Case Report
Bickerstaff Brainstem Encephalitis Masquerading As Snake Bite: A Case Report
Meghana BL1, Jain MK1*, Patnaik S1, Sahoo B1, Behera MR1, Mishra R1 and Panda S2
1Department of Pediatrics, Kalinga Institute of Medical Sciences, KIIT University, Bhubaneswar, Odisha, India
2Department of radio diagnosis, Kalinga institute of medical sciences, Bhubaneswar, Odisha, India
2Department of radio diagnosis, Kalinga institute of medical sciences, Bhubaneswar, Odisha, India
*Corresponding author:Mukesh Kumar Jain, Department of Pediatrics, Kalinga Institute of Medical Sciences, KIIT University, Bhubaneswar, Odisha, India. E-mail Id: Mukesh26.jain@gmail.com
Article Information:Submission: 06/04/2024; Accepted: 25/04/2024; Published: 30/04/2024
Copyright:© 2024 Meghana BL, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction:Bickerstaff brainstem encephalitis (BBE) is a rare immune mediated disease that has good prognosis. It presents with several clinical and immunological similarities with Guillain Barre syndrome and miller fisher syndrome.
Aim:To sensitize the pediatrician to revise the diagnosis of snake bite in absence of improvement with antisnake venom.
Case: We report a case of 5-year-old male child presented with drooping of eyelids followed by difficulty breathing and altered sensorium, provisionally diagnosed and treated as a case of snake bite later diagnosed as Bickerstaff encephalitis clinically and supported by laboratory and radiological investigations.
Results:The child had fully recovered with supportive care and IVIG.
Conclusion:The interest in this observation lies in its rarity, presenting symptoms and drastic clinical improvement with immunotherapy. Any case of neurogenic snake bite which did not respond to conventional treatment, we should look for alternative diagnosis.
Aim:To sensitize the pediatrician to revise the diagnosis of snake bite in absence of improvement with antisnake venom.
Case: We report a case of 5-year-old male child presented with drooping of eyelids followed by difficulty breathing and altered sensorium, provisionally diagnosed and treated as a case of snake bite later diagnosed as Bickerstaff encephalitis clinically and supported by laboratory and radiological investigations.
Results:The child had fully recovered with supportive care and IVIG.
Conclusion:The interest in this observation lies in its rarity, presenting symptoms and drastic clinical improvement with immunotherapy. Any case of neurogenic snake bite which did not respond to conventional treatment, we should look for alternative diagnosis.
Keywords:Bickerstaff Brainstem Encephalitis; Snake Bite; GuillianBarre Syndrome Variant
Introduction
Bickerstaff Brainstem Encephalitis first described in 1957 by
Bickerstaff et al., is a rare autoimmune encephalitis characterized by
an acute brainstem dysfunction occurring few days after an infection
or vaccination, characterized by ophthalmoplegia, ataxia and altered
sensorium.[1] It presents with several clinical and immunological
similarities with Guillain Barre syndrome and miller fisher syndrome.
[2] The aim of this work is to acknowledge atypical presentation of
GBS and consider BBE as differential diagnosis in case of suspected
neurotoxic snake bite with no improvement following ASV.
Case Report
We report the case of 5-year-old male child presented with
complaints of drooping of eye lid followed by unable to stand and
slurring of speech since last 2 days.There was no history of recent
travelling, exposure to toxic materials, or head injury. He was fully
vaccinated, and had previously been a healthy child. At local hospital,
child received total of 20 vials of antisnake venom (ASV) in 2 divided
doses, Atropine, Neostigmine suspecting as a case of neurogenic
snake bite, also symptomatic treatment done with Mannitol for
features of raised ICP. There in view of low GCS and difficulty
breathing child was intubated and referred to our hospital on day 2
of illness. We received child in emergency room with bag and tube
ventilation, child was afebrile with bradycardia,hypertension and
abnormal breathing pattern. Child was immediately shifted to PICU
and stabilized. There is history of flu like illness 15 days before onset
of symptoms. Neurological examination showed ophthalmoplegia,
brisk deep tendon reflexes with bilateral plantar extensor, rest clinical
examination was insignificant. Routine blood investigation revealed
hemoglobin of 11.7g/dl, total leukocyte counts 8150/ microliter (60%
neutrophil)with negative sepsis screen. Liver function test, renal
function test and coagulation parameter are within normal limits.CSF
examination showed total 2 cells, glucose 88mg/dl, protein 76.5mg/dl
(albumin-cytological dissociation). Presence of albumin cytological
dissociation along with ophthalmoplegia, hyperreflexia and altered
