Case Report
Very Rarely Reported MRI Brain Changes - Spectrum of MRI Brain Changes in Serological Proven Case of Scrub Typhus Encephalopathy for Early Diagnosis
Sudhir S*, Kshipra K and Aravindh R
Department of Radiodiagnosis, Mahatma Gandhi Medical College and Research Institute, Sri Balaji Vidyapeeth University, Puducherry, Puducherry Union Territory, India
*Corresponding author: Sudhir Sachar, Department of Radiodiagnosis, Mahatma Gandhi Medical College and Research Institute, Puducherry. Email Id: sudhirsachar@gmail.com
Article Information: Submission: 24/08/2023; Accepted: 26/09/2023; Published: 29/09/2023
Copyright: © 2023 Sudhir S, et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction: Scrub typhus or bush typhus caused by Orientia tsutsugamushi is a common, zoonotic disease in South East Asia. Although CNS involvement in scrub typhus is well described but there are extremely rare documented studies of Brain changes in MRI in this infection. This is a case report of scrub typhus induced encephalopathy showing changes in Brain on MRI. The spectrum of MRI brain changes being reported by us is very important for scientific/medical community for correct early diagnosis and management, to save lives.
Methodology: Observational type of case study using 1.5 Tesla MRI. 45 years male presented with history of occipital headache for 5 days, projectile non-bilious vomiting and giddiness multiple episodes of upward rolling of eyes with loss of consciousness for few seconds and involuntary micturition. No known comorbidities. Patient is non-alcoholic, non-smoker, farmer by profession. Widal test was negative. Malaria and Dengue rapid card test - negative. Scrub typhus rapid card test - Positive for IgM antibodies (Inbios, USA). Spectrum of Brain changes on MRI: T2 and FLAIR images showed hyperintensity in head of bilateral caudate nuclei and in bilateral lentiform nuclei (more so in putamen). Also noted were mild bilateral hyperintensities in thalami on T2 and FLAIR (more evident on FLAIR). Lesions showed no restricted diffusion on DWI.
Conclusion: Based on the patient’s clinical and radiological characteristics, “Scrub Typhus Induced Encephalopathy” was diagnosed & it was confirmed serologically.
Methodology: Observational type of case study using 1.5 Tesla MRI. 45 years male presented with history of occipital headache for 5 days, projectile non-bilious vomiting and giddiness multiple episodes of upward rolling of eyes with loss of consciousness for few seconds and involuntary micturition. No known comorbidities. Patient is non-alcoholic, non-smoker, farmer by profession. Widal test was negative. Malaria and Dengue rapid card test - negative. Scrub typhus rapid card test - Positive for IgM antibodies (Inbios, USA). Spectrum of Brain changes on MRI: T2 and FLAIR images showed hyperintensity in head of bilateral caudate nuclei and in bilateral lentiform nuclei (more so in putamen). Also noted were mild bilateral hyperintensities in thalami on T2 and FLAIR (more evident on FLAIR). Lesions showed no restricted diffusion on DWI.
Conclusion: Based on the patient’s clinical and radiological characteristics, “Scrub Typhus Induced Encephalopathy” was diagnosed & it was confirmed serologically.
Keywords: Scrub Typhus Induced Encephalopathy; Mri,Thalami; Caudate Nuclei; Putamen.
Introduction
Scrub typhus is a well-known acute febrile illness caused by
Orientia tsutsugamushi. Scrub typhus is endemic in the tropical
and subtropical regions of the Asian continent. It is a re-emerging
infectious disease in India as well as in other parts of the world
like South Korea, northern China and Taiwan [9]. This disease has
multiorgan involvement, which includes lungs, heart, liver, spleen,
and central or peripheral nervous system [1-4]. Early diagnosis of
scrub typhus with CNS involvement is extremely important, as it can
alter the patient’s treatment, prognoses and reduce mortality rates
[4]. CNS involvement in scrub typhus has been described but there
are extremely raredocumented studies of MRI brain changes in this
infection [2].
Materials and Methods
Observational type of case study using 1.5 Tesla MRI. 45 years
male presented with history of headache (occipital region), severe
throbbing type with no aggravating and relieving factors since 5 days,
vomiting since 1day- 2 to 3 episodes, non-projectile, non-bilious and
containing food particles. Patient had giddiness 1 episode lasting
for 2 minutes (head spinning type, no postural variation). Multiple
episodes of upward rolling of eyes with loss of consciousness for
few seconds and involuntary micturition. Patient had decreased
appetite for 5 days, altered sleep. No complaints of photophobia, fever,
bleeding manifestations, chest pain, palpitations, rhinorrhoea, sore
throat, cough, abdominal pain and any abnormal movements. No
known comorbidities. Patient is non-alcoholic, non-smoker, farmer
by profession. No relevant family history. General examination within
normal limits. Systemic examination of CVS, RS and per abdomen
normal. CNS examination showed GCS- 15/15, Pupil 3mm - equally
reacting to light, Tone normal in all 4 limbs, Power 5/5 in all 4 limbs.
