Research Article
Linezolid Induced Peripheral Neuropathy in Multidrug Resistant Tuberculosis- A Prospective Observational Study
Maniyar A*, Chheda A, Mahto AP, Chaudhary GS, Jagiasi KA, Ojha PT, Singh RK, Nagendra S,Shah AG, Aipu BK and Bagadia HP
Department of Neurology, Grant Government Medical College and J.J. Hospital, Mumbai, Maharashtra, India
*Corresponding author: Dr. Aamna Maniyar, Department of Neurology, Grant Government Medical College and J.J.
Hospital, Mumbai, Maharashtra, India. E-mail. Id; amaniyar1991@gmail.com
Article Information: Submission: 03/02/2025; Accepted: 05/03/2025; Published: 08/03/2025
Copyright: © 2025 Maniyar A, et al. This is an open access article distributed under the Creative Commons
Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the
original work is properly cited.
Abstract
Background: Linezolid is used for treatment of MDR TB and one of the common adverse effects is peripheral neuropathy. Dose modification or interruption at the onset of peripheral neuropathy can prevent the development of irreversible deficits. We aim to study the clinical features, grade the severity of linezolid induced peripheral neuropathy and effects of dose modification so as to avoid long term deficits.
Methods: MDR TB patients on linezolid treatment who developed peripheral neuropathy were studied. National Cancer Institute Neurosensory Scale was used to grade patients into mild, moderate and severe neuropathy. Mild were continued on linezolid 600 mg, moderate were reduced to 300mg and linezolid was withdrawn for severe neuropathy. Follow up was done regularly and dose modified accordingly. End result was analyzed at 18 months of TB treatment completion.
Results: 84 patients were included in the study. On presentation, 31(36.9%) patients had mild neuropathy, 33 (39.28%) moderate and 20 (23.8%) severe peripheral neuropathies. At the end of 18 months of treatment, linezolid was stopped early in 34 (40.5%) patients and dose reduction to 300mg was done in 50 (59.5%) patients. Final assessment revealed 11(13.09%) patients free from symptoms of peripheral neuropathy, 37 (44.04%) patients had mild, 22 (26.19%) had moderate and 14 (16.6%) had severe peripheral neuropathy.
Conclusion: This study highlights the importance of grading linezolid induced peripheral neuropathy and the need to provide standard guidelines for dose modification to prevent irreversible severe deficits.
Methods: MDR TB patients on linezolid treatment who developed peripheral neuropathy were studied. National Cancer Institute Neurosensory Scale was used to grade patients into mild, moderate and severe neuropathy. Mild were continued on linezolid 600 mg, moderate were reduced to 300mg and linezolid was withdrawn for severe neuropathy. Follow up was done regularly and dose modified accordingly. End result was analyzed at 18 months of TB treatment completion.
Results: 84 patients were included in the study. On presentation, 31(36.9%) patients had mild neuropathy, 33 (39.28%) moderate and 20 (23.8%) severe peripheral neuropathies. At the end of 18 months of treatment, linezolid was stopped early in 34 (40.5%) patients and dose reduction to 300mg was done in 50 (59.5%) patients. Final assessment revealed 11(13.09%) patients free from symptoms of peripheral neuropathy, 37 (44.04%) patients had mild, 22 (26.19%) had moderate and 14 (16.6%) had severe peripheral neuropathy.
Conclusion: This study highlights the importance of grading linezolid induced peripheral neuropathy and the need to provide standard guidelines for dose modification to prevent irreversible severe deficits.
Keywords:Linezolid; Peripheral Neuropathy; Multidrug Resistant TB
Introduction
India accounts for highest number of tuberculosis (TB) cases
in the world. In 2022, 2.8 million TB cases were reported in India
representing 27% of the global burden [1]. Multidrug resistant
(MDR) TB cases have increased by 32% in 2022 compared to 2021
[2]. In 2018, linezolid (LNZ) was included to group A drug and
recommended it to be used for patients with MDR‐TB [3]. It is
given in the dose of 600mg/day for initial 6 months followed by
300mg/day for 18 months in adults above 18 years with MDR TB.
However, adverse events are common with courses longer than one
month, affecting over 80% of patients in some studies [4]. Peripheral
neuropathy is a common adverse effect with risks of deficits which
are often irreversible [5]. Recently, CDC has provided guidelines
for dosing modification or interruption of Linezolid based on the
adverse reactions [6]. In our study, patients on linezolid for MDR
TB who complained of pain/ paresthesias for more than 7 days were
considered of having peripheral neuropathy. We need to objectively
grade the severity of neuropathy and guide on reducing dose or
withdrawing the drug accordingly to avoid long term deficits.
