Research article
Role of Whole Brain Radiotherapy in Patients of Primary Central Nervous Lymphoma in the Era of High Dose Methotrexate-Based Chemotherapy – A Single Institution Retrospective Audit
Yadav BS* and Gade VKV
Department of Radiotherapy and Oncology, Post Graduate Institute of Medical Education and Research, Chandigarh, India.
*Corresponding author:Budhi Singh Yadav, Department of Radiotherapy and Oncology, Post Graduate Institute of Medical Education and Research, Chandigarh, India.
Article Information: Submission: 15/01/2025; Accepted: 07/02/2025; Published: 14/02/2025
Copyright: © 2025 Yadav BS, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction: Primary central nervous system lymphoma (PCNSL) is an aggressive form of non-Hodgkin lymphoma that primarily affects the brain and its surrounding structures. The introduction of high-dose methotrexate-based chemotherapy (HD-MTX) has led to more individualized treatment approaches based on patient and disease characteristics.
Materials and Methods: This retrospective audit was conducted at a tertiary care center in Northern India for PCNSL patients treated between 2015 to 2024. Patient records were anonymized and variables such as age, sex, performance status, comorbidities, and disease characteristics were recorded. Treatment details included chemotherapy regimens and radiotherapy techniques. Survival outcomes were analyzed using Kaplan-Meier methods and univariate and multivariate analyses were performed to identify prognostic factors.
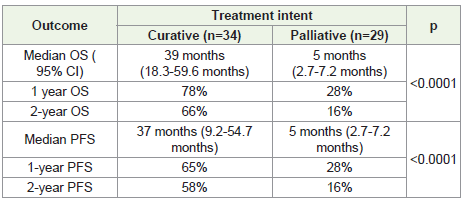
Results: The study cohort comprised 63 patients, 34 patients treated with curative intent and 29 with palliative intent. The mean age of the patients was 54.2 years. Histology was diffuse large B-cell lymphoma in all patients exceptin one with plasmablastic lymphoma. Among the patients treated with curative intent, 55.8% received HD-MTX-based chemotherapy and WBRT, while 32.3% received HDMTX chemotherapy alone. Median overall survival (OS) and progression-free survival (PFS) in patients treated with curative intent and palliative intent was 39 months vs. 5 months (p<0.0001), and 37 months vs. 5 months (p<0.0001), respectively. On univariate analysis poor performance status at diagnosis was a significant predictor of worse survival outcomes (p<0.00001). In patients receiving WBRT, neurological function scale (NFS) improved in 8.5%, remained stable in 82.5%, and worsened in 21.3%. Importantly, no correlation was found between the delivery of radiotherapy and changes in NFS (p=0.08).
Conclusion: This audit demonstrates that WBRT remains an important component of PCNSL management along with HD-MTX regimen. Despite advancements in chemotherapy, WBRT continues to play a crucial role in consolidating treatment outcomes for PCNSL patients.
Materials and Methods: This retrospective audit was conducted at a tertiary care center in Northern India for PCNSL patients treated between 2015 to 2024. Patient records were anonymized and variables such as age, sex, performance status, comorbidities, and disease characteristics were recorded. Treatment details included chemotherapy regimens and radiotherapy techniques. Survival outcomes were analyzed using Kaplan-Meier methods and univariate and multivariate analyses were performed to identify prognostic factors.
Results: The study cohort comprised 63 patients, 34 patients treated with curative intent and 29 with palliative intent. The mean age of the patients was 54.2 years. Histology was diffuse large B-cell lymphoma in all patients exceptin one with plasmablastic lymphoma. Among the patients treated with curative intent, 55.8% received HD-MTX-based chemotherapy and WBRT, while 32.3% received HDMTX chemotherapy alone. Median overall survival (OS) and progression-free survival (PFS) in patients treated with curative intent and palliative intent was 39 months vs. 5 months (p<0.0001), and 37 months vs. 5 months (p<0.0001), respectively. On univariate analysis poor performance status at diagnosis was a significant predictor of worse survival outcomes (p<0.00001). In patients receiving WBRT, neurological function scale (NFS) improved in 8.5%, remained stable in 82.5%, and worsened in 21.3%. Importantly, no correlation was found between the delivery of radiotherapy and changes in NFS (p=0.08).
Conclusion: This audit demonstrates that WBRT remains an important component of PCNSL management along with HD-MTX regimen. Despite advancements in chemotherapy, WBRT continues to play a crucial role in consolidating treatment outcomes for PCNSL patients.
