Case Report
Progressive Multifocal Leukoencephalopathy in a Patient with Advanced HIV: A Case Report
Kunal Saini*, Akanksha Singh, Rohit Saini, Nargis Banoo
*Corresponding author: Kunal Saini, Department of Internal medicine, ABVIMS and DR RML Hospital, India, E-mail Id:virenderbawaniwal@gmail.com
Article Information:Submission: 23/12/2024; Accepted: 15/01/2025; Published: 18/01/2025
Copyright: © 2025 Saini K, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Abstract
Background: Progressive Multifocal Leukoencephalopathy (PML) is a demyelinating central nervous system disorder caused by JC virus reactivation in immunocompromised individuals, particularly those with advanced HIV. Although rare, its occurrence alongside pulmonary tuberculosis (TB) poses significant diagnostic and therapeutic challenges.
Case Presentation: We report the case of a 34-year-old male who presented with prolonged fever, Productive cough, significant weight loss, and progressive neurological decline. He was diagnosed with advanced HIV infection (CD4 count: 95 cells/μL) and pulmonary TB, confirmed by sputum CBNAAT. Neuroimaging revealed lesions suggestive of PML, later confirmed by cerebrospinal fluid analysis detecting JC virus DNA. The patient was initiated on antitubercular
therapy, followed by antiretroviral therapy after stabilization. Systemic improvements included increased appetite and weight gain of 8kg; however, neurological recovery remained limited.
Conclusion: This case underscores the complexity of managing advanced HIV with concurrent opportunistic infections like PML and TB. Early diagnosis using advanced imaging and molecular diagnostics, along with multidisciplinary management strategies, is critical for optimizing outcomes. However, neurological prognosis in PML remains poor, highlighting the need for innovative therapeutic approaches targeting JC virus and enhancing myelin repair.
On behalf of all authors, the corresponding author states that there is no conflict of interest.
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Keywords:Progressive Multifocal Leukoencephalopathy; JC virus; HIV/AIDS; Opportunistic infections; Antiretroviral therapy; Immune reconstitution
Introduction
Progressive Multifocal Leukoencephalopathy (PML) is a severe,
demyelinating disease of the central nervous system (CNS) caused by
the reactivation of the JC virus (JCV), a polyomavirus that resides
latently in the kidneys and lymphoid tissues of most individuals. In
most individuals, it remains a latent infection with a prevalence of
0.22 and incidence of 0.11 per 100,000 people.[1]
it is particularly virulent in patients with immunosuppressive
conditions such as AIDS, post solid organ and bone marrow
transplant recipients, malignancies, and chronic inflammatory
conditions.[2]JCV reactivates and causes progressive destruction
of oligodendrocytes, the myelin-producing cells in the brain. The
resulting demyelination manifests as subacute neurological deficits.
Its clinical presentation includes progressive focal neurological
dysfunction. Aphasia/dysarthria, monoparesis, hemiparesis, ataxia,
cortical blindness, and visual field defects are commonly reported.
Mental status changes such as confusion, dementia, and even coma
are seen [3].
PML is an opportunistic infection that occurs in approximately
3–5% of individuals with untreated HIV, especially those with a CD4
count below 200 cells/μL. Although antiretroviral therapy (ART) has
significantly reduced the incidence of PML, its presence remains an
ominous marker of advanced immunosuppression.[4]
This case report describes a 34-year-old male presenting with
advanced HIV infection, pulmonary tuberculosis (TB), and PML.
The interplay of multiple opportunistic infections and profound
immunosuppression complicated the diagnostic and therapeutic
approach. This case emphasizes the importance of a multidisciplinary
strategy in managing HIV patients with complex clinical presentations.
Case Presentation
A 34-year-old male labourer from Faridabad, Haryana, presented
to the emergency department with complaints of intermittent fever
and Productive cough in the last two months duration, accompanied
by progressive neurological decline over one month. The neurological
symptoms included reduced verbal output, and complete dependence
for ambulation. His wife provided the history, which was deemed
reliable.
The patient had a significant history of chronic smoking (smoking
index of 320) and daily alcohol consumption for over eight years. He
reported substantial weight loss, from 56 kg to 31 kg over the past
eight months, and decreased appetite. There was no prior history
of tuberculosis, diabetes mellitus, hypertension, or other chronic
illnesses.
On examination, the patient appeared cachexic with a BMI of 10.7
kg/m². He was conscious but disoriented to time, place, and person.
Neurological examination revealed gaze-evoked nystagmus and
reduced verbal response. Respiratory examination revealed normal
vescicular breath sounds but no other significant findings. Meningeal
signs were absent, and reflexes were intact.