Plantar - flexor on sides and ankle, knee, biceps, triceps reflexes on
both sides are normal. X-ray chest and ECG were normal.
Hb - 10.8 g/dl, PCV - 34.3% (normal 40-50%) on admission
which later on showed improvement to Hb level 11.0 g/dl and PCV -
32.9% on discharge. Liver and renal function tests urine routine and
microscopy were normal. Widal test was negative. Malaria rapid card
test - negative. Dengue rapid card test - negative. Scrub typhus rapid
card test - Positive for IgM antibodies (Inbios, USA).
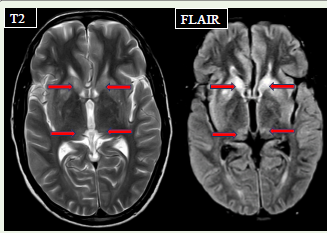
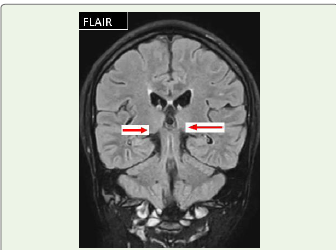
Spectrum of Brain Changes on MRI:
T2 and FLAIR images showed hyperintensities in head
of bilateral caudate nuclei& inbilateral lentiform nuclei (more
so in putamen). Also noted were mild bilateral hyperintensities
in thalami on T2 and FLAIR (more evident on FLAIR). Lesions
showed no restricted diffusion on DWI. These features were suggestive
of Scrub Typhus Induced Encephalopath.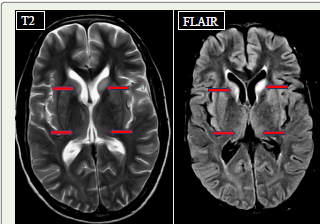
Discussion
Scrub typhus encephalitis syndrome has drawn public attention
in recent years [3]. The pathophysiology of scrub typhus is not
fully understood, though in general it is thought to be due to focal
or disseminated vasculitis. The target site of the organism is the
vascular endothelium [10]. Important neurological manifestations
of scrub typhus observed in many studies are mainly meningitis,
meningoencephalitis, seizures, and altered sensorium [1,7].
Neurological features accompany 20% of scrub typhus infections, and
may affect the central or peripheral nervous system, and sometime,
may even occur in combination [8].There is limited literature on
the neuroimaging findings of scrub typhus induced encephalopathy
[1,5]. In this study, patient who underwent neuroimaging, showed
abnormalities like T2-weighted and FLAIR hyper intensities in heads
of caudate nuclei, lentiform nuclei (mainly in putamen) and thalami,
indicating primary involvement of brain parenchyma [1]. However,
a radiologic diagnosis based on MRI findings was not easy before
because scrub typhus does not present typical features as reported
earlier [4,6].Though this study is limited by its size being a case report,
but it is not difficult to say that the imaging findings mentioned above
are helpful in diagnosis of scrub typhus as these have been seen in a
serologically proven case however larger studies on neuroimaging in
scrub typhus infections are warranted. Never the less the spectrum
of brain MRI findings in our case which on serology showed Scrub
typhus IgM +, indicate that these MRI brain findings are indeed very
helpful in suggesting the diagnosis of Scrub typhus encephalitis at the
earliest to institute proper therapy at the earliest to save life. The timely
instituted treatment after the diagnosis using Injection i.vDoxycycline
100 ml 8th hourly for 5 days, tablet Doxycycline 100 mg twice a day for
2 more days and tablet Azithromycin 500 mg OD for 5 days along with
other supportive medication made patient to recover.
Conclusion
Our patient presented with complaints of headache followed
by seizure and vomiting. Serological examination revealed Scrub
typhus IgM +.Radiological findings demonstrated involvement of
basal ganglia (heads of caudate nuclei, lentiform nuclei- mainly
putamen) and thalami. CNS involvement is not rare in scrub typhus;
thus, clinicians should carefully consider a patient’s complaints of
neurologic symptoms, including headache, dizziness, and drowsiness.
Recognizing typical radiologic findings as described in our case of
scrub typhus may be helpful in early diagnosis of scrub typhus with
CNS involvement, which may alter the treatment and prognoses of
patients.
References
Citation
Sudhir S, Kshipra K, Aravindh R. Very Rarely Reported MRI Brain Changes - Spectrum of MRI Brain Changes in Serological Proven Case of Scrub Typhus Encephalopathy for Early Diagnosis. Indian J Neurol. 2023;4(1): 120.