Research Article
Retrospective Observational Study of Series of Longitudinal Extensive Transverse Myelitis
Ojha P, Jagiasi K and Abhijeet Gaikwad*
Department of Neurology, Grant Government Medical College, Mumbai, India
*Corresponding author: Abhijeet Gaikwad, Department of Neurology, Grant Government Medical College, Mumbai, India
Email: abhijitgaikwad10491@gmail.com
Article Information: Submission: 18/05/2022; Accepted: 24/06/2022; Published: 27/06/2022
Copyright: © 2022 Ojha P, et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Abstract
Introduction: Longitudinally extensive transverse myelitis (LETM) is characterized by a contiguous inflammatory lesion of the spinal cord involving more
than 3 segments. It is most commonly associated with various acquired demyelinating diseases of the Central Nervous system. Clinical and Radiological
differentiation can help in diagnosis and predicting disease prognosis.
Materials and Methods: We did a Retrospective observational study to evaluate the Clinical and Radiological Characteristics of LETM cases and also
tried to evaluate the outcome.
Results: We observed All patients were presented with spastic Paraparesis or Quadriparesis depending on spinal cord level with predominant 13
(81.25%) patients with early bladder involvement & 2 patients (12%) presented with Brainstem Syndromes. Majority of which were found to be serum NMO
positive (60%) rest 40% equally distributed among Seronegative NMOSD, MOG and Idiopathic LETM. We found Predominately Thoracic cord (31%)& lower
cervical cord and thoracic cord (31%) involvement on MRI Spine with Characteristic Central Bright spotty lesion involving More than > 50 % of Areaon Axial
T2 Weighted scan in Seropositive NMOSD.2 patients (12 %) with NMOSD Showed Characteristic Brainstem involvement of MRI. We also spotted outpatients
who didn’t respond to Conventional immunotherapy 62% of them responded to Rituximabat a Mean follow of 18 months.
Conclusion: Longitudinally extensive transverse myelitis (LETM) has Characteristic Clinical & Radiological Presentations that need to be addressed.
We observed better results with Rituximab to non-responders to conventional immunotherapy.
Keywords
Longitudinally extensive transverse myelitis (LETM); Neuromyelitis Optica (NMO); NMO spectrum disorder (NMOSD); Myelin Oligodendrocyte
Glycoprotein Antibody (MOG)
Introduction
Longitudinally extensive transverse myelitis (LETM) is a
neurological condition characterized by a contiguous inflammatory
lesion of the spinal cord involving more than 3 segments [1]. it
is most commonly associated with the acquired demyelinating
disease of central nervous system diseases such as Neuromyelitis
Optica (NMO), NMO spectrum disorder (NMOSD), Myelin
Oligodendrocyte Glycoprotein Antibody (MOG ) [2]. Here we
tried to study the clinical and radiological profile of LETM patients
presenting to our tertiary institute and clinical outcome with various immunosuppressive therapy including rituximab.
Methodology
Here we collected details of 16 cases presented to our institution
over one year. Patients with long-segment myelitis of more than three
vertebral Segments involved on magnetic resonance imaging (MRI)
were included in the study.
All patients underwent detailed clinical neurological examination,
routine blood tests, serum autoimmune antibody (ANA), ANA
blot test, thyroid profile, and vitamin B12, Routine cerebrospinal fluid (CSF) analysis, Serum Aquaporin-4 antibodies (NMO-IgG)
and Myelin Oligodendrocyte Glycoprotein Antibody (MOG), CSF
analysis including cell count with differential, protein, glucose, the
Venereal Disease Research Laboratory (VDRL) test, immunoglobulin
G (IgG) index, and cytology. oligoclonal band (OCB).
All patient who has suspected demyelinating aetiology underwent
MRI brain with whole spinal cord screening with optic nerve study as
per demyelinating protocol.
Cases were included as per the Transverse Myelitis Consortium
Working Group. Proposed diagnostic criteria and nosology of acute
transverse myelitis Diagnosis of NMO / NMOSD was done as per
International consensus diagnostic criteria for neuromyelitisoptica
spectrum disorders [3,4].
Diagnosis of associated Optic Neuritis was done by Clinical
Presentation of visual Diminution and Ophthalmic evaluation as per
needed. Every Patient was evaluated by bedside evaluation, Fundus
copy and MRI Orbit plain and with Gadolinium contrast and Visual
Evoked potentials.
We analysed the clinical profiles of patients in real-world settings.
16 patient data we could compile with completeness in terms of
follow-up over the mean period of 18 months. We analysed the data
to determine factors significantly affecting the outcome in terms of
improved The Modified Rankin Scale (mRS) from 0 to 3. Simple
basic analysis was done using the excel function to describe our
findings. Categorical variables were compared using Fisher’s exact
test. All p-values were two-tailed, with values of < 0.05 considered
significant.
