Review Article
Management of Neuropsychiatric Symptoms of Anti-NMDA Receptor Encephalitis
Rathore U1*, Singhal M2, Yadav P3 and Asif AA4
1Sanjeevni Clinic, Indore, India
2MGM Medical College, Indore, India
3Grant Government Medical College, Mumbai, India
4University of Illinois College of Medicine, Peoria, USA
*Corresponding author: Rathore U, Sanjeevni Clinic, Indore, India Email: rathoreurvashi96@gmail.com
Article Information: Submission: 04/04/2022; Accepted: 07/05/2022; Published: 10/05/2022
Copyright: © 2022 Rathore U, et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Abstract
Introduction: Anti-NMDA receptor (NMDAR) encephalitis is a significant cause of novel autoimmune and paraneoplastic encephalitis,
Affect one out of 1.5 million people per year. Females are four times more affected as compared to males. Patients present with a prodromal
phase of constitutional symptoms followed by a spectrum of clinical manifestations eventually leading to death if left untreated. However,
rapid recognition and treatment can lead to survival and a return to the baseline level of functioning in most patients. It was diagnosed by the
presence of Anti-NMDAR antibodies that are directed to the extracellular domain of the GluN1 subunit in the CSF and serum.
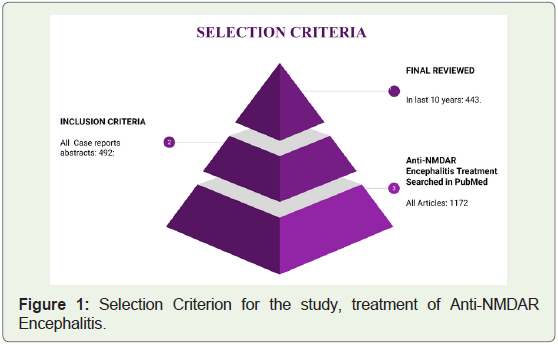
Methods: In this review article, we have examined the treatment of Anti-NMDA encephalitis in the past ten years, based on references
retrieved from PubMed, NCBI publications.
Result: Treatment of Anti-NMDAR encephalitis is based on first-line immunotherapy [corticosteroids, plasmapheresis, and intravenous
immunoglobulin] and second-line immunotherapy (rituximab and/or cyclophosphamide). Early treatment leads to rapid improvement in motor
skills, responsiveness, self-care, and speech, additionally in the paediatric population dramatic resolution of neurologic and psychiatric
symptoms was noted. In the case of complement deficiency, plasmapheresis was found to be highly effective. When first-line treatment
was ineffective, intravenous rituximab has shown noteworthy clinical improvement. In cases refractory to intravenous rituximab, the use of
intrathecal rituximab has shown marked improvement mainly associated with homozygous C4B deficiency. The use of cyclophosphamide
helped resolve movement disorder and brought significant improvement in the domains of cognition, language, and behaviour. When
given with rituximab it demonstrates remarkable improvement. in drug-resistant status epilepticus. Methotrexate, when given intrathecally
along with steroids showed tremendous improvement in some paediatric cases. Bortezomib has proven to be a reserve when secondline
immunotherapy is refractory. Electroconvulsive therapy reported a vigorous response in resolving neuropsychiatric symptoms. The
use of oral perampanel , an α-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid (AMPA) receptor antagonist, illustrated considerable
improvement in seizure activity and abnormal behaviour. Recently the use of ACTH therapy in patients with paralysis associated with choric
dyskinesia of limb recovered.
Conclusion: It was observed that early initiation of combined immunosuppressive therapy in higher dosage for a prolonged duration
shortens the clinical course and potentiates the possibility for complete recovery in the case of Anti-NMDAR Encephalitis. In the last decade,
only 9 drugs have shown some beneficial effects. Therefore, further studies which involve more participants and evaluate newer medications
are needed.