Keywords:Primary Central Nervous System; Lymphoma; Chemotherapy; Radiotherapy
Introduction
Primary central nervous system lymphoma (PCNSL) is a rare,
aggressive non-Hodgkin lymphoma that primarily affects the brain,
eyes, spinal cord, and meninges. It accounts for up to 4% of intracranial
tumors in immunocompetent individuals, with a higher incidence in
elderly men and White populations [1]. Incidence has risen since
the 1960s with increased prevalence among immunocompromised
individuals, particularly those with HIV, organ transplants, or
autoimmune diseases requiring immunosuppression [2]. Diffuse
large B-cell lymphoma is the most common subtype, although
T-cell variants are also observed [3]. It commonly occurs in the
periventricular white matter, basal ganglia and corpus callosum and
can infrequently involve the cerebellum and brainstem [4].
Before the introduction of high-dose chemotherapeutic regimens,
whole-brain radiotherapy (WBRT) was the standard treatment.
Currently, treatment decisions are individualised based on patientrelated
factors such as age, performance status and comorbidities and
disease-related factors like neurological function, size and extent of the
disease. Patients eligible for curative treatment receive chemotherapy
with high-dose methotrexate (HD-MTX)-based regimens, followed
by an assessment for consolidation with WBRT. Other options for
consolidation include cytosine arabinoside and autologous stem cell
transplant. Unfit patients are usually treated with WBRT alone [5-7].
In this article, we present a single institutional experience of PCNSL
patients diagnosed and treated over the last decade.
Materials and Methods
This is a retrospective single institutional audit conducted in a
large tertiary care centre in Northern India. Departmental ethical
clearance was obtained. Records of patients with PCNSL registered in
the Department of Radiotherapy and Oncology from 2015-2024 were
retrieved. Patient identifiers such as name and address were masked
for the purpose of the study. Patient related variables entered in to the
data included age, sex, performance status and comorbidities. Disease
related variables included site, size, number of lesions, histology
and molecular subtype. Treatment related variables included
baseline investigations, surgery, radiotherapy and chemotherapy.
Radiotherapy details included the dose fractionation regimen and
the technique of radiotherapy. Chemotherapy details included the
regimen and number of cycles .Various prognostic indices such as
Charlson’s Comorbidity index, IELSG score, MSKCC RPA score and
the 3F score were calculated [8,9].
Study related variables were entered into SPSS v25 (Statistical
package for social sciences – IBM). Patients treated with curative
and palliative intent were analysed separately. Descriptive data was
generated for variables in the study. Independent samples T-test
was used to analyse normally distributed continuous data and Mann
Whitney U test was used to analyse non-normal continuous data.
Chisquare and Fischer’s exact test were used to compare categorical
variables in both the groups. Overall survival (OS) was calculated
from the date of diagnosis to the date of death due to any cause or the
time of last follow up. Progression free survival (PFS) was calculated
from the date of diagnosis to the date of progression or death. Survival
analysis was done by Kaplan-Meir method. Univariate analysis of the
factors affecting survival was performed with the log rank test and
multivariate analysis was done with the Cox regression analysis.
Results
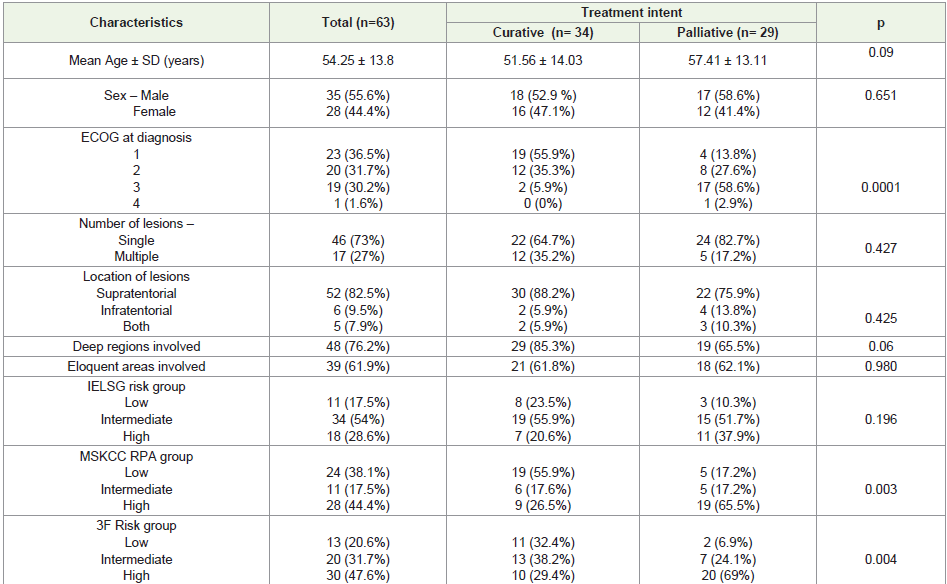
Baseline characteristics:
A total of 63 patients were included in the analysis. Thirty-four
patients were treated with curative intent and 29 patients were
treated with palliative intent [Table 1]. The mean age of the patients
was 54.2 ± 13.8 years. The gender distribution was similar across
both the groups. All patients had a negative serology for HIV and
Hepatitis B, whereas one patient was positive for Hepatitis C virus.