We aim to study the clinical manifestations of linezolid
induced peripheral neuropathy in patients with Multidrug resistant
Tuberculosis and to follow up and assess the effects of standard
drug tapering or withdrawal on long term deficitsat18 months of
tuberculosis treatment completion.
Methods
A prospective observational study was done in the Department of
Neurology of a tertiary care centrein western Maharashtra. Patients
with MDR TB were enrolled for one year (July 2021 to June 2022) and
each patient was followed up for 18 months. The duration including
analysis period was 3 years and was completed in December 2023.
MDR TB was diagnosed on the basis of sputum examination, FNAC
in case of lymphadenopathy, CSF study, clinical and radiological
features.
Inclusion Criteria: Patients above 18 years diagnosed with
Multidrug resistant Tuberculosis and started on treatment with Bed
aquiline based all oral regimenthat contains Linezolid in dosage of
10mg/kg/day or maximum dose of 600mg/day developing peripheral
neuropathy were included in the study.
Exclusion Criteria:Patients with pre-existing peripheral
neuropathy secondary todiabetes mellitus, chronic liver disease,
chronic kidney disease, positive serology for HIV, Hepatitis B and C,
pregnancy or lactation were excluded
Data Collection:
MDR TB patients on linezolid treatment presenting to outpatient
of Neurology Department with neuropathic symptoms, fulfilling
the inclusion criteria were enrolled in the study. All information
were collected in a standardized evaluation form. On presentation
demographic characteristics including age, sex, weight, height,
body mass index (BMI) was recorded. Detailed clinical neurological
evaluation was done along with nerve conduction studies (NCS).
Common nutritional causes of peripheral neuropathy were ruled out
by testing for serum vitamin B12, folic acid and mean corpuscular
volume (MCV) levels.
Based on the National Cancer Institute Neurosensory Scale,
peripheral neurotoxicity is divided into 4 grades:Grade 1: Mild paresthesias, loss of deep tendon reflexes
Grade 2: Moderate paresthesias, mild to moderate objective sensory loss
Grade 3:Paresthesias interfering with function, severe objective sensory loss
Grade 4: Permanent sensory loss that impairs function.
Grade 2: Moderate paresthesias, mild to moderate objective sensory loss
Grade 3:Paresthesias interfering with function, severe objective sensory loss
Grade 4: Permanent sensory loss that impairs function.
Using these grades, patients were divided into mild neuropathy
(Grade 1), moderate neuropathy (Grade 2) and severe neuropathy
(Grade 3 and 4).
As per our institute’s center of care guidelines, those with mild
neuropathy were continued on same dose linezolid of 600mg/
day and after completion of 6 months of treatment, dosage was
reduced to 300mg. Immediate dose reduction to 300mg/day was
done for moderate neuropathy and linezolid was withdrawn for
severe neuropathy. All patients were treated with oral neuropathic
agents (gabapentin, duloxetine) with oral pyridoxine, benfotiamine
and mecobalamin supplementation though vitamin B12 levels were
normal. Follow up was doneregularly as and when required and dose
of linezolid was modified at each visit after grading the neuropathy.
End result was analysed at 18 months of TB treatment completion.
Informed consent was taken for each case and approval of
Institutional Ethics committee was taken.
Results
Statistical analysis of the data was performed using SPSS 23.0.
Categorical data was represented in the form of frequency and
percentage. Descriptive statistics was expressed using mean and
standard deviation. Chi square test was used as test of significance
and a p value of <0.05 was considered as statistically significant.
