Case Report
A Case of Isolated Adie’s Pupil in Herpes Zoster Ophthalmicus
Soveeta R1*, Neha K2, and Suman T1
1Department of Paediatric Ophthalmology and Strabismus and Neuro-ophthalmology. Dr Shroff’s Charity Eye Hospital, New Delhi, India.
2Department of Cornea and ocular surface. Dr Shroff’s Charity Eye Hospital, New Delhi, India
*Corresponding author: Soveeta Rath, Department of Pediatric Ophthalmology, Strabismus and Neuro-ophthalmology, Dr Shroff’s Charity Eye Hospital, New Delhi, India. E-mail: soveetarath1@gmail.com
Article Information: Submission: 21/09/2023; Accepted: 06/11/2023; Published: 09/11/2023
Copyright: © 2023 Soveeta R, et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
We report a case of isolated internal ophthalmoplegia in a 32-year-old female who presented to us 6 weeks after the cutaneous manifestations of Herpes zoster. She presented with diminution of vision and severe photophobia due to right pupil anisocoria that responded to dilute pilocarpine test. She was symptomatically better after the test and was prescribed the same for 2 months, during which there was recovery of cutaneous lesions. In the subsequent visits, her anisocoria had reduced and she was asymptomatic.
Tonic pupil following viral infections can occur due to ciliary ganglion involvement. However in most cases of Adies pupil, it remains idiopathic. Internal ophthalmoplegia in herpes zoster ophthalmicus without any other ocular manifestations is rarely reported.
Introduction
Adies pupil was first reported by William John Adie in the year
1931 as a case of tonic pupil. It is usually seen in young female of 20-
40 years of age, unilateral in 80% of cases. It presents with difference
in size of pupil, noted by the patient or with usual complaints of
photophobia, difficulty in near work or blurring of vision. The
common signs remain absence of light reflex, better constriction to
accommodation, vermiform movements of the pupillary border,
and hypersensitivity to 0.125% pilocarpine. It is actually reported
to occur following infections, tumours, autoimmune diseases, and
trauma though it can also be associated with systemic diseases with
autonomic dysfunction. The site of insult in majority is damage to
the ciliary ganglion and its parasympathetic postganglionic fibres.
Hepatitis, Neurosyphilis, COVID-19, Leprosy, herpes zoster are few
of the associated aetiologies of Adie’s pupil [1,2]. Though Herpes
remains a common virus affecting the eye, tonic pupil in relation to
this has been less commonly described. In this case Adies tonic pupil
remains the isolated ocular finding in a young female with herpes
zoster [3].
Case Report
A 32 year old female presented to us with the complaints of
worsening of vision in the right eye (RE) associated with photophobia
since 1 week. She had a history of excruciating pain followed by skin
rash around the eye and on the right side of the forehead extending till
tip of nosesince 5 weeks consistent with the diagnosis of herpes zoster
ophthalmicus (HZO). [Figure 1] She was started on oral Acyclovir
(800 mg, five times a day) within 24 hours of skin rash onset and
maintained for 1 week, with improvement of her symptoms. She
denied any other history of trauma, surgery or inflammatory disease.
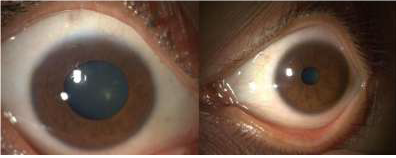
On examination her visual acuity was 6/18, N10 in the RE and 6/6 ,
N6 in the left eye. Pupil size in the RE was 8 mm compared to 3 mm
in the left eye (LE). [Figure 2] Though she was very symptomatic for

a detailed examination, consensual reflexes appeared intact in both
eyes. Extraocular motility and fundus examination was normal in
both eyes. In the examination of near reflex, the size of the left pupil
reduced slowly but not completely. Accommodation amplitudes
could not be done as patient refrained due to symptoms, however
she had difficulty in reading, possibly due to photophobia. Corneal
sensations were poor and rest anterior segment examination detected
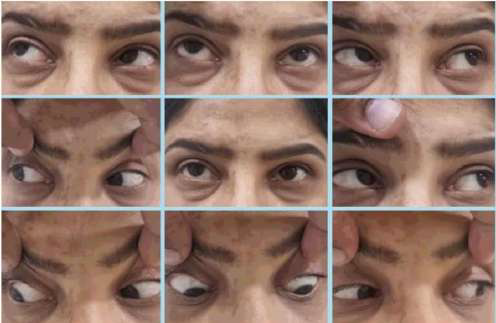
no abnormality in right eye. Vermiform movements could not
be appreciated. The extraocular motility appeared full, with mild
limitation of depression, though patient was not very co-operative.
