Case Report
When a TIA is not a TIA: A case report of Cerebral Venous Thrombosis masquerading as Transient Ischemic Attack
Kiran Kuraning, Padmakumar Arayamparambil Vijayan, Garud Suresh Chandan, Pooja Prathapan Sarada and Ganesh KM
Department of Critical Care Medicine Fortis Hospitals, Bannerghatta Main Road, Opposite to IIMB Bengaluru, Karnataka, India
*Corresponding author:Dr Kiran Kuraning, Department of Critical Care Medicine Fortis Hospitals, Bannerghatta Main Road, Opposite to IIMB Bengaluru, Karnataka, India. E-mail Id: kirankuraning@gmail.com
Article Information:Submission: 16/03/2026; Accepted: 28/03/2026; Published: 31/03/2026
Copyright: © 2026 Kuraning K, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Aim and Background: Cerebral venous thrombosis (CVT) is an uncommon subtype of stroke predominantly seen in young adults. Wide spectrum of clinical manifestations of CVT often leads to diagnostic uncertainty and delay in initiating appropriate therapy with anticoagulation.
Case report: We report a case of 34 years old gentleman diagnosed to have cerebral venous thrombosis presenting with recurrent transient unilateral weakness suggestive of Transient Ischemic Attack (TIA). Detailed workup for CVT was not suggestive of any risk factors attributing the cause to be idiopathic.
Clinical Significance: This case report highlights the importance of maintaining a high index of suspicion of CVT In patients with transient focal deficits and persistent headache and utilizing appropriate neuroimaging for accurate diagnosis.
Case report: We report a case of 34 years old gentleman diagnosed to have cerebral venous thrombosis presenting with recurrent transient unilateral weakness suggestive of Transient Ischemic Attack (TIA). Detailed workup for CVT was not suggestive of any risk factors attributing the cause to be idiopathic.
Clinical Significance: This case report highlights the importance of maintaining a high index of suspicion of CVT In patients with transient focal deficits and persistent headache and utilizing appropriate neuroimaging for accurate diagnosis.
Keywords:Cerebral Venous Thrombosis; Transient Ischemic Attack; Stroke; Anticoagulation
Introduction
Cerebral venous thrombosis (CVT) is an uncommon subtype of
stroke. It accounts for approximately 1% of all strokes. CVT is seen
predominantly in young adults. CVT presents with headache, altered
sensorium, seizures, papilledema and rarely focal neurological deficits.
This wide spectrum of clinical manifestations of CVT often leads to
diagnostic uncertainty and delay in initiating appropriate therapy
[1,2]. CVT rarely present as Transient ischemic attack (TIA) due to
fluctuations in intracranial pressure and transient venous congestion
[3]. Such presentation of CVT may misclassify it as arterial stroke
and delays the initiation of anticoagulation which is the mainstay of
treatment in CVT even in the presence of hemorrhagic infarction
[4].
Many times, failure to identify CVT and not considering
suitable imaging modality may lead to inappropriate treatment with
antiplatelet therapy alone and may lead to clinical deterioration. We
report a case of cerebral venous thrombosis presenting with recurrent
transient unilateral weakness suggestive of TIA, highlighting the
importance of maintaining a high index of suspicion and utilizing
appropriate neuroimaging for accurate diagnosis.
Case report
A 34-year-old gentleman with no known comorbidities
presented with complaints of headache for a few days, along with
three episodes of left upper and lower limb weakness over a period of
two days. Each episode lasted approximately 5–10 minutes. During
these episodes, he experienced subjective weakness on the left side,
was unable to bear weight on the left lower limb and had difficulty
holding objects with his left hand. Before and after each episode, he
was neurologically normal.
He initially visited a local clinic, where he was prescribed oral supplements. Due to recurrent episodes of left-sided weakness, he subsequently presented to our hospital. On evaluation in the emergency room (ER), his respiratory and hemodynamic parameters were stable. Central nervous system examination revealed normal motor strength and sensation in all four limbs, with intact sensorium (Glasgow Coma Scale: E4V5M6).