Among 20 patients with poor performance status (ECOG 3-4), two
received treatments with curative intent, while 18 received palliative
treatment. Total 46(73%) of the patients had a single lesion and
52(82.5%) of patients had lesions in the supratentorial location. On
histology 62 patients had diffuse large B-cell lymphoma and one
patient had plasmablastic lymphoma. Molecular subtyping was not
available for 29 patients. Three patients belonged to the GCB subtype
and 31 patients belonged to non-GCB subtype. On risk stratification,
18(28.6%), 28(44%) and 30(47.5%) of patients belonged to the highrisk
group as per the IELSG, MSKCC RPA and 3F scoring systems,
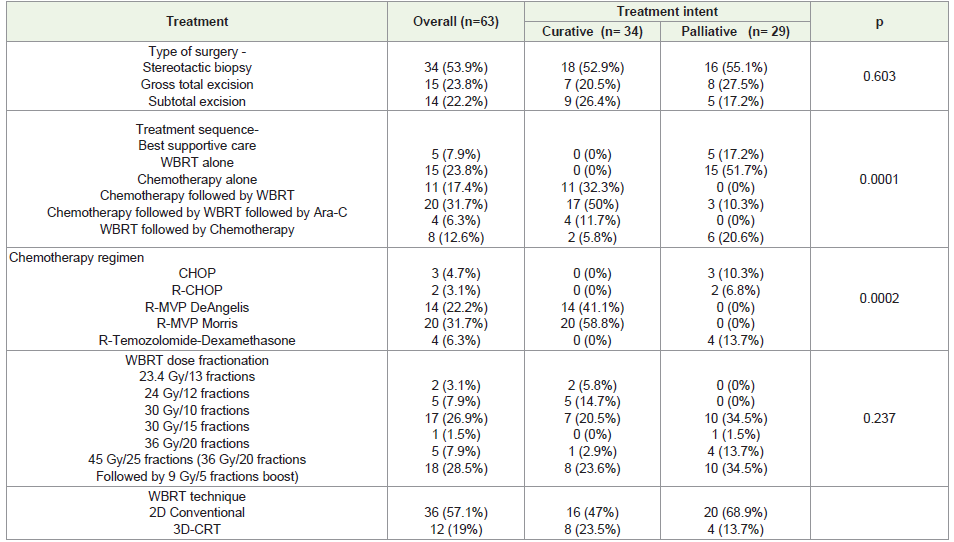
respectively.Treatment detail:
In patients treated with curative intent, 17(50%) received
chemotherapy followed by WBRT, 11(32.3%) received chemotherapy
alone and 4(11.7%) received chemotherapy followed by WBRT and
cytosine arabinoside consolidation [Table 2]. Two patients with
performance status of ECOG 3 were treated with WBRT followed
by HD-MTX-based chemotherapy in view of marked improvement
in their performance status. These patients were considered as being
treated with curative intent. In patients treated with curative intent,
14(41.1%) of patients received HD-MTX-based chemotherapy with
R-MVP DeAngelis regimen and 20(58.8%) received R-MVP Morris
regimen. In those treated with palliative intent, 5(17.3%) received best
supportive care, 15(51.7%) received WBRT alone, 3(10.3%) received
chemotherapy followed by WBRT and 6(20.6%) received WBRT
followed by chemotherapy. The chemotherapeutic regimens used
included R-CHOP 2(6.8%), CHOP 2(10.3%) and R-Temozolomide-
Dexa 4(13.7%).For WBRT, radiotherapy technique was fluoroscopy guided
2 dimensional (2D)and 3D conformal radiotherapy (3D-CRT) in
36(57%) and 12(19%) patients, respectively. In patients who received
HD-MTX-based chemotherapy, 7(20.5%) patients received reduced
dose WBRT (23.4 Gy in 13 fractions or 24 Gy in 12 fractions) after
having achieved complete response. Nine (26.5%) patients with a
partial response received WBRT with definitive intent (36-45 Gy at
1.8 Gy/#). Seven (20.5%) patients received 30 Gy in 10 fractions –
5(14.7%) of them had stable or progressive disease after high-dose
chemotherapy and 2(5.8%) received WBRT upfront. After WBRT,
14 (41%) of patients achieved complete remission. Among those
treated with palliative intent, WBRT was delivered in doses ranging
from 30 Gy in 10 fractions to 45 Gy in 25 fractions. In these patients,
neurological function scale (NFS) improved in 2 patients (8.3%), and
remained stable in 22 patients (91.6%). In forty-seven patients who
received radiotherapy, NFS was improved in 4 (8.5%), was stable
in 33 (82.5%) and worsened in 10 (21.3%) of patients. Among 16
patients who did not receive radiotherapy, NFS improved in 1 (6.3%),
remained stable in 7(43.8%) and worsened in 8 (50%) patients. There
was no correlation between the delivery of radiotherapy and change
in NFS (p=0.08).