Results
Clinical characteristics:
In our sample, there was a high preponderance of female subjects
11 (68.75%) compared to male subjects 5 (31.25%). The mean age of
our patients was 31.00 years and the median also shows almost the
same value. To evaluate the groups, we divided all the subjects into
three categories based on age 15 years to 30 Years, 30-45 years and
those above 45. Roughly equal representation was seen in 15 to 30
years 8 subjects (50%) and 30 to 45 years 7 (43.75%) with one patient
in group >45 years.In our series of 14 patients (87.50 %) subjects were newly
diagnosed and 2 patients (12.50%) were presented with relapse from
previously attained functional level.
Patents were presented clinically as spastic quadriparesis or
paraparesis with sensory Involvement as per Level of spinal Cord
involvement. 13 (81.25%) patients were presented with bladder
involvement and the remaining 3 (18.75%) subjects had no bladder
complaints at presentation. More females 10 (62.25%) compared to
males 3 (18.75%), in our opinion, this preponderance is due to the
over-representation of female subjects.
In this series of subjects, we could see the optic neuritis in
3 (18.75%) subject’s rest of 81.25% of subjects did not have any
complaints related to optic neuritis.
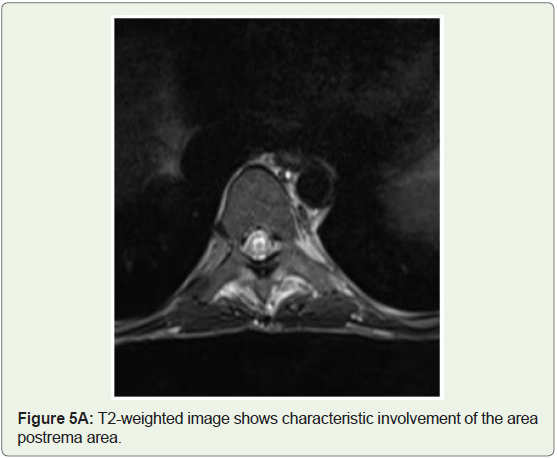
2 patients (12 %) presented with Brainstem Syndromes
accompanied by LETM.1 patient presented with diplopia, and bulbar
dysfunctions and another patient presented with Area postrema
syndrome in form of vomiting, Nausea and intractable hiccups.
Serological examination:
AQP4 antibodies were determined using a cell-based assay on
an AQP4-transfected cell line from a commercial BIOCHIP kit and
MOG antibody immunoglobulin G (IgG) is detected in serum, using
a cell-based assay (fluorescence-activated cell sorting)Majority of which were found to be serum NMO positive (60%)
rest 40% equally distributed among Sero negative NMOSD,MOG and
Idiopathic as 13.33% in each category.
MRI scanning:
Brain and spinal cord MRI scans were carried out for all patients
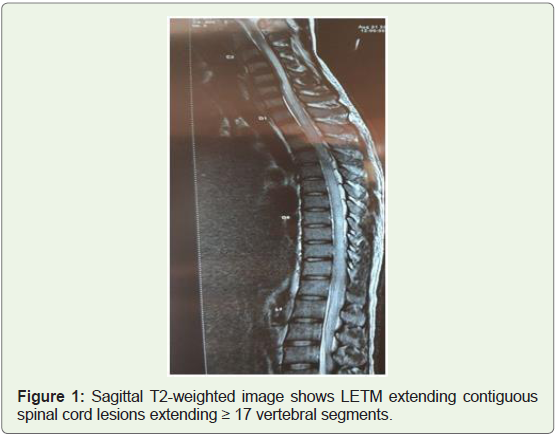
using a GE 1.5 T MR scanner.We found all patients were having 4 or more than 4 spinal cord
level involvement on T2 weighted images. Interestingly 2 patients
were With Holocord involvement as in Figure 1.
The average numbers of Segments involved in all patients were 7.
The most common presentation was equally distributed in the
Thoracic cord involvement 5 patient (31%) and 5 patients (31%) with
lower cervical cord and thoracic cord involvement. 3 patients(18% )
were presented with upper cervical cord involvement and 2 patients
(12%) with Holocord involvement as mentioned earlier and 1 (6%)
patient with Lumbosacral cord involvement.
