Case Report
GABA B Receptor Autoimmune Encephalitis –A Case Report
Gupta A*, Bhardwaj S, Munjal J, K Lal S, Nakra R and Lal V
Department of Hematology and Immunopathology, National Reference Lab, Dr Lal Path labs, Rohini , New Delhi, India
*Corresponding author:Ajay Gupta, Department of Hematology and Immunopathology, National Reference Lab, Dr Lal Path labs, Rohini, New Delhi, India, Email:drajaygupta76@gmail.com
Article Information:Submission: 14/10/2024; Accepted: 30/10/2024; Published: 07/11/2024
Copyright: © 2024 Gupta A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: Although autoimmune encephalitis is a rare disease with an incidence of 0.8/ 100,000, it is associated with cognitive decline, epilepsy, behavioural disturbances, and impairment in the level of consciousness. Therefore, prompt diagnosis and treatment lead to improvement or full recovery in most cases [6]. Encephalitic syndromes are a common medical emergency. The importance of early diagnosis and appropriate treatment is paramount. If initial investigations for various conditions including infectious agents prove negative, other diagnoses must be considered promptly. Autoimmune encephalitis are being increasingly recognized as important (and potentially reversible) non-infectious causes of an encephalitic syndrome [1]. Some encephalitis or seizure disorders once thought idiopathic now seem to be immune mediated [3]. In 2010 the spectrum of known antigens in autoimmune encephalitis has been expanded by GABAB receptors. Until now over 80 patients with GABAB receptor encephalitis have been described [2].
Introduction
Anti-gamma-aminobutyric-acid B receptor (anti-GABABR)
encephalitis, which was first described by Lancaster et al., is clinically
characterized by limbic encephalitis (including seizures, cognitive
disorders, behavioural changes) and other uncommon clinical
syndromes (such as cerebellar ataxia and opsoclonus-myoclonus
syndrome) [4]. Approximately 50% of patients are diagnosed
with small cell lung cancer (SCLC), and in rare cases, thymoma,
malignant melanoma, breast carcinoma, rectal carcinoma, multiple
myeloma, esophageal carcinoma, sarcomatoid carcinoma (SC), and
gastric adenocarcinoma have also been found [6]. Antibodies against
GABAB receptor are found in serum or CSF [5]. In the majority of
patients oligoclonal bands are found in the CSF and 24 hr IgG levels
are increased in 92% of patients [7]. Antibody-mediated encephalitis
constitutes a group of inflammatory central nervous system disorders
that are associated with antibodies against neuronal cell-surfaces
proteins, ion channels, or receptors. The most common type of
autoimmune encephalitis is autoantibodies against the N-methyld-
aspartate (NMDA) receptor. Other autoantibodies include those
directed against the voltage-gated potassium channel complex
(VGKC), the α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic
acid (AMPA) receptor, the γ-aminobutyric acid (GABA) receptor,
anti-dipeptidyl-peptidase-like protein-6 (DPPX, viz. DPP6), and the
glycine receptor [6].
We report a case of a patient who was diagnosed with autoimmune
encephalitis due to GABAB receptor autoantibodies who had long
history of unexplained fever, diabetes, severe hypertension having
normal routine lab and radiological investigations initially and
gradually progressing onto having seizures and neurological deficits
with deteriorating life threatening health condition.
Case Presentation
A 56 yr old male pt admitted with history of 10 days fever being
investigated upon, all routine lab investigations CBC, LFT, KFT ESR,
CRP, Urine R/M, fever profile including MP, Blood C/s, Dengue and
X-ray Chest, USG whole abdomen were normal. pt was diabetic,
hypertensive with Hba1c 7.0 and BP 142 / 90 mmHg respectively and
was on medication for both conditions, pt was put on IV antibiotics
for 2 days, fever subsided on 3rd day of admission and discharged on
4th day. After 2 days pt has one episode of seizure, BP 200 / 120 mmHg,
MRI brain was normal was put on antihypertensive medication and
BP was 140/90 mmHg in 2 days . After couple of days pt had repeat
episode of seizure , again 2nd MRI was done which was normal.pt
also had little delirium. Subsequently he had repeated episodes of
seizures with twitching of left side of face and frothing, pt BP was
fluctuating and was put on anti-epileptic drugs. looking at the sign /
symptoms a provisional diagnosis of Hypertensive encephalopathy
was made. After 10 days of being afebrile, pt again had fever and was
quite unstable as he was irritable, in continuous delirium, amnesia,
even pulling off infusion line. Pt was on antibiotics, anti diabetics,
antihypertensives, anti epileptics drugs with BP in normal range.