sensorium compel us to think of BBE. Serum Anti Gq1b antibody
was sent and came out to be positive. Nerve conduction study showed
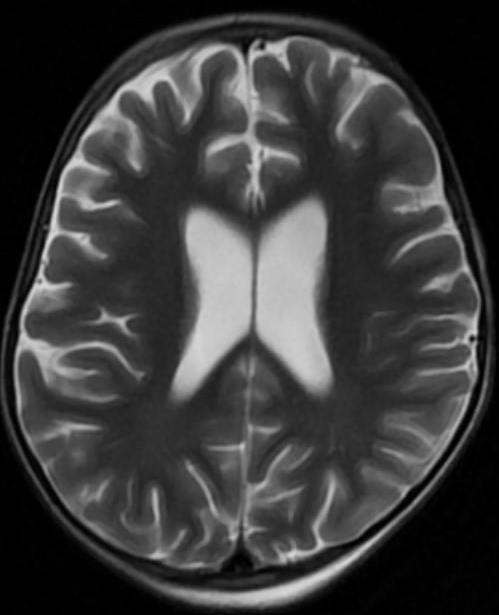
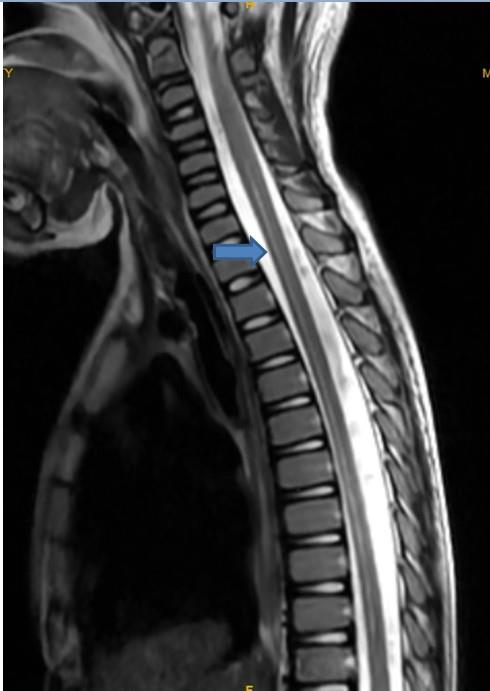
axonal type of motor sensory neuropathy.MRI brain and spine showed
diffuse cerebral atrophy with minimal syrinx with T2 hyper intensity
in a long segment of cervico-dorsal cord.Electroencephalography
(EEG) showed high amplitude slow wave activities without
epileptiform discharges, suggesting encephalopathy. Child received
IvIg on day 4 of illness at 2gm/kg over 5 days. Intubated for 13 days
following which tracheostomy was done and on ventilator support
for total of 20 days. Gradually regained power in bilateral upper and
lower limbs by day 30 of hospitalization and was being discharged.
On follow up child is healthy and completely recovered.
Discussion
brainstem encephalitis is an autoimmune disorder that
falls under same spectrum as Miller Fisher syndrome and Guillian Barre
syndrome. This is classified as a central nervous system (CNS) disease;
whereas, Guillain–Barre syndrome and Miller Fisher syndrome are
peripheral nervous system (PNS) disorders [3]. It is similar to Miller
Fisher syndrome, a variant of Guillain-Barre syndrome, in that they
share features such as ophthalmoplegia and ataxia. The difference is
that patients with Bickerstaff’s brainstem encephalitis have impaired
consciousness & hyperreflexia, whereas patients with Miller Fisher
syndrome have alert consciousness and areflexia. Progressive,
relatively symmetric external ophthalmoplegia and ataxia by 4 weeks’
and ‘disturbance of consciousness or hyperreflexia’ are required as
clinical features for the diagnosis of BBE [4]. The Etiopathogenesis of
the disease is still unclear. Infectious etiology could be considered as
an antecedent history of upper respiratory tract infection is usually
present before the development of the neurological symptoms. [5]
Production of gangliosides from some bacteria, similar to those of
myelin constituent, may induce a molecular mimicry phenomenon in
which the production of specific antibodies (anti-GQ1b). Infectioninduced
immunological mechanisms may play a pathogenic role
in BBE as anti-G1Qb IgG antibody is positive in more than 60%
of patients (3), which is positive in our case.Anti-GQ1b antibodies
are commonly found in both, but more frequently in Miller Fisher
syndrome.[6] Typical MRI finding (hyper intensity on T2-weighted
images of the pons, medulla, thalamus, or cerebellum) [6]are absent
butpresence of minimal syrinx with T2 hyper intensity in a long
segment of cervico-dorsal cord supports ourdiagnosis.According to
a previous report, 11% of 47 patients with Bickerstaff’s brainstem
encephalitis had abnormalities on brain MRI, whereas 57% of 30
patients with Bickerstaff’s brainstem encephalitis had abnormalities
on EEG[6]. Another study on 37 patients with Bickerstaff’s brainstem
encephalitis reported abnormalities at 23% and 50% for brain MRI and
EEG, respectively[7]. Thus, brain MRI could not detect abnormalities
in more than two-third of the patients with Bickerstaff’s brainstem
encephalitis. As most cases of Bickerstaff’s brainstem encephalitis
show no abnormal lesions on brain MRI, functional imaging tools such
as PET could be useful to document CNS involvement [8].According
to the epidemiological study in Japan, similar to our case, 56% of the
patients with Bickerstaff’s brainstem encephalitis showed less than 5/
mm3 of CSF cell count and 20% showed more than 50/mm3 of CSF
cell count [7]. In the study by Odaka et. al., most patients with BBE
were given immunotherapy, such as steroids, plasmapheresis, and
IVIg. [9] Fox et al. have suggested that plasmapheresis and IVIg have
a beneficial effect in patients with BBE. [10]. Treatment with either
intravenous immunoglobulin or plasma exchange as both have been
established as efficacious in improving outcome based on randomised
control trials in GBS. As seen in our case child showed improvement
with IVIG and recovered completely.
Conclusion
Alternative diagnosis should be kept in mind when neurogenic
snakebite cases did not showed improvement with conventional
treatment (ASV). Complete neurological examinations should be
performed in all case of suspected snake bite before giving ASV to
ruled out GBS like illness.In any case of acute brainstem dysfunction
especially after infectious etiology, BBE should be suspected. MRI
brain,CSF analysis and presence of Anti GQ 1 antibody are aid to
diagnosis of BBE. Early detection and timely intervention plays
pivotal role in achieving remarkable recovery.
References
Citation
Meghana BL, Jain MK, Patnaik S, Sahoo B, Behera MR, et al. Bickerstaff Brainstem Encephalitis Masquerading As Snake Bite: A Case Report. Indian J Neurol. 2024;5(1): 131.