We Found that out of 9 Seropositive NMOSD (60%), 4 patients
had Involvement of Lower Cervical cord with Thoracic cord
involvement, 2 patients had Holocord involvement, 2 patients had
Thoracic cord and 1 patient had upper Cervical Cord Involvement
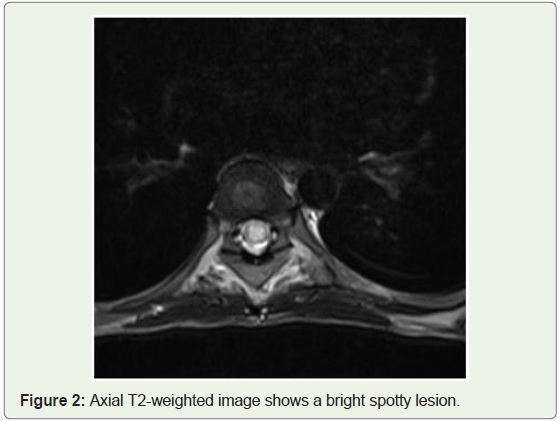
.6 Patient had Characteristic Central Bright spotty lesion involving
More than > 50 % of Area on Axial T2 Weighted scan (Figure 2).
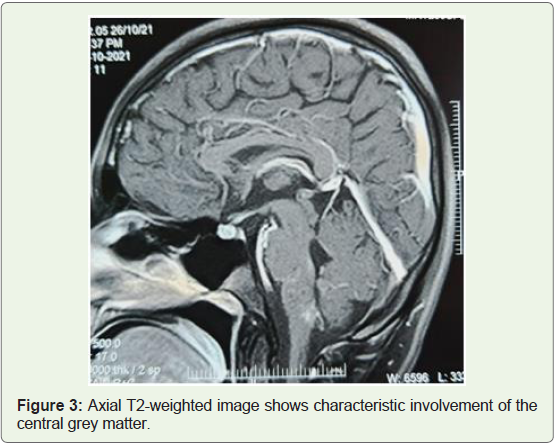
3 patients showed Predominately Grey Matter T2 weighted
Hyperintense signal on axial images as shown in Figure 3.
Amongst 2 (13%) Patients of NMOSD with Sero negative Status, 1
Patient had Lower Cervico thoracic with Thoracic Cord Myelomalacia
and another patient with Upper cervical cord involvement.
Amongst 2 MOG (13%) patients 1 patient has Lumbo sacral Cord
involvement and one patient with Thoracic Cord involvement.
2 Patients (13%) with Idiopathic Long Segment Transverse
Myelitis patient had Predominant Thoracic cord involvement.
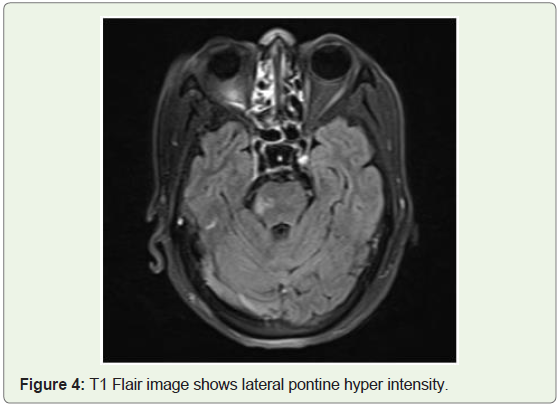
On Brain MRI imaging, 2 patients showed Significant Findings. 1
Patient with Seropositive NMO showed T2 weighted hyper intensity
in Lateral Pons Figure 4.
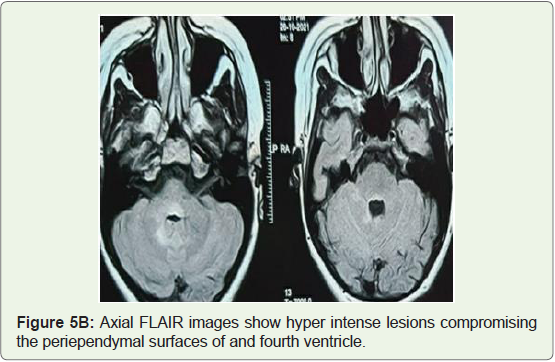
1 patient who was Seronegative NMOSD had T 2 weighted hyper
intensity in Area postrema and periependymal region as shown in
Figure 5 A&B.
Clinical Outcome:
We documented the treatment Received by Every patient. All
patients had Received 1 gm/day of Intravenous Methylprednisolone
for 5 days as initial Immunosuppressive therapy.3 patients Showed Improvement after initial Immunosuppressive
therapy and were maintained on Oral Prednisolone at a dose of 1mg /
Kg with a Second Immunosuppressant Oral Azathioprine at a dose of
1- 3 mg/kg. These patients showed significant modified Rankin scale
(mRS) improvement at a mean follow-up of 2 months only.