Survival outcomes:
The median follow-up duration was 23 months (1-84 months).
The median PFS was 37 months (95% CI - 9.2-54.7 months) in those
patients treated with curative intent and 5 months (95% CI - 2.7-7.2
months) in those treated with palliative intent (p<0.0001) (Figure 1)
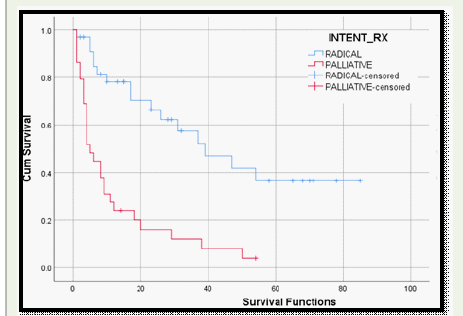
[Table 3]. The median OS was 39 months (95% CI - 18.3-59.6 months)
in those patients treated with curative intent (Figure 2) and 5 months
(95% CI - 2.7-7.2 months) in those treated with palliative intent
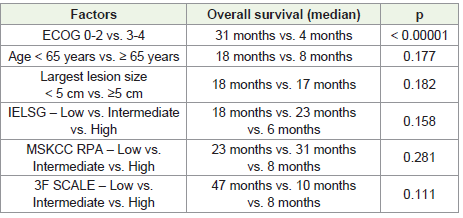
(p<0.0001). Univariate analysis revealed that a poor performance
status at diagnosis was a significant predictor of worse survival
(p<0.00001). Charlson comorbidity index, IELSG, MSKCC RPA
and 3F scores and classification did not significantly affect survival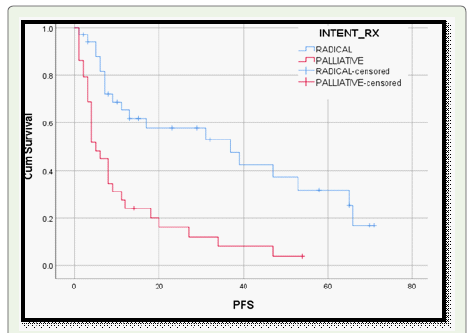
in this cohort in either univariate or multivariate analysis [Table 4,5]
Discussion
In this single institutional retrospective study of 63 patients with
PCNSL, 34 patients were treated with radical intent and 29 with
palliative intent. Median OS was 39 months in those treated with
curative intent and 5 months in those treated with palliative intent.
Poor performance status at baseline the significant factor affecting OS
in these patients.
PCNSL treatment has advanced significantly over the past
decade. Initially, WBRT was the mainstay of treatment, achieving
high response rates of up to 90%, but limited OS of 12-18 months
and substantial rates of intracranial recurrences [10-12]. The
addition of conventional chemotherapy regimens like CHOP and
R-CHOP did not improve survival due to inadequate intracranial
penetration of these drugs [13]. The addition of HD-MTX, marked
a major breakthrough, significantly improving median OS to 30-60
months [13,14]. Combination regimens with HD-MTX, cytarabine,
rituximab, and other agents like procarbazine and vincristine further
enhanced efficacy [15,16]. In the present study we could achieve a
median survival of 39 months as compared to 14 months in a previous

study from our institute, which is a remarkable achievement for these
patients 13. Intensified chemotherapy regimens such as MATRIX
have shown promising results, especially in younger, fit patients with
complete remission rates as high as 49% [17]. In our study complete
remission was observed in 41% patients.