Laboratory investigations revealed hemoglobin levels of 13.3 g/
dL, a total leukocyte count of 11,000/mm³ with a differential count
showing neutrophils at 88%, lymphocytes at 7%, monocytes at 4%, and
eosinophils at 1%. Platelet count was elevated at 4.6 lakhs/mm³, with
a MCV(mean corpuscular volume) of 84 fL and a HCT(Hematocrit)
of 42%. Liver function tests were within normal limits, with serum
bilirubin levels (total/direct) of 0.6/0.2 mg/dL and transaminases
(OT/PT) and ALP(Alkaline phosphatase) measured at 26/61 and
103 U/L, respectively. Serum electrolytes were stable with sodium
and respectively, potassium levels at 136 mEq/L and 3.47 mEq/L,
respectively. Calcium and phosphate levels were noted at 9.34 mg/dL
and 4.32 mg/dL, and total protein/albumin levels were 6.1/3.8 g/dL.
Inflammatory markers showed an ESR (Erythrocytic sedimentation
rate) of 40 mm/hour and CRP(C-Reactive Protein) of 87 mg/L.
Cardiac evaluation with electrocardiography (ECG) indicated
normal sinus rhythm, while chest X-ray (PA view) displayed
prominent bronchovascular markings with patchy opacities in the
right upper lung zone. Abdominal ultrasonography demonstrated
normal findings for the liver, portal vein, spleen, and bilateral kidneys
in terms of size, shape, and echotexture. A 2D echocardiogram
revealed no abnormalities.
Urine analysis showed 2 pus cells per high-power field, with
no proteinuria or hematuria, and cultures were sterile. Common
infectious diseases were ruled out, with negative results for Typhidot,
WIDAL, malaria card test, Rapid malarial antigen test(RMAT), and
peripheral smear for malaria. Blood cultures also yielded no growth.
Non-contrast CT (NCCT) of the head was normal, and cerebrospinal
fluid (CSF) analysis revealed 10 lymphocytic cells, glucose at 62 mg/
dL, protein at 97 mg/dL, and adenosine deaminase (ADA) levels of 6
U/L. Cryptococcal antigen, Gram stain, and bacterial/fungal cultures
were negative. Additionally, tests for EBV, CMV, and HSV were
negative.
Sputum CBNAAT confirmed the presence of Mycobacterium
tuberculosis. Fungal (KOH) and acid-fast bacillus (AFB) stains, along
with bacterial cultures, were negative. HIV-1 and 2 were reactive by
ELISA, with a CD4 count of 95 cells/μL. Serologies for HBsAg, anti-
HCV, VDRL, Brucella, and TORCH profile were negative. Thyroid
function tests were normal, as were serum ACE levels at 12 U/L and
ANA results.
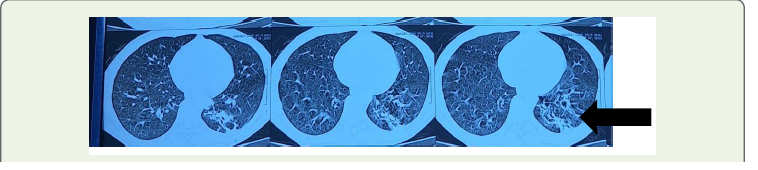
CECT chest showed findings suggestive of Multiple confluent
alveolar and branching tree in bud lesions involving apical and
anterior segment of right upper lobe,medial segment of right
middle,apical and posterior segment of bilateral lower lobe and
apical segment of left upper lobe likely Tubercular etiology
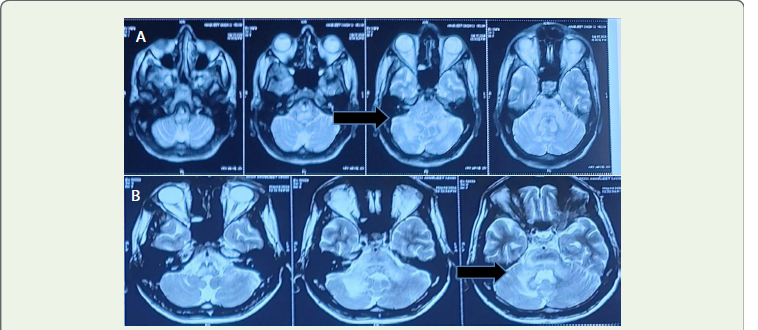
CEMRI BRAIN showed findings suggestive of non-enhancing
patchy and confluent assymetrical T1 Hypo and T2/Flair iso to
hyperintense altered signal intensity lesion involving the pons,
bilateral cerebellar peduncles and deep white matter of right
cerebellar parenchyma likely demyelination? Progressive multifocal
leucoencephalopathy?HIV Encephalopathy
CSF for JC VIRUS QUANTITATIVE - 20650 IU/ML
Sputum CBNAAT was positive for Mycobacterium tuberculosis,
confirming pulmonary TB.
