Case Report
Coexistence of Neuromyelitis Optica Spectrum Disorder, Sjogren’s Syndrome And Tuberculosis In A Postpartum Female-A Case Report
Priyanka P1*, Shobana N2, Sacratis M3, Selvakumar CJ4 and Kumar VS5
Department of Neurology, Coimbatore Medical College and Hospital Coimbatore, Tamil Nadu, India
*Corresponding author:Pasala Priyanka, Department of Neurology, Coimbatore Medical College And Hospital Coimbatore, Tamil Nadu, India E-mail Id: indupriya.pasala@gmail.com
Article Information:Submission: 15/10/2024; Accepted: 31/10/2024; Published: 05/11/2024
Copyright: ©2024 Priyanka P, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Patients with NMOSD coexisting with both sjogren’s syndrome and tuberculosis are very rare. There are no specific guidelines for the treatment of these patients especially during pregnancy. We report a case of AQP4 seropositive Nmosd associated with Sjogren syndrome and tuberculosis in a postpartum female and is treated with rituximab. In 2017 a 25 year female presented with quadriparesis and is diagnosed as AQP4 positive NMOSD. She is treated with
I.V.methyl prednisolone. 1 year later she became pregnant and is asymptomatic during pregnancy and at 2 months postpartum she developed paraparesis. She is treated with i.v.methyl prednisolone and plasmapheresis and started on Azathioprine. At the same time she is diagnosed with Sjogren’s syndrome. In 2021 Azathioprine is changed to MMF in view of pancytopenia. In 2022 she developed pulmonary TB and used ATT for 6 months. She discontinued MMF
at that time. After completing ATT she conceived for the second time, remained asymptomatic throughout pregnancy and at 3 months postpartum she again developed quadriparesis. She is treated with rituximab with significant improvement of symptoms. For treating relapsing NMOSD coexistent with Sjogren syndrome and tuberculosis in the postpartum period, rituximab may be a good choice.
Keywords:Neuromyelitis Optica Spectrum Disorder; Sjogren Syndrome; Tuberculosis; Rituximab
Abbreviations
AQP4-Aquaporin 4; ATT-Anti TB treatment; MMFMycophenolate Mofetil; NMOSD-Neuromyelitis Optica spectrum
disorder; TB-Tuberculosis.
Introduction
Neuromyelitis optica (NMO) also known as Devic syndrome
is a rare relapsing auto-immune disease of the central nervous
system (CNS) which is sometimes found in association with other
autoimmune disorders, including SS. Based on the revised criteria by
Wingerchuck et al, a diagnosis of NMO can be made in the presence
of both absolute and two of three supportive criteria [1]. The absolute
criteria include optic neuritis and myelitis; while the supportive
criteria are magnetic resonance imaging (MRI) evidence of a
contiguous spinal cord lesion (3 or more segments in length), MRI
brain non-diagnostic for multiple sclerosis and serological evidence
of NMO-IgG or aquaporin 4 (AQP4) antibodies. NMO spectrum
disorders (NMOSD) includes a wide range of neurologic conditions
that express NMO antibody and share features with NMO but do not
meet the strict diagnostic criteria specified previously [2].
Case Presentation
A 27-year-old female presented with recurrent neurological
deficits i.e.1ST EPISODE IN 2017 – weakness of all four limbs with bladder
symptoms and sensory loss below neck. MRI showed long segment
myelitis in cervical region. Serum aquaporin 4 antibody is positive.
patient is treated with I.V methylprednisolone pulse therapy for 3
days. patient had complete improvement in 2 months. patient was on
oral steroids for 1 year and stopped once she became pregnant.
2ND EPISODE IN OCTOBER 2019 – paraparesis, reduced
sensation below thorax and urge incontinence. The patient was 2
months postpartum during the onset of symptoms. MRI showed
T2 hyperintense lesions in dorsal spinal cord. She received I.V
methylprednisolone for 3 days and large volume plasmapheresis
-5 sessions and then started on oral azathioprine. At the same time
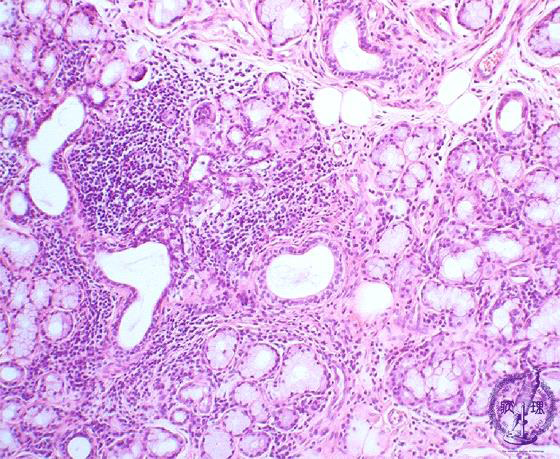
patient is diagnosed with Sjogren’s syndrome – lip biopsy proven.