[Figure 3]
A dilute pilocarpine test was done with 0.125% pilocarpine which
was positive showing constriction of pupil to 2 mm, improvement in
RE visual acuity to 6/6P, N6 and relief from photophobia.[Figure 4].
Laboratory blood tests and magnetic resonance imaging of brain and
orbit did not reveal any abnormality.
Adiagnosis of Adie’s pupil in HZO was made and dilute
pilocarpine was prescribed for 1 month.On her subsequent follow
up she reported to be symptomatically better and the anisocoria had
reduced to 4 mm from 8 mm in the right eye.Extraocular motility
appeared full and free 2 months post treatment and she remained
orthophoric. [Figure 5]. Posterior segment was normal in both eyes
throughout the course.
Discussion
Herpes Zoster Ophthalmicus (HZO), is a viral disease in older
adults, which occurs after reactivation of latent varicella-zoster
virus (VZV) present within the sensory spinal or cerebral ganglia.
It is characterized by a unilateral painful skin rash in one or more
dermatome distributions of the fifth cranial nerve (trigeminal nerve),
shared by the eye and ocular adnexa. Painful erythematous skin
lesions with macules, papules, vesicles, pustules, and crusting lesions


in the dermatome distribution and associated ocular findings strongly
suggest HZO [3].
Vesicular skin rash and scars in the forehead lids and lid adnexa, conjunctivitis, episcleritis and scleritis, keratitis, decreased corneal sensation, iridocyclitis, secondary glaucoma, retinal involvement, multiple ocular nerve involvement are the various manifestations of HZO [3].
Holmes Adie’s pupil is a type of pupil with parasympathetic denervation in which the affected pupil is large, poorly reacting to light, but reacting better to accommodation.
Vesicular skin rash and scars in the forehead lids and lid adnexa, conjunctivitis, episcleritis and scleritis, keratitis, decreased corneal sensation, iridocyclitis, secondary glaucoma, retinal involvement, multiple ocular nerve involvement are the various manifestations of HZO [3].
Holmes Adie’s pupil is a type of pupil with parasympathetic denervation in which the affected pupil is large, poorly reacting to light, but reacting better to accommodation.
Although most cases are idiopathic it mainly results from
inflammation or damage to the ciliary ganglion, and characterized by
a large regular pupil with decreased response to light but preserved or
enhanced constriction to accommodation, segmental iris constriction,
vermiform movements of the pupillary border, and hypersensitivity
to 0.125% pilocarpine [1,4].
Adie’s pupil in isolation has been reported rarely following HZO.
It definitely warrants careful evaluation as it may not be noticed in
the presence of the symptomatic skin lesions, which tend to be more
bothersome. A similar case of Holmes Adie’s pupil has been reported
in 2016 in a 35-year-old male which presented 3 months after the
onset of herpetic rash and was treated with dilute pilocarpine [5].
Karti et al has reported a case of isolated internal ophthalmoplegia
in a 27 year old female which did not respond to dilute pilocarpine
unlike in our case. However, they have reported positive constriction
to 2% pilocarpine, but the mydriasis persisted even at 4 months
follow up [6].
Pion and Salu have described a case of complete ophthalmoplegia
with Adie’s pupil in herpes zoster where the mechanism of cholinergic
hypersensitivity was considered a part of third nerve palsy [7].
The most common cause of Adie’s tonic pupil is infectious
diseases, most commonly Syphilis followed by immune related
disorders and paraneoplastic syndromes. In majority of the cases,
the primary cause should be evaluated and ophthalmic symptoms
improve after treatment of the primary cause [1]. However symptoms
like blurring of vision and photophobia is usually treated with dilute
pilocarpine.
In our case also the denervation hypersensitivity had set in at
the time of presentation and there was positive response to dilute
pilocarpine. In these cases the cholinergic super-sensitivity is
explained by the postganglionic parasympathetic denervation, which
leads to an up-regulation of the receptors at the nerve - sphincter
synapse. Adie’s tonic pupil is caused by acute denervation of the
ciliary body and iris sphincter.
Although total ophthalmoplegia has been reported in few cases in
association with herpes zoster, isolated internal ophthalmoplegia has
not been commonly reported.
Conclusion
Isolated anisocoria can be a presenting manifestation of herpes
zoster. In the presence of painful skin lesions, although a complete
ocular evaluation may be more demanding, yet it has to be done
carefully. Partial or complete , external or internal ophthalmoplegia
or both can be associated besides the corneal lesions. Anisocoria with
difficulty in reading and photophobia accelerates the discomfort,
thus needs prompt management.
References
Citation
Soveeta R, Neha K, Suman T. A Case of Isolated Adie’s Pupil in Herpes Zoster Ophthalmicus. Indian J Neurol. 2023;4(1): 125.