Case Report
Wallerian Degeneration of the Bilateral Middle Cerebellar Peduncles Secondary to Pontine Infarct
Anusha I1*, Shobana N2, Sacratis M3, Selvakumar CJ4 and Sadeeshkumar V4
1Resident, Department of Neurology, Coimbatore Medical College, Tamilnadu, India
2Professor and HOD, Department of Neurology, Coimbatore Medical College, Tamilnadu, India
3Professor, Department of Neurology, Coimbatore Medical College, Tamilnadu, India
4Assistant Professor, Department of Neurology, Coimbatore Medical College, Tamilnadu, India
2Professor and HOD, Department of Neurology, Coimbatore Medical College, Tamilnadu, India
3Professor, Department of Neurology, Coimbatore Medical College, Tamilnadu, India
4Assistant Professor, Department of Neurology, Coimbatore Medical College, Tamilnadu, India
*Corresponding author:Anusha I, Resident, Department of Neurology, Coimbatore Medical College, Tamilnadu, India. E-mail Id: anushainduri38@gmail.com
Article Information:Submission: 30/09/2024; Accepted: 21/10/2024; Published: 25/10/2024
Copyright: © 2024 Anusha I, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Bilateral middle cerebellar peduncle hyperintensities in MRI can be described in several diseases. Previous studies have indicated that neurodegenerative diseases like OPCA, SDS are most likely to affect bilateral MCP. Recent studies have proven that there are many causes of bilateral MCP involvement of which most common being ACI with arterial occlusion. WD, MSA, NMO, heroin-induced leukoencephalopathy, and PCNSL are other causes. Specific
neuroimaging findings& clinical features help in differentiating such lesions. We present a case of 40year old male presented with recurrent pontine stroke having bilateral middle cerebellar peduncle T2 and FLAIR hyperintensities
in repeat MRI due to Wallerian degeneration secondary to pontine infarction. It is important to know how to differentiate WD from Acute stroke which is highlighted in this study.
Keywords:OPCA: olivopontocerebellar atrophy; SDS: schwamon diamond syndrome; WD: Wallerian degeneration; MCP: middle cerebellar peduncle; ACI: acute cerebral infarction; MSA: multisystem atrophy; NMO: neuromyelitis optica
Introduction
Wallerian degeneration is the process of demyelination and
disintegration of distal axonal segment following the interpretation
of axonal integrity or damage to the proximal neuron. Wallerian
degeneration of bilateral MCP’s can be seen after a pontine stroke.
This can be seen as T2,FLAIR hyperintensities in MRI. Although it
looks similar to an infarct in MRI, stroke causing bilateral symmetrical
lesions in MCP’s is very rare. However, it is important to differentiate
it from other causes of bilateral MCP’s hyperintensities in MRI.
We report a case presented with recurrent CVA pontine infarct
showing Bilateral symmetrical T2 flair hyperintensities in middle
cerebellar peduncle 2months after the onset of symptoms.
Case Discussion
A 49-year-old male hypertensive and diabetic presented with chief
complaints of acute onset weakness of left upper limb and lower limb
for 1 week with complaints of swaying to left while walking. History
of similar complaints 3 months back from which he was partially
recovered with MRS 2/6.On examination: patient was awake, alert,
oriented to time, place and person with normal vitals. Higher mental
function and Cranial nerves were normal. Motor examination – bulk
& tone of all 4limbs– normal, Power – left upper limb and lower limb
-4/5, right side 5/5.DTR 2+ bilateral, plantar extensor on left side with
normal sensory examination. FNT, FFNT normal bilateral. No
dysdiadochokinesia, broad-based gait and impaired tandem walking
present.
Routine investigations like complete blood picture, renal and liver
functions tests, lipid profile were normal, with normal ECG,ECHO
and bilateral CV doppler. Serum copper, serum calcium, fund us were
normal.
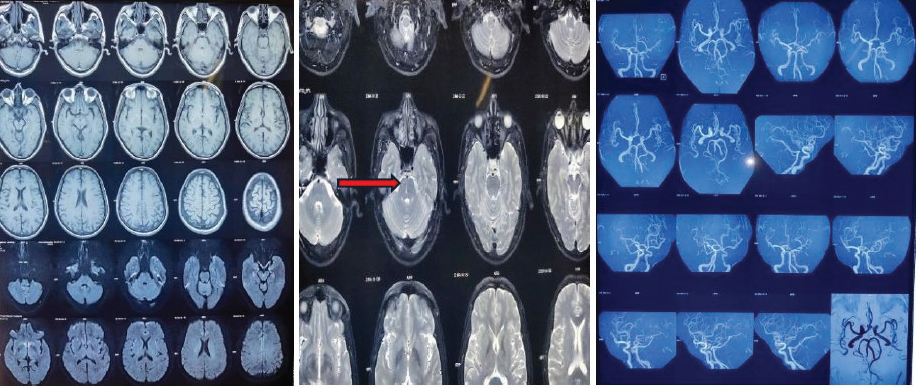
Due to financial issues MRI brain was done 20 days after the
first stroke which was showing Gliotic foci in central mid-pons in
T2W[Figure 1B], MRA normal [Figure 1C].