Concluded as NMO-Sjogren Overlap.
3rd EPISODE IN APRIL 2020 - 1month history of bilateral painful
nonprogressive blurring of vision. VEP showed P100 prolongation
in both eyes. She is treated with i.v.methyl prednisolone and large
volume plasmapheresis and continued on azathioprine.
IN 2021 –Routine investigations revealed pancytopenia.
Azathioprine was stopped in view of pancytopenia. Planned for
serum TPMT testing and to start azathioprine in low dose but patient
refused for the test. Mycophenolate mofetil is started for long term
immunomodulation.
IN JANUARY 2022 – Patient developed pulmonary tuberculosis
and used ATT for 6 months. She has no contact history of tuberculosis.
She didn’t take MMF at this time. 1 month after completing ATT she
conceived for the 2nd time.
4TH EPISODE IN 2023 – stiffness of all 4 limbs with no weakness
or sensory involvement or bladder involvement. She is 2 months
postpartum during this time.
On Examination patient is conscious and oriented and vitals are
stable. HMF normal. Visual acuity 6/18 with fundus pale disc. Other
cranial nerves are intact. Motor system increased tone in all limbs


with power 5/5. DTR 2+. Sensory system-touch pain and temperature
-intact in all dermatomes. Vibration and proprioception intact
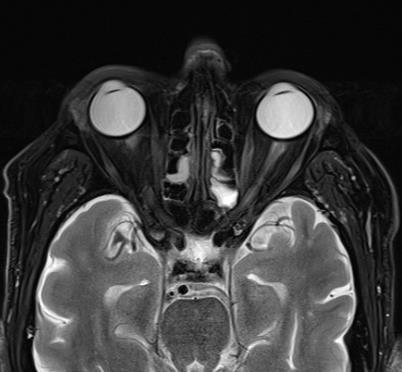
bilaterally. MRI showed altered signal intensity with thickening of
both optic nerves and altered signal intensity in the cord extending
from cervico-medullary junction to C7. Patient is treated with I.V
methylprednisolone for 5days and given 1gm of rituximab. Patient
improved after rituximab injection and is relapse free till now.

Discussion
NMOSD is a relapsing neurological illness that has been
sometimes reported in association with primary SS and SLE. NMO
is characterized by recurrent episodes of myelitis and optic neuritis
and most patients have a unique antibody against NMO IgG/ AQP4.
Patients who have NMO IgG/AQP4 antibodies have frequent relapses
compared to those who do not have the antibodies [3].
Relapsing NMO carries a poor prognosis, thereby validating the
need for early testing and treatment. It has been reported to have
a 5 year survival rate of approximately 80% [4]. The cumulative
effect of recurrent attacks renders a debilitating outcome, including
permanent disabilities requiring assistive devices for ambulation and
monocular blindness [4]
NMO and NMOSD are rare diseases with no consensus on
treatment guidelines. The treatment options are empiric and based
on disease severity ranging from plasmapheresis, corticosteroids, and
rituximab to oral agents such as azathioprine, MMF and methotrexate.
Early initiation of systemic steroids alone or in combination with
other immunosuppressive therapies is most often used. In our
patient with relapsing disease course, combination of steroids and
azathioprine/MMF is used.
One established treatment of acute NMOSD relapses during
pregnancy is intravenous administration of 1 g methylprednisolone/
day over five consecutive days. For non-pregnant NMOSD patients,
currently favoured long-term treatment includes azathioprine (AZA)
and rituximab (RTX). Case reports describe bone marrow suppression
with anaemia and severe lympho- and pancytopenia in infants after
maternal AZA exposure. Evidence suggests that RTX treatment
carries a higher risk of premature births. As RTX treatment during
pregnancy also transiently depletes B cells in newborns measuring B
lymphocyte levels of fetuses is advised if exposed to RTX after the
first 20 weeks of pregnancy. Overall, careful risk-benefit analysis of
stopping or continuing immunosuppressive treatment is necessary
in patients planning families. Treatment with mycophenolate mofetil
should stop 6 weeks; methotrexate, 12 weeks; and mitoxantrone, 6
months before attempting to conceive [5].
Conclusion
we report this case due to its rarity of occurrence. There are no
specific guidelines for the treatment of NMOSD coexistent with
Sjogren syndrome and tuberculosis especially during pregnancy or
post-partum period. Rituximab might be used in such patients with
less side effects during pregnancy or lactation not only to improve
the disease symptoms but also to reduce the risk of relapses. Further
studies are needed to establish guidelines for new treatment options.
References
Citation
Priyanka P, Shobana N, Sacratis M, Selvakumar CJ, Kumar VS. Coexistence of Neuromyelitis Optica Spectrum Disorder, Sjogren’s Syndrome And Tuberculosis In A Postpartum Female-A Case Report. Indian J Neurol. 2024;5(1): 137.