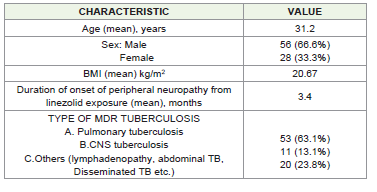
We studied 84 MDR TB patients with linezolid induced peripheral
neuropathy. There was a high preponderance of females 56 (66.6%)
as compared to males 28 (33.3%). The mean age of patients was 31.2
years. Peripheral neuropathy developed after a mean duration of 3.4
months of linezolid treatment. Mean body mass index (BMI) was 20.67
kg/m2. 32 (38%) patients had low BMI of which moderate and severe
neuropathy was present in 12 patients each. There was statistically
significant association between development of severe peripheral
neuropathy and low BMI (p value= 0.015). Neuropathic symptoms
were reported within 2 months in 19 (22.6%), between 2 to 4 months in
46 (54.7%) and beyond 4 months in 19 (22.6%) patients after starting
linezolid. Out of the 19 patients who developed symptoms within 2
months of exposure, 2 patientsdeveloped symptoms as early as 21
days. 9 (10.7%) patients had asymmetrical onset of deficits, remaining
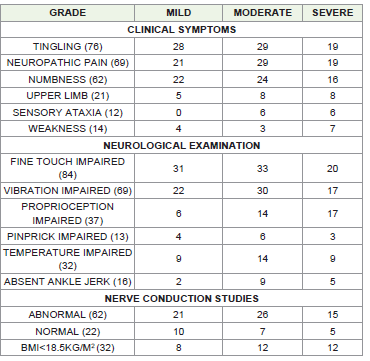
75 (89.3%) patients had a symmetrical presentation. Most common
clinical symptom was lower limb tingling paresthesias present in 76
(90.5%) patients followed by neuropathic pain and numbness present
in 69 (82.14%) and 62 (73.8%) patients respectively. Other symptoms
included upper limb complaints, weakness and sensory ataxia present
is 21 (25%), 14 (16.6%) and 12 (14.3%) patients respectively. Sensory
examination revealed impaired fine touch as the predominant finding
seen in all 84 (100%) patients followed by impaired vibration in 69
(82.1%) patients. Other findings were impaired joint position sense,
temperature and pin prick seen in 37 (44%), 32 (38%) and 13 (15.5%)
patients respectively. Reflex examination revealed absent ankle jerks
in 14(16.6%) patients. Nerve conduction studies was abnormal in
62(73.8%) patients. Axonal neuropathy was found in 58 patients and
4 patients had mixed demyelinating with axonal neuropathy while
remaining 22 (26.2%) cases had normal NCS findings.
On presentation, 31(36.9%) patients had mild neuropathy, 33
(39.28%) moderate and 20 (23.8%) severe peripheral neuropathies.
After monthly followups, the dosage of linezolid was modified
according to the severity of neuropathy. Patients were finally assessed
at 18 months of TB treatment completion.
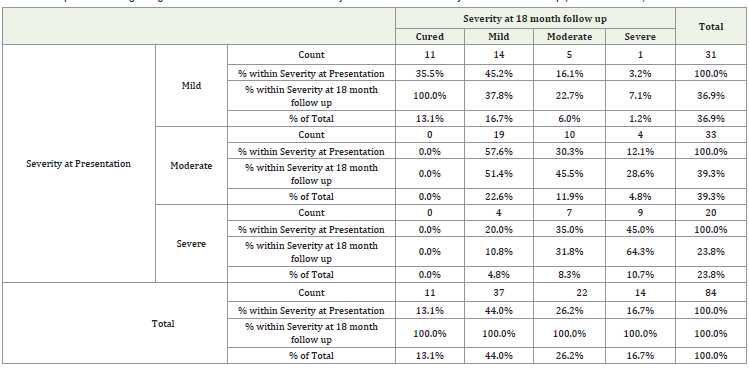
The cross-tabulation analysis presents the relationship between
the severity of patients’ conditions at presentation and their severity
at an 18-month follow-up. The results highlight how initial severity
impacts long-term outcomes, with significant variations observed
across different severity levels.
For patients who presented with mild neuropathy, 35.5% were
cured at the 18-month follow-up, 45.2% had mild severity, 16.1% had
moderate severity, and 3.2% had severe neuropathy. These patients
constituted 36.9% of the total sample, demonstrating that the majority
either remained mild or improved.
In the moderate group at presentation, none were cured after
18 months. However, 57.6% remained mild, 30.3% had moderate
severity, and 12.1% progressed to severe neuropathy. This group
made up 39.3% of the total sample, showing a significant proportion
experiencing persistent or worsened conditions.
For those initially presenting with severe neuropathy,
20.0%improved to mild, 35.0% had moderate severity, and 45.0%
remained severe. These patients accounted for 23.8% of the total
sample, indicating a substantial challenge in achieving improvement
within this group. Out of 4 patients with mixed demyelinating and
axonal neuropathy, 2 belonged to mild group and remained with
mild symptoms at 18 months, 1 worsened from moderate to severe
group and 1 improved from severe to mild group.
At the end of 18 months of treatment, linezolid was stopped early
in 34 (40.5%) patients and dose reduction to 300mg was done in 50
(59.5%) patients. Final assessment revealed 11(13.09%) patients free
from symptoms of peripheral neuropathy, 37 (44.04%) patients had
mild, 22 (26.19%) had moderate and 14 (16.6%) had severe peripheral
neuropathy. Of the 14 (16.6%) patients who had persistent severe
deficits at 18 months, 9 were from severe group, 3 from moderate and
only 2 from mild group.
Discussion
The exact mechanism of linezolid induced peripheral neuropathy
is not fully understood. It may involve mitochondrial dysfunction
and autophagy inhibition leading to axonal damage, impaired
mitochondrial protein synthesis, loss of neurons and myelin sheath.
