Case Report
Acute Pan-Cerebellar Syndrome in a Patient with Newly Diagnosed Chronic Kidney Disease
Ramachandran MohanRaj*, Lenin Sankar Palanisamy and Ravikumar Veeramani
Department of Neurology, Thanjavur Medical College, Thanjavur, Tamil Nadu, India
*Corresponding author:Ramachandran Mohan Raj, Department of Neurology, Thanjavur Medical College, Thanjavur, Tamil Nadu, India. E-mail Id: mrama248@gmail.com
Article Information:Submission: 09/01/2025; Accepted: 10/02/2025; Published: 15/02/2025
Copyright: © 2025 MohanRaj R, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Neurological manifestations of chronic kidney disease are due to various reasons and one among them is inefficient elimination of toxins by the kidneys. The neurological manifestations can involve both central and peripheral nervous systems. It ranges from severe encephalopathy, coma to sensorimotor peripheral neuropathy. However, cerebellar manifestations in CKD per se is rare, though it can occur if any predisposing factors are there. Here, we report a case of acute pan-cerebellar syndrome in newly diagnosed CKD patient who took isoniazid prophylaxis for contact with open tuberculosis.
Keywords:Chronic Kidney Disease; Cerebellar Syndrome; Isoniazid
Introduction
Chronic Kidney Disease is associated with several neurological
manifestations. It includes progressive cognitive decline,
peripheral neuropathy, movement disorders, sleep disturbance,
delirium, seizures,and metabolic encephalopathy leading to
coma and death. Postulated mechanisms for these manifestations
are due to accumulation of toxic organic acids in the CNS or to
direct effects on the CNS of parathyroid hormone. But there are
no direct cerebellar manifestations in CKD unless there are some
predisposing factors.
Among anti-tubercular drugs, Isoniazid is known for its
neurotoxicity and hepatotoxicity. Neurotoxicity generally
manifests as peripheral neuropathy which is usually mild and
reversible. In this report, we present a newly diagnosed CKD
patient who developed rare central nervous system complication
following isoniazid prophylaxis.
Case Report
A 60-year-old-woman admitted in our intensive care unit
with history of giddiness for 2 days followed by vomiting and
acute onset of slurring of speech, unsteadiness while sitting and
walking with excessive sleepiness since the night before the day
of admission. There was no history of fever, diarrhea, headache,
visual disturbance, and motor weakness. No history of seizures
altered sensorium and loss of consciousness. She didn’t have any
significant past medical and surgical history. She took isoniazid
prophylaxis for 5days, started to her because her husband
was recently diagnosed to have sputum positive pulmonary
tuberculosis.
On examination, patient was drowsy, arousable to call and
oriented to time, place, and person. She obeyed all commands.
Her vitals were stable with mild hypertension (admission BP was
150/90mmHg). On neurological examination, she was drowsy
and arousable to call and oriented to time, place, and person. Her
language was normal with cerebellar type of dysarthria.Cranial
nerve examinations showed normal fundus with no extra-ocular
movement abnormalities. Motor power was normal and sensory
examinations were also normal. No evidence of extra-pyramidal
and autonomic involvement. She had gross stance and gait ataxia
with impaired rapid alternative movements and incoordination
in both upper and lower limbs.There were no generalized
lymphadenopathies, pedal edema, or hepatosplenomegaly.
Breast examination was normal. Clinically she was suspected
to have posterior circulation stroke with localisation to pancerebellar
involvement and hence the treatment was started for
the same.
She was evaluated for above mentioned complaints and
findings. Her complete blood count showed hemoglobin of 9.5g/
dl, total leucocyte count of 10,930/cu.mm and platelet count of
2.23L/cu.mm. The renal function tests revealed serum urea of
75mg/dl and creatinine of 2.9mg/dl with creatinine clearance
of 16ml/min and eGFR of 18ml/min/1.73m2. The serum
sodium was 142mmol/l and serum potassium were 3.7mmol/l.
Ultrasound abdomen showed bilateral contracted kidney. CT
abdomen showed also showed bilateral contracted kidney. CT
chest was normal. Electrocardiogram and Echocardiogram was
normal. Her CSF analysis were unremarkable with JE negative.
Serum JE, IgM dengue, IgM Scrub typhus and CBNAAT were also
negative.