Amongst these 3 (19%) well responders, 2 patients were MOG
positive and one patient with NMO positive. All these patients were
presented within 7 days of onset.
13 patients who didn’t respond to initial Immunosuppression
therapy underwent 5 cycles of plasmapheresis. Those who did not
respond to conventional therapy including plasmapheresis were
given Rituximab at 2 gm iV loading as 1 gm iv 15 days apart and
maintenance dose at 6 monthly intervals. These Patients were
followed for a mean period of 18 months and Evaluated for outcome
in terms of Improvement in modified Rankin scale (mRS) from 0 to 3.
We found that 8 (62%) patients who received Rituximab showed
an Improved mRS scale at a Mean follow of 18 months. 2 patients
developed minimal and treatable complications in Form of Flare-up
of Herpes simplex and Urinary tract infection post-Rituximab. No
other significant complication was observed. Out of 8, 6 patients were
seropositive NMO and 2 were seronegative NMOSD.
As compared to conventional immunotherapy, Rituximab was
more effective in achieving improvement, at last, follow up with a
P-value of 0.02 ( P-value<0.05 significant)
We observed 5 patients who did not improve with any
immunosuppressive therapy including Rituximab. The majority of
these patients were Idiopathic 3 (60%) and 2 patients (40%) were
seropositive NMO.
Discussion
Long Segment transverse myelitis (LETM) is a rare entity. It is
characterized by a contiguous inflammatory lesion of the spinal cord
involving more than 3 segments. Contemplating differential diagnosis
it is very important to identify clinical radiological features remarking
causative factors. In this study, we try to evaluate the Clinical and
radiological characteristics of LETM and Its response to Conventional
immunotherapy and special consideration to Rituximab.
In our series of cases, the range of age of patients was 17 to 53
years with mean and median ages of 31.06 and 31.0 respectively. Most
patients as equal as 15 subjects fall into two categories of age 15 to 30
years 8 (50%) and 30 to 45 years 7 (43.75%) subjects, only 1 (6.25%)
subject was of the age of 70 years. This finding correlates with the
findings of other studies where most subjects fall between the age
group of 20-40 years (5). In our series, we found a 2.5:1 ratio of female
subjects compared to males.
In our series, most of the chunk is formed by Seropositive
NMOSD (60%) rest 40% equally distributed among Seronegative
NMOSD,MOG and Idiopathic as 13.33% in each category. It is
coherent with many series of LETM including 33 subjectsseries from
another part of India as well [6].
Patients with NMOSD presented With MRI spine changes of
Central Bright spotty lesion involving more than > 50 % of Area on
Axial T2 Weighted scan has been described as a characteristic MRI
finding in NMOSD with Predominately Grey matter T2 weighted
Hyper intense signal on the axial scan [7,8].
We observed Patients with NMOSD had prominent involvement
of Lower cervical and thoracic cord and Holocord involvement with an Average number of Segments involved were 7 these findings
overlap with findings mentioned by Sven Jarius et al [9].
A patient with MOG was presented with Characteristics MRI
features of Involvement of the Lumbosacral Cord segment as
described in the literature [10].
2 Patients with NMOSD Each from the seropositive and sero
negative group showing typical brainstem involvement defines the
core feature of NMOSD [11].
While observing the response to immunotherapy we found a
better response to conventional immunotherapy was found in MOGpositive
myelitis. This echoes from finding of Dubey et al (10).
In Non-responders conventional immunotherapy including
Plasmaphareis, Rituximab was more effective in achieving
improvement; at last, follow up with statically significance,
especially those presenting early in course of the disease. This
finding supplements the role of Rituximab in preventing permanent
Disability and relapses as described by previous studies in the Indian
population [12].
Rituximab which is a monoclonal antibody against CD20 Epitope
all B cells and depletes CD 20 +B and thus suppressing production
and antibodies including AQP4 [13,14].
In our studies, Rituximab was well tolerated without any
significant adverse effects.
Conclusion
Longitudinally extensive transverse myelitis (LETM) poses a
challenge needing clinical and radiological experience. Patients with
LETM present clinically with spastic Paraparesis or Quadriparesis
with early Bladder involvement. The majority of patients were
NMOSD with Predominately Thoracic cord & lower cervical cord
and thoracic cord involvement on MRI Spine with Characteristic
Central Bright spotty lesion involving More than > 50 % of Areaon
Axial T2 Weighted scan. We observed better results with Rituximab
to non-responders to conventional immunotherapy, particularly in
early disease presentation.
References
Citation
Ojha P, Jagiasi K, Gaikwad A. Retrospective Observational Study of Series of Longitudinal Extensive Transverse Myelitis. Indian J Neurol. 2022;3(1): 109.