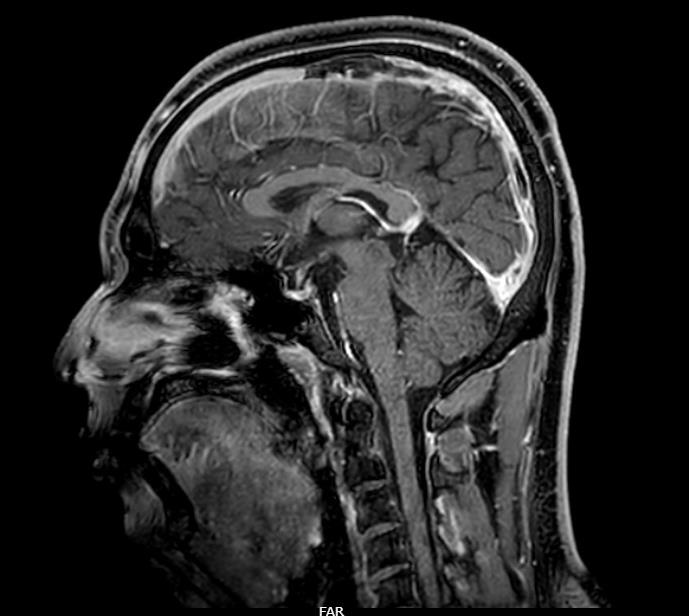
Given the history of transient left-sided weakness and suspicion of stroke, magnetic resonance imaging (MRI) of the brain was performed, which showed no acute abnormalities. In view of persistent headache with normal MRI findings, magnetic resonance venography (MRV) was obtained. MRV demonstrated a filling defect in the superior sagittal sinus, appearing hyperintense on T1-weighted images with loss of flow void on T2-weighted sequences, suggestive of cerebral venous thrombosis (CVT). The patient was subsequently shifted to the Medical Intensive Care Unit (MICU) for further management.
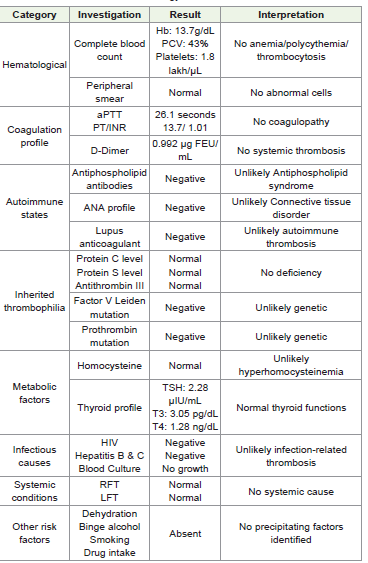
In the MICU, the history was revisited to identify potential risk factors for CVT, including recent diarrhea, vomiting, dehydration, binge alcohol intake, or drug use; none were present. A detailed laboratory workup was performed prior to initiation of therapeutic anticoagulation with low-molecular-weight heparin (enoxaparin 60 mg subcutaneously twice daily). Evaluation for common etiologies was unremarkable (refer to [Table 1]). Cause of CVT in our case was attributed to be idiopathic.
The patient was managed with anticoagulation, intravenous fluids, and antiepileptic therapy. He experienced one additional episode of similar left-sided weakness while in the MICU. Due to concern for possible seizure activity, he underwent 24-hour continuous EEG monitoring, and the antiepileptic dosage was escalated. EEG did not reveal any epileptiform activity. After 48 hours, he was transferred to the ward and was discharged two days later with a plan to bridge
He initially visited a local clinic, where he was prescribed oral supplements. Due to recurrent episodes of left-sided weakness, he subsequently presented to our hospital. On evaluation in the emergency room (ER), his respiratory and hemodynamic parameters were stable. Central nervous system examination revealed normal motor strength and sensation in all four limbs, with intact sensorium (Glasgow Coma Scale: E4V5M6).
Given the history of transient left-sided weakness and suspicion of stroke, magnetic resonance imaging (MRI) of the brain was performed, which showed no acute abnormalities. In view of persistent headache with normal MRI findings, magnetic resonance venography (MRV) was obtained. MRV demonstrated a filling defect in the superior sagittal sinus, appearing hyperintense on T1-weighted images with loss of flow void on T2-weighted sequences, suggestive of cerebral venous thrombosis (CVT). The patient was subsequently shifted to the Medical Intensive Care Unit (MICU) for further management.
In the MICU, the history was revisited to identify potential risk factors for CVT, including recent diarrhea, vomiting, dehydration, binge alcohol intake, or drug use; none were present. A detailed laboratory workup was performed prior to initiation of therapeutic anticoagulation with low-molecular-weight heparin (enoxaparin 60 mg subcutaneously twice daily). Evaluation for common etiologies was unremarkable (refer to [Table 1]). Cause of CVT in our case was attributed to be idiopathic.