Some individuals may be more susceptible to developing linezolid
neuropathy due to genetic factors [7]. Linezolid induces large fibre
neuropathy evidenced by reduction in sensory nerve action potentials
on NCS. However, 26.2% patients had normal NCS findings. Detailed
analysis of symptoms revealed prevalence of neuropathic pain in
82.14% of patients indicating that small diameter sensory nerves may
degenerate early in the course causing small fibre neuropathy[8].
According to literature, the prescribed daily dose of linezolid
ranges from 300mg to 1200mg. Adverse effects have found to be
linearly correlated with dosage. A daily dose of 1200mg is reported to
be associated with peripheral neuropathy in more than 80% patients
[9]. Lower dose of 300mg causes less toxicity, but its prolonged
exposure has risk of acquired drug resistance [10,11]. To optimize
the efficacy and safety, a daily dose of 600 mg for 12–18 months is
recommended by WHO for MDR TB.
In our study National Cancer Institute Neurosensory Scale
is used to grade the severity of peripheral neuropathy. It is an
extrapolation from cancer treatment related peripheral neuropathy as
linezolid is also a toxin and causes peripheral nerve involvement due
to mitochondrial cell injury [11]. This scale helped us in classifying
patients into mild, moderate and severe peripheral neuropathy and
thereby deciding on linezolid dosage modification. Our patients
initially received 600mg of linezolid. After dose modification at
regular follow up, 49 received 300mg linezolid till 18 months of
treatment completion.
Regular follow up with monitoring is important for timely
identification of cases worsening towards severe neuropathy where
immediate linezolid withdrawal is crucial. Inspite of frequent
monitoring and immediate linezolid withdrawal, 14 (16.6%) patients
in our study had severe residual deficits at 18 months follow up.
This highlights that linezolid induced peripheral neuropathy can
be irreversible. There are various studies reporting irreversibility of
linezolid induced peripheral neuropathy [11-14].
In terms of duration of linezolid exposure, he observed that
peripheral neuropathy was diagnosed after a mean duration of
3.4 months of linezolid exposure. This is similar to study done in
China where peripheral neuropathy occurred 2 to 4 months after
treatment initiation [15]. However, in our study19 patients developed
neuropathy within 2 months of exposure.
On studying the demographic characteristics, we found that
32 (38%) patients had low BMI. Though we found an association
of development of peripheral neuropathy with low BMI, other
parameters to evaluate malnutrition as the predisposing factor have
to assessed.
Jaspard M et al.[14] diagnosed peripheral neuropathy based
on nerve conduction study in 72% cases. In our study, evidence of
neuropathy on NCS was found in 73.8% cases whereas 26.2% had
normal NCS. This could be due to small fibre involvement, early
testing, lack of age appropriate NCS cutoff values. However, all
patients had clinical symptoms and signs of peripheral neuropathy
on diagnosis indicating that clinical neurological examination can
be effectively used to screen for peripheral neuropathy even if NCS/
EMG facility is not available.
Health care providers in TB centers should be trained regarding
peripheral neuropathy examination. Definite guidelines need to be
provided for grading the neuropathy and implementing linezolid
dose reduction and withdrawal as done in our study. This will endow
decision making to primary caregivers where Neurology services
like Neurophysician, NCS facility are not available and will help in
avoiding development of severe irreversible neurodeficits.
Limitations:
Some limitations of this study are inherent as it is monocentric with
small sample size. Confounding factors play a role in development of
linezolid induced neuropathy such as anemia, vitamin B12 and other
nutritional deficiencies, other drugs in regimen used to treat MDRTB
which could not be completely eliminated in our study. Relation
of LNZ induced neuropathy with serum concentrations of LNZ could
not be studied. Long term follow up is needed to know the outcome of
peripheral neuropathy in these patients beyond 18 months.Conclusion
In this study including linezolid induced peripheral neuropathy
in MDR TB patients, we highlight the importance of grading the
neuropathy based on severity at presentation which appropriately
guides in linezolid dose reduction and withdrawal. Regular follow
up with monitoring is important for timely identification of cases
worsening towards severe neuropathy where immediate linezolid
withdrawal is crucial in preventing irreversible severe neurodeficits.
Clinical neurological examination should be used by medical
personals across all TB centers for early diagnosing peripheral
neuropathy. Proposal of definite guidelines for grading the severity of
neuropathy shall guide them regarding linezolid dose modification.
Further detailed studies are required in identifying various risk factors
involved in causing linezolid induced peripheral neuropathy so as to
decrease the rate of development of neuropathy without affecting the
multidrug resistant TB outcomes.
References
Citation
Maniyar A, Chheda A, Mahto AP, Chaudhary GS, Jagiasi KA, et al. Linezolid Induced Peripheral Neuropathy in Multidrug Resistant
Tuberculosis- A Prospective Observational Study. Indian J Neurol. 2025;6(1): 142.