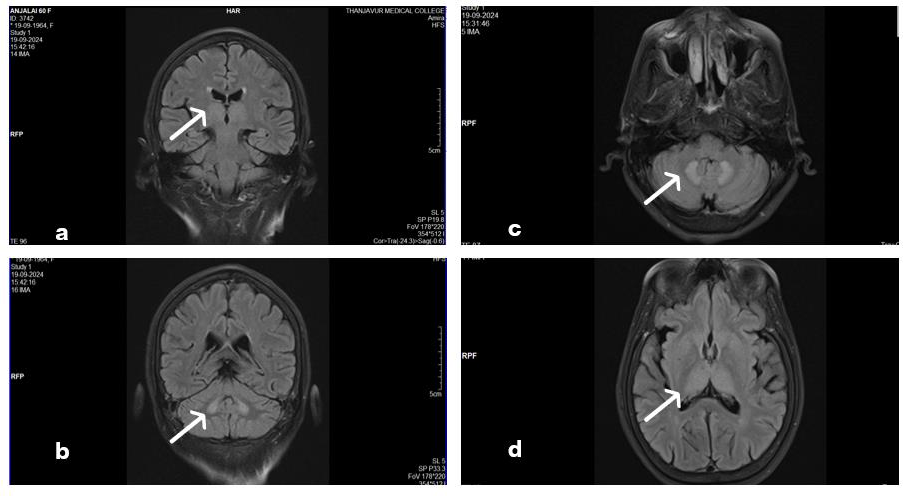
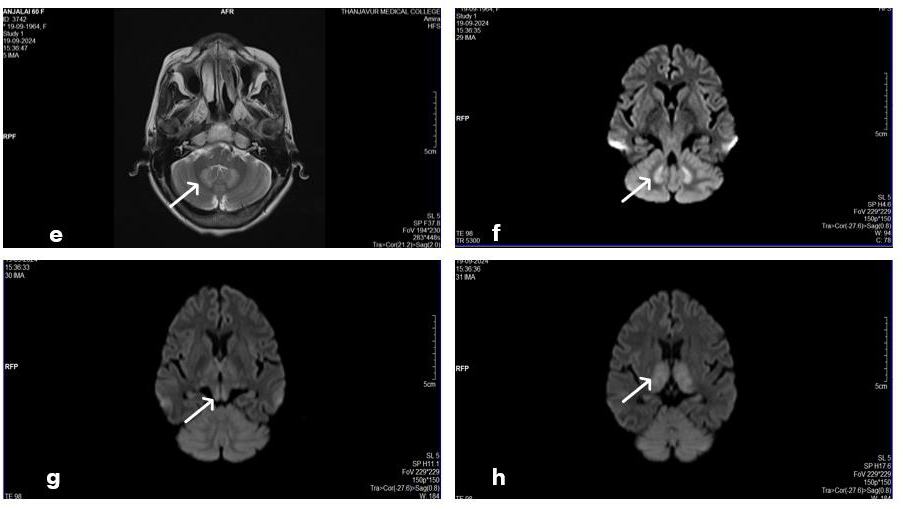
Neuroimaging namely MRI of Brain was carried out which
showed bilateral symmetrical T2/FLAIR hyperintensities in
dentate nucleus and thalamus with mild diffusion restrictions
and rest of the brain parenchyma was normal. MR angiogram and
venogram was also normal. Carotid-vertebral artery doppler was
also normal.
As there were no other etiologies for acute onset pancerebellar
syndrome, patient was re-questioned about the count
of tablets of INH taken and she broke the ice with history of
intake of isoniazid tablets of 100mg each for 3times a day for
5days prior to admission. Through the process of diagnosis of
exclusion, we made the possible diagnosis of isoniazid induced
cerebellar toxicity, which is also described in literature especially
in CKD patients. Patient improved in a week time after treatment
with high dose pyridoxine [1-5].
Discussion
Isoniazid is the first line anti-tubercular drug with bactericidal
activity. The usual dose in the fixed dose combination of current
ATT regimen is 75mg. INH interferes with pyridoxine metabolism
resulting in deficiency of this vitamin. Adverse effects due to INH
occur in 5% of patients even with adequate dose of pyridoxine
supplementation. The most common Neurological Adverse Drug
reaction of INH is that of sensorimotor peripheral neuropathy
which is mild and usually reversible. Due to its metabolism in
liver, no dosage adjustment is needed for patients with renal
disease. It is well tolerated in CKD patients and when toxicity
occurs, it is related to hepatotoxicity.
CNS toxicity due to INH and its metabolite isonicotinylhydrazide,
causing encephalopathy and seizures has been documented, but
cerebellar manifestations are very rare. Cerebellar toxicity occurs
due to reduced GABA and down regulation of NMDA receptors,
with resultant edema of the dentate nucleus. Since the main route
of elimination of INH is through kidneys, in CKD patients, there is
high chance of accumulation of its toxic metabolite and causing
neurotoxicity.
Neuroimaging findings in INH induced cerebellitis include
bilateral symmetrical T2/FLAIR hyperintensities in dentate
nucleus because of edema. Similar imaging findings are
document in metronidazole toxicity, arboviral and enteroviral
infections, maple syrup urine disease and metabolic disorders
like Wernicke’s encephalopathy and hypoparathyroidism. In our
patient, it is not isolated involvement of dentate nucleus but also
thalamus and midbrain involved which rare in INH toxicity.
Association between initiation of therapy and onset of
symptoms should give us the diagnosis of INH toxicity related
cerebellitis.
Conclusions
INH induced cerebellar toxicity should be kept in differential
diagnosis in the case of bilateral dentate nucleus hyperintensities,
though metronidazole is the common one. In the background
of renal impairment, INH can cause cerebellar syndrome apart
from other CNS manifestations. Early diagnosis and intervention
like dose modification and pyridoxine supplementations will
preventive morbidity.
References
Citation
MohanRaj R, Palanisamy LS, Veeramani R. Acute Pan-Cerebellar Syndrome in a Patient with Newly Diagnosed Chronic Kidney Disease. Indian J Neurol. 2025;6(1): 141.