Decisions regarding the intent of treatment in PCNSL are made
after a multidisciplinary discussion and considering factors such as
age, performance status, comorbidities, disease burden, neurological
function status and social support. Those patients who are unfit
for curative treatment are treated with palliative intent. Options
for palliation include best supportive care (BSC), WBRT alone and
single agent chemotherapy [18-20]. In the current study, 34 patients
were treated with curative intent and 29 patients were treated with
palliative intent. Among those patients treated with palliative intent
with WBRT, NFS improved in 2 (8.3%) of patients and remained
stable in 22 (91.6%) of patients.
In patients treated with curative intent, WBRT was delivered
up to a dose of 45 Gy. In 18 (28.5%) of patients this was achieved
in two phases,in the first phase 36 Gy was delivered to the whole
brain and a 9 Gy boost to the gross disease in patients where lesions
were well localised and could be delineated. Currently, patients who
receive radiotherapy alone and those with residual disease after
high-dose chemotherapy are treated with this dose fractionation. A
study by Thiel et al., have shown that patients treated with WBRT
had significantly better PFS compared to those who were kept on
observation after induction therapy[21].Off late, concerns regarding
neurocognitive decline have prompted the adoption of a risk stratified
approach for radiotherapy. Patients who achieve a complete remission
after chemotherapy are often given a reduced dose WBRT of 23.4-
30 Gy [16,17,22]. We treated 8(22%) patients with this schedule.
Alternative strategies being studied in this group to avoid WBRT
include consolidation with autologous stem cell transplantation or
cytosine arabinoside [23,24]. In the current study, those patients
who received HD-MTX-based chemotherapy, 7(11%) patients
received reduced dose WBRT after complete response and 17(26.5%)
received WBRT with definitive intent (36-45 Gy). Four (6%) patients
received consolidation therapy with cytosine arabinoside in addition
to WBRT.
The PRECIS study compared the neurocognitive outcomes
of patients who were randomised to receive consolidation with
either ASCT or WBRT with a dose of 40 Gy. The authors reported
that compared with the ASCT group, more patients in the WBRT
group had significant deteriorations in balance and neurocognition
during follow-up. However, all patients in the WBRT arm received
a dose of 40 Gy despite 46% of them achieving a complete response
after induction therapy [23]. A myriad of factors plays a role in
neurocognitive function in PCNSL. Apart from radiotherapy, the
intensity of chemotherapy, location, size and number of lesions may
also influence cognition [25]. In the current study, where radiotherapy
dose was adapted based on intent of treatment and response
to induction therapy, no correlation between radiotherapy and
worsening NFS was found. In 47 patients who received radiotherapy,
NFS improved in 4 (8.5%), remained stable in 33 (82.5%) and
worsened in 10 (21.3%) patients. Among sixteen patients who did not
receive radiotherapy, NFS improved in 1 (6.3%), remained stable in
7 (43.8%) and worsened in 8 (50%) of patients (p=0.08). However, it
should be noted that detailed MMSE and neurocognitive assessment
was not done in the present study.
According to the SEER database, OS significantly increased
from 12.5 months in the 1970s to 26 months in the 2010s [26]. In
the current study, median PFS was 37 months in those treated with
curative intent and 5 months in those treated with palliative intent
[Figure 1]. Median OS was 39 months in patients treated with curative
intent and 5 months in those treated with palliative intent [Figure 2].
Studies that incorporated high-dose chemotherapy along with WBRT
reported a median OS ranging from 30-60 months[13, 16, 27]which
is in line with the present study of 39 months. On univariate analysis,
a poor performance status at diagnosis was a significant predictor
of worse survival. Many studies have reported other factors which
adversely affect prognosis such as advanced age, poor performance
status, multifocal lesions, male gender, frontal lobe location and high
CSF protein concentrations [29-35].
Limitations of the study are single institutional, retrospective and lack of neurocognitive assessment of the patients.
Limitations of the study are single institutional, retrospective and lack of neurocognitive assessment of the patients.
Conclusion
In this single institution retrospective audit of patients with
PCNSL, median OS was 39 months in those treated with curative
intent and 5 months in those treated with palliative intent.
Radiotherapy dose was adapted based on intent of treatment and
response to induction therapy.There was no correlation between the
radiotherapy and worsening NFS. WBRT plays an important role in
the management of PCNSL in the era of high-dose chemotherapy.
References
Citation
Yadav BS, Gade VKV. Role of Whole Brain Radiotherapy in Patients of Primary Central Nervous Lymphoma in the Era of High Dose Methotrexate-Based Chemotherapy – A Single Institution Retrospective Audit. Indian J Neurol. 2025;6(1): 140.