Cerebrospinal fluid (CSF) analysis revealed lymphocytic
pleocytosis with elevated protein levels, and polymerase chain
reaction (PCR) detected JCV DNA, confirming the diagnosis of PML.
In this patient, anti-tubercular therapy (ATT) was initiated
for pulmonary TB, along with supportive care to address cachexia
and immune suppression. ART was introduced two weeks after
ATT commencement to reduce the risk of IRIS. Over five months,
the patient experienced systemic improvement, including an 8
kg weight gain and increased appetite. However, neurological
recovery was minimal, reflecting the generally poor prognosis
associated with PML.
Discussion
This case highlights the challenges of managing coexisting
opportunistic infections in patients with advanced HIV. Progressive
Multifocal Leukoencephalopathy (PML), resulting from JC virus
reactivation in the setting of profound immunosuppression, is a
severe condition associated with high mortality rates. Adaptive
immunity, particularly cellular responses, plays a crucial role in
controlling JC virus.[5]Any impairment, whether primary or
secondary, significantly increases the risk of viral reactivation. The use
of monoclonal antibodies for treating malignancies and autoimmune
conditions has contributed to a rise in secondary PML cases in recent
decades.[5]
The coexistence of PML and pulmonary tuberculosis (TB)
in this patient underscores the diagnostic difficulties faced
in immunocompromised individuals. Both conditions share
overlapping symptoms, such as fever, weight loss, and neurological
changes, making differentiation challenging. Neuroimaging and
advanced molecular techniques proved essential in distinguishing
PML from other CNS infections like tubercular meningitis or fungal
diseases. New-onset neurological symptoms in immunosuppressed
individuals should prompt consideration of PML as a possible
diagnosis.[6]Polymerase chain reaction (PCR)-based detection of JC
virus DNA in cerebrospinal fluid (CSF) is crucial for confirming the
diagnosis.[6]
The American Academy of Neurology (AAN) has established
diagnostic criteria for PML. In cases where histopathological analysis
is available, the presence of demyelination, bizarre astrocytes, and
enlarged oligodendroglial nuclei, along with positive JC virus PCR,
immunohistochemistry, or electron microscopy findings, confirms
the diagnosis. In the absence of histopathology, a combination of
clinical features, radiological findings, and positive CSF PCR for JC
virus is used.[6]
The primary management strategy for PML involves immune
restoration, as there are no targeted antiviral therapies for JC virus.
Antiretroviral therapy (ART) is pivotal in HIV-related PML, as it
enhances immune function by increasing CD4 counts and reducing
HIV replication. Beyond immune reconstitution, treatment options
remain limited. Withdrawal of immunosuppressive therapies, where
applicable, and initiation of ART in HIV-positive individuals offer
the most substantial survival benefit.[7]
However, in cases with concurrent TB, careful timing of ART
initiation is required to mitigate the risk of Immune Reconstitution
Inflammatory Syndrome (IRIS), which can exacerbate neurological
symptoms.
This case emphasizes the need for a multidisciplinary approach
involving infectious disease specialists, neurologists, radiologists,
and critical care teams to address the complexities of managing HIV
patients with overlapping opportunistic infections. Despite immune
restoration through ART, the prognosis for PML remains poor,
with survivors often facing significant neurological impairment.
Studies have investigated the effectiveness of 5-hydroxytryptamine
antagonists such as mirtazapine and risperidone, nucleoside
analogs like cidofovir and cytosine arabinoside, as well as biological
treatments including interferon alpha. However, these approaches
have not demonstrated conclusive efficacy[8-11]. In recent times,
positive results have been observed in patients undergoing treatment
with immune checkpoint inhibitors.[12-14]and infusion of virusspecific
T cells.[15]
Research efforts are needed to develop novel therapies targeting
JC virus and promoting myelin repair.
Conclusion
This case highlights the intricate interplay between advanced
HIV, pulmonary TB, and PML in a profoundly immunosuppressed
individual. The early recognition of opportunistic infections, timely
initiation of ATT and ART, and careful management of IRIS were
pivotal in improving the patient’s systemic condition with significant
improvement in weight gain of 9kg and of increased appetite
While the neurological recovery in this patient was limited,
the case underscores the importance of a comprehensive approach
to diagnosing and managing complex HIV-associated illnesses.
The findings emphasize the role of advanced diagnostics, such as
neuroimaging and molecular PCR, in identifying PML and guiding
treatment decisions.
This report adds to the growing body of literature on HIVassociated
PML and calls for increased awareness, early detection,
and resource allocation for managing these challenging cases. Future
research into targeted antiviral therapies and adjunctive treatments
for PML is essential to improve survival and quality of life for affected
patients.
References
Citation
Saini K, Singh A, Saini R, Banoo N. Progressive Multifocal Leukoencephalopathy in a Patient with Advanced HIV: A Case Report. Indian J Neurol. 2025;6(1): 139.