Keywords
Anti-NMDAR Encephalitis; Neuropsychiatric symptoms; Rituximab; Bortezomib; Perampanel
Introduction
Anti-NMDA receptor (NMDAR) encephalitis is a significant
cause of novel autoimmune and paraneoplastic encephalitis. Although
this is a rare disease, one affected out of 1.5 million people per year
but is the most common cause of non-viral encephalitis. Females are
four times more commonly affected as compared to males. Patients
present with a prodromal phase of constitutional symptoms followed
by a spectrum of clinical manifestations consisting of behavioural and
psychiatric symptoms, autonomic disturbances, movement disorders,
and seizures, even leading to death if left untreated. However, rapid
recognition and treatment can lead to survival and a return to the
baseline level of functioning in most patients and is based on a
multidisciplinary approach [1]. Diagnosis of the disease is confirmed
by the presence of Anti-NMDA receptor Antibodies, these antibodies
are directed at the extracellular domain of the GluN1 subunit in the
CSF and serum. Anti NMDAR encephalitis was previously known
to be associated with teratoma but recent studies have shown its
relationship with other tumours and autoimmune diseases [2]. In
this review article, we have examined the treatment of Anti-NMDA
encephalitis in the past ten years, it is based on references retrieved
from PubMed publications [3] (Figure 1).
Review
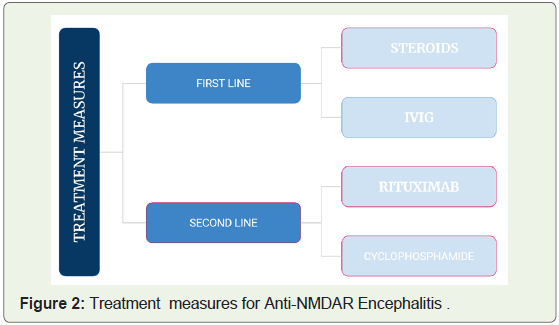
Treatment of Anti-NMDA encephalitis is based on first-line
immunotherapy (corticosteroids, plasmapheresis and intravenous
immunoglobulin) and second-line immunotherapy (rituximab
and/or cyclophosphamide) [4,5,6]. Treatment with steroid
(methylprednisolone) and intravenous immunoglobulins (IVIG)
leads to rapid improvement in motor skills, responsiveness, self-care,
and speech, additionally in the paediatric population with the use of
cyclophosphamide dramatic resolution of significant neurologic and
psychiatric symptoms was noted [7,8]. In the case of complement
deficiency, plasmapheresis was found to be highly effective [9,10].
When first-line treatment was ineffective, intravenous rituximab has
shown noteworthy clinical improvement [11]. In cases refractory
to intravenous rituximab [12], the use of intrathecal rituximab has
shown marked improvement [13,14]. Besides, this therapy was also
found to be helpful in Anti-NMDA encephalitis associated with
homozygous C4B deficiency. The use of cyclophosphamide helped
resolve movement disorder and brought significant improvement in
the domains of cognition, language, and behavior. Cyclophosphamide
when given with rituximab in drug-resistant status epilepticus
demonstrated remarkable improvement [15]. A promising alternative
immunomodulator was methotrexate when given intrathecally in
combination with steroids showed tremendous improvement in
some paediatric cases of Anti NMDAR encephalitis. Bortezomib
(proteasome inhibitor) proved to be a useful reserve when secondline
immunotherapy is refractory [16,17,18] (Figure 2).
Electroconvulsive therapy reported a vigorous response in
resolving neuropsychiatric symptoms such as catatonia [19],
especially in the paediatric population [20,21]. In a few studies use
of oral perampanel, an α-amino-3-hydroxy-5-methyl-4-isoxazole
propionic acid (AMPA) receptor antagonist, illustrated considerable
improvement in seizure activity and abnormal behavior [22]. Some patients with paralysis associated with choric dyskinesia of limb in
cases of Anti-NMDA encephalitis recovered with the use of ACTH
therapy [23].
Conclusion
Early initiation of combined immunosuppressive therapy which
includes both first and second line in higher dosage for a prolonged
duration shortens the clinical course and potentiates the possibility
for complete recovery in the case of Anti-NMDAR Encephalitis [24].
There have been many new drugs used for the resolution of various
symptoms in the past decade in total 9 medicines have shown some
beneficial effects. However, other than 4 drugs including first-line
immunotherapy [corticosteroids, plasmapheresis, and intravenous
immunoglobulin] and second-line immunotherapy (rituximab and/
or cyclophosphamide) no other drug is approved. Further studies
which involve more participants and evaluate newer medications are
needed.
References
Citation
Rathore U, Singhal M, Yadav P, Asif AA. Management of Neuropsychiatric Symptoms of Anti-NMDA Receptor Encephalitis. Indian J Neurol. 2022;3(1): 108.