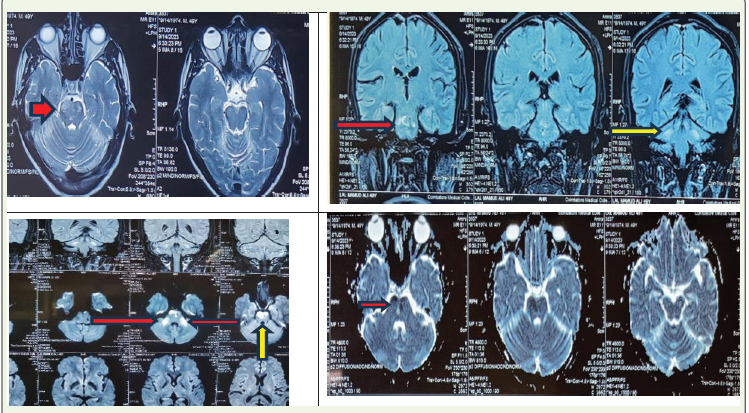
MRI brain which was repeated after the onset of symptoms
second time showing T2 [Figure 2A]/flair [Figure 2B] hyperintensity
noted in anterior aspect of bilateral pons with diffusion restriction
[Figure 2C], with hypodensity in ADC [Figure 2D]T2 [Figure 2A]) / FLAIR[Figure 2B] hyperintensityis noted in Bilateral middle
cerebellar peduncle with subtle diffusion restriction [Figure 2C], with
no ADC changes[Figure 2D] likely to be acute infarct in pons with
Wallerian degeneration in Bilateral middle cerebellar peduncle.
Discussion
Wallerian degeneration refers to progressive anterograde
disintegration with demyelination of the distal axons following injury
to the proximal axon or soma [1]. The histologic and metabolic
characteristics of the different stages of WD are correlated with
specific findings on conventional MRI [2]. The first stage (within
20 days after injury) is characterized by disintegration of the axons
and myelin sheaths without abnormal signals on conventional MRI.
However, several studies have revealed that DWI can depict transient
signal abnormalities at this stage, especially within the first 14 days of
the stroke (pre‐WD) [3,4]. The second stage (from 20 days to 60-120
days after injury) is characterized by rapid myelin protein breakdown,
during which the tissue becomes more hydrophobic, resulting in
hypointensities on proton‐density and T2‐weighted imaging. Myelin
and lipid breakdown, gliosis, and increase in hydrophilic tissue
during the third stage (98 days after injury) result in the appearance
of hyperintensities on T2‐weighted and FLAIR imaging and
hypointensities on T1‐weighted imaging. The last stage (after several
years) is characterized by volume loss due to atrophy. Therefore, WD
entails the degeneration of axonal structures and demyelination, and
finally fibrosis and atrophy of the affected fibertracts [2].
Diffusion abnormalities may occur in degenerating fibers and are
time‐related, irrespective of the ADC sequence, especially during the
first and third stages. This occurrence might be related to cell swelling,
demyelination with axonal degeneration, phagocytotic activity, and
water uptake and indicate that diffusion abnormalities in degenerating
fibers are not specific and may provide evidence to differentiate WD
from ACI[2].
Wallerian degeneration is observed most frequently in the
corticospinal tract following injury to the motor cortex or internal
capsule and presents as ipsilateral T2 hyperintensity or atrophy of the
cerebral peduncle[5].
The middle cerebellar peduncle (MCP) consists of the transversely
coursing pontocerebellar fibers that arch across the midline and gather
on each side [6]. The pontine nuclei are intermediary gray matter
scattered in the basis pons and part of the cortico-ponto-cerebellar
pathway (closed loop communication between the cerebellum and
pre-central /prefrontal cortex that control not only the action of
motor tasks but also planning and initiation of movements)[7].
Bilateral MCP lesions were found in many diseases.
ACI (acute cerebral infarction), WD,MSA(multiple system
atrophy),NMO(neuromyelitis optica), heroin induced leukoencephalopathy
and PCNSL(primary central nervous system lymphoma).
Most of these are associated with other cerebral lesions[2].
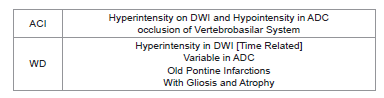
Patients with ACI exhibited bilateral MCP‐restricted diffusion
hyperintensities on diffusion‐weighted imaging, hypointensity on
ADC and corresponding stenosis or occlusion of the vertebrobasilar
system. However bilateral MCP infarctions are rare.In initial MRI of
patients with WD depicted pontine infarctions, while symmetrical
MCP lesions as above mentioned, with chronic pontine lesions and
gliosis were observed on follow‐up MRI. Symmetrical MCP lesions,
cruciform hyperintensity, and marked atrophy in the posterior fossa
were characteristic manifestations of MSA-C[8,9]. Longitudinally
extensive myelitis affecting more than three vertebral segments on
cervical MRI and positive serum AQP4‐IgG may be indicative of
NMOSD[10]. Heroin‐induced leukoencephalopathy often results in
extensive, symmetrical lesions of the cerebral and cerebellar white
matter, posterior limb of internal capsule & splenium of corpus
callosum[11]. PCNSL was indicated by a significant and characteristic
“fist” sign on contrast enhanced MRI[12].
Conclusion
In bilateral symmetrical MCP hyperintensities in MRI following
pontine infarction Wallerian degeneration should also be considered
before labelling it as a new infarction and subsequent changes should
be identified. Neurologists should be familiar with WD of the bilateral
MCPs to avoid misdiagnosis as an additional infarction.
References
Citation
Anusha I, Shobana N, Sacratis M, Selvakumar CJ, Sadeeshkumar V. Wallerian Degeneration of the Bilateral Middle Cerebellar Peduncles Secondary to Pontine Infarct. Indian J Neurol. 2024;5(1): 135