The patient was managed with anticoagulation, intravenous fluids, and antiepileptic therapy. He experienced one additional episode of similar left-sided weakness while in the MICU. Due to concern for possible seizure activity, he underwent 24-hour continuous EEG monitoring, and the antiepileptic dosage was escalated. EEG did not reveal any epileptiform activity. After 48 hours, he was transferred to the ward and was discharged two days later with a plan to bridge
parenteral anticoagulation to oral anticoagulants for long-term
therapy.
Discussion
Cerebral venous thrombosis (CVT) is an uncommon but
increasingly recognized cause of stroke in young adults, characterized
by thrombosis of the intracranial venous sinuses and/or cortical veins.
Unlike arterial stroke, CVT has a highly variable clinical presentation,
often leading to diagnostic challenges. Headache is the most common
presenting symptom, reported in up to 80–90% of patients, and may
be the only initial manifestation [1,2]. Our patient presented with
headache followed by recurrent transient focal neurological deficits,
an atypical presentation that closely mimicked transient ischemic
attack (TIA).
Transient focal deficits in CVT are uncommon and may result from transient venous congestion, regional cerebral edema, or fluctuating intracranial pressure rather than true arterial ischemia [3]. Such episodes can resemble TIA, particularly when neuroimaging does not initially reveal parenchymal lesions. In our case, MRI of the brain was normal, and the diagnosis was established only after MR venography demonstrated a filling defect in the superior sagittal sinus. This highlights the importance of venous imaging in patients with transient neurological deficits accompanied by persistent headache or other atypical features.
Transient focal deficits in CVT are uncommon and may result from transient venous congestion, regional cerebral edema, or fluctuating intracranial pressure rather than true arterial ischemia [3]. Such episodes can resemble TIA, particularly when neuroimaging does not initially reveal parenchymal lesions. In our case, MRI of the brain was normal, and the diagnosis was established only after MR venography demonstrated a filling defect in the superior sagittal sinus. This highlights the importance of venous imaging in patients with transient neurological deficits accompanied by persistent headache or other atypical features.
The superior sagittal sinus is among the most frequently involved
sites in CVT [2]. Thrombosis at this location can impair cortical
venous drainage, leading to reversible cortical dysfunction and
transient motor deficits, as observed in our patient. Although seizures
are commonly reported in CVT, the transient weakness in this case
was not associated with epileptiform activity on EEG, supporting a
vascular rather than ictal mechanism.
Identification of underlying risk factors is essential in CVT; however, up to 15–20% of cases remain idiopathic [5] Common predisposing factors include dehydration, infections, prothrombotic states, pregnancy, oral contraceptive use, and systemic inflammatory disorders. No clear precipitating factor was identified in our patient despite extensive evaluation, consistent with idiopathic CVT.
Early diagnosis is critical because the management of CVT differs fundamentally from that of arterial TIA or ischemic stroke. Anticoagulation with heparin remains the cornerstone of therapy, even in the presence of hemorrhagic infarction, and is associated with reduced mortality and improved functional outcomes [4]. Our patient showed clinical stability following initiation of low-molecular-weight heparin, reinforcing the effectiveness of early anticoagulation.
Identification of underlying risk factors is essential in CVT; however, up to 15–20% of cases remain idiopathic [5] Common predisposing factors include dehydration, infections, prothrombotic states, pregnancy, oral contraceptive use, and systemic inflammatory disorders. No clear precipitating factor was identified in our patient despite extensive evaluation, consistent with idiopathic CVT.
Early diagnosis is critical because the management of CVT differs fundamentally from that of arterial TIA or ischemic stroke. Anticoagulation with heparin remains the cornerstone of therapy, even in the presence of hemorrhagic infarction, and is associated with reduced mortality and improved functional outcomes [4]. Our patient showed clinical stability following initiation of low-molecular-weight heparin, reinforcing the effectiveness of early anticoagulation.
This case underscores the need for a high index of suspicion for
CVT in young patients presenting with transient focal neurological
deficits, especially when accompanied by headache and normal initial
MRI findings. Early use of MR venography can facilitate prompt
diagnosis and appropriate management, thereby preventing potential
complications.
Conclusion
Cerebral venous thrombosis can rarely present with transient
ischemic attack–like episodes, leading to diagnostic uncertainty. In
patients with transient focal deficits and persistent headache, early
venous imaging is essential. Prompt recognition and anticoagulation
are key to achieving favorable outcomes.
References
Citation
Kuraning K, Vijayan PA, Chandan GA, Sarada PP. When a TIA is not a TIA: A case report of Cerebral Venous Thrombosis masquerading as Transient Ischemic Attack. Indian J Neurol. 2026;7(1): 164.