, Liu Q, Wang C, Fu L, et al. (2013) Association of CHRNA5-A3-B4 variation with esophageal squamous cell carcinoma risk and smoking behaviors in a Chinese population. PLoS One 8: e67664.
- Li WQ, Hu N, Hyland PL, Gao Y, Wang ZM, et al. (2013) Genetic variants in DNA repair pathway genes and risk of esophageal squamous cell carcinoma and gastric adenocarcinoma in a Chinese population. Carcinogenesis 34: 1536-1542.
- Jessri M, Rashidkhani B, Hajizadeh B, Jessri M, Gotay C (2011) Macronutrients, vitamins and minerals intake and risk of esophageal squamous cell carcinoma: a case-control study in Iran. Nutr J 10: 137.
- Abedi-Ardekani B, Kamangar F, Sotoudeh M, Villar S, Islami F,et al. (2011) Extremely high Tp53 mutation load in esophageal squamous cell carcinoma in Golestan Province, Iran. PLoS One 6: e29488.
- Eslamian G, Jessri M, Hajizadeh B, Ibiebele TI, Rashidkhani B (2013) Higher glycemic index and glycemic load diet is associated with increased risk of esophageal squamous cell carcinoma: a case-control study. Nutr Res 33: 719-725.