As blood counts were normal, CSF tap revealed TLC 25 cells/
cumm, raised protein, low sugar, CSF c/s was normal and bacterial
meningitis was ruled out .pt was put on acyclovir with Anti tubercular
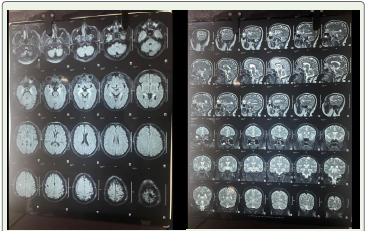
therapy and higher antibiotics but didn’t respond and a repeat MRI
was done after 20 days of 2nd MRI showed T1 hypointense / T2
hyperintense, punctate T2 /FLAIR hyperintensities seen involving
the bilateral mesial temporal lobes including amygdala , hippocampi,
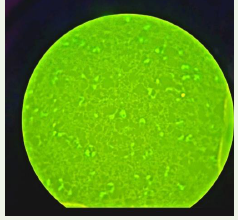
parahippocampal gyri. Based on the finding of MRI – test for
autoantibodies to diagnose Autoimmune encephalitis and test for
oligoclonal bands, test for paraneoplastic syndrome antibodies was
done. GABA B receptor autoantibodies were positive and oligoclonal
bands were positive. Autoantibodies against paraneoplastic syndrome
were negative. EEG was done which showed generalized beta activity.
PET –CT was negative for any lymph nodal or any distant metastasis,
presence of diffuse mild increased FDG uptake also noted in bilateral
mesial temporal lobe, bilateral basal ganglia which is suggestive of
Autoimmune encephalitis. Finally a Diagnosis of GABA B receptor
Autoimmune encephalitis was made after more than one month of
onset of 1st seizure. Pt was put on IV immunoglobulins for 5 days,
his condition improved. Further pt was advised with follow up and
treatment with rituximab [Figure 1,2].
Discussion
GABA B receptor autoimmune encephalitis , the diagnosis can
be delayed which may be due to the variable presentation of the
disease as was seen in this case , the diagnosis was made 1.5 month
after initial sign / symptom. This type of encephalitis is often seen in
middle aged and older men as was seen in this particular case. Tumour
are associated in 50% of cases with more commonly Small cell lung
carcinoma however no malignancy was seen in our case. It usually
presents with seizures or status epilepticus, ataxia, memory loss as
was seen in this case . Some pt might experience fever after which
epilepsy, cognitive dysfunction, behaviour abnormalities may be seen
and fever may be the first symptom as was seen in this case. MRI is
performed early upon pt presentation , however can be negative in
large no. of cases [8] as was seen in this case where first 2 MRI were
negative. Role of autoantibodies testing in Serum / CSF via cell based
assay using IFA technique is of major importance as they tend to be
present in early onset when MRI is often negative.
Conclusion
Anti GABA B receptor encephalitis mainly occurs in middle
aged men. The onset can be with fever and frequent epileptic
seizures, cognitive dysfunctions and abnormal mental behaviour. 50
% cases may be associated with tumour more like lung carcinoma.
Comprehensive early testing of Autoantibodies in serum / CSF helps
in early diagnosis as MRI may be negative in early stages. A need for
early diagnosis and understanding of disease is a good way to prevent
misdiagnosis and delayed treatment.
References
Citation
Gupta A, Bhardwaj S, Munjal J, Lal KS, Nakra R, et al. GABA B Receptor Autoimmune Encephalitis – A Case Report. Indian J Neurol. 2024;5(1): 136.