Research Article
The Role of Statins in Stroke Management
Mahamankar A1*, Sonawane A2, Kotwal S3, Ramkumar R4 and Kannan S5
1Aditya Nursing Home, Mahad, Raigad, Near Shivaji Chowk, Maharashtra – 402301, India
2Sarthak Health Clinic, Near Shatabdi Hospital, Mumbai Naka, Renuka Nagar, Nashik, Maharashtra – 422001, India
3Government Medical College, Jammu, India
4Kamakashi Hospital, Pallikaranai, Chennai-600100, India
5NH Hospital, 258/A, Hosur Road Anekal Taluk, Bommasandra Industrial Area, Bengaluru, Karnataka 560099, India
*Corresponding author: Mahamankar A, Aditya Nursing Home, Mahad, Raigad, Near Shivaji Chowk, Maharashtra –
402301, India, Mobile : +91 9860996012, E-mail: dradityamhamnkar81@gmail.com
Article Information: Submission: 16/08/2021; Accepted: 23/09/2021; Published: 27/09/2021
Copyright: © 2021 Mahamankar A, et al. This is an open access article distributed under the Creative Commons
Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the
original work is properly cited.
Abstract
Stroke is the second leading cause of death globally. Statins are the preferred drugs for management of dyslipidemia, a major risk factor for atherosclerosis.
In addition to their cholesterol-lowering effects, statins have been shown to have pleiotropic effect of being antithrombotic, anti-inflammatory, and providing
endothelial protection. The present review was performed to assess the role of statins in the prevention and management of stroke.
A PubMed search was conducted with the search terms ‘statins’ and ‘stroke’ for randomized controlled trials published between 2010 and 2020.
Abstracts were screened and relevant articles were selected. A search was then conducted on PubMed and Google Scholar with the search terms ‘statins’,
‘stroke’, ‘primary prevention’, ‘secondary prevention’, between 2010 and 2020 and relevant articles were selected. In a backward chronological search, the
reference lists of all the selected articles were checked and other relevant articles were selected. The selected papers were used to evaluate the role of statins
in the prevention and management of stroke.
The narrative review discusses the role of statins in primary and secondary prevention of stroke, role of intensive statin therapy and the economic
implications of statins for the prevention of stroke.
It was concluded that statins have known role in reducing cholesterol levels, and primary and secondary prevention trials have time and again shown
the beneficial effects of statins in the prevention and management of stroke. Treatment with statins could be more cost-effective if low-risk patients are
aggressively treated, and guidelines consider the therapy for a broader patient population.
Keywords
Stroke; Statins; Ischemic stroke, Cardiometabolic stroke, Primary prevention, Secondary prevention
Introduction
A cerebrovascular accident (CVA), or an acute stroke, is also
termed a ‘brain attack’ [1
]. The aging population and the accruing
risk factors on a global level, are contributing to an increasing risk
of stroke. The Global Burden of Disease 2016 Lifetime Risk of Stroke
Collaborators stated that there has been a relative increase of 8.9% in
the lifetime risk of stroke from 1990 to 2016 [2
]. Additionally, stroke is the second leading cause of death globally, after ischemic heart
disease [3].
It is estimated that close to 17 million people succumb to
cardiovascular diseases (CVDs), especially heart attacks and strokes,
each year. A vast majority of these deaths can be attributed to tobacco
smoking, which tends to heighten the risk of death from coronary
heart disease and cerebrovascular disease by about 2-3 times [4].
Additionally, there is a close link between cardiovascular diseases
and cerebral perfusion. Any cardiac pathology can play a role in
raising the risk of stroke. A stroke may often be the first presentation
of an unidentified cardiac disorder [5]. While heart diseases can
increase the risk of stroke, acute stroke may also lead to cardiac
injury. Around 85% of all cases of stroke are ischemic while 15% are
hemorrhagic strokes [5].
Coronary artery disease and stroke are known to share common
risk factors. Hypertension is the most significant risk factor for both
ischemic and hemorrhagic stroke. Other common risk factors for
stroke include cardiac disease, particularly atrial fibrillation; diabetes;
smoking; abdominal obesity; diet; physical inactivity; alcohol; raised
apolipoprotein ApoB/ApoA1 ratio; and psychosocial factors [5].
Considering the enormous burden that the incidence of stroke
poses on individuals and healthcare systems, it is important to
consider stroke prevention and management early. Stroke prevention
is aimed at reducing stroke incidence by modification of risk factors.
Prevention can be categorized into primordial prevention, primary
prevention and secondary prevention. Primordial prevention deals
with lifestyle modification and includes efforts encouraging smoking
cessation, healthy diet, increased physical activity, and weight control.
Primary and secondary stroke prevention deal with an individual’s
specific lifestyle-related and medical risk factors, such as hypertension
and diabetes [6].
Statins are the preferred drugs for management of dyslipidemia,
a major risk factor for atherosclerosis. Besides their cholesterol lowering
effects, statins have been shown to have pleiotropic effects of
being antithrombotic, anti-inflammatory, and providing endothelial
protection [7].
This narrative review aims to discuss the role of statins in the
prevention and management of stroke and the economic implications
of statins for the prevention of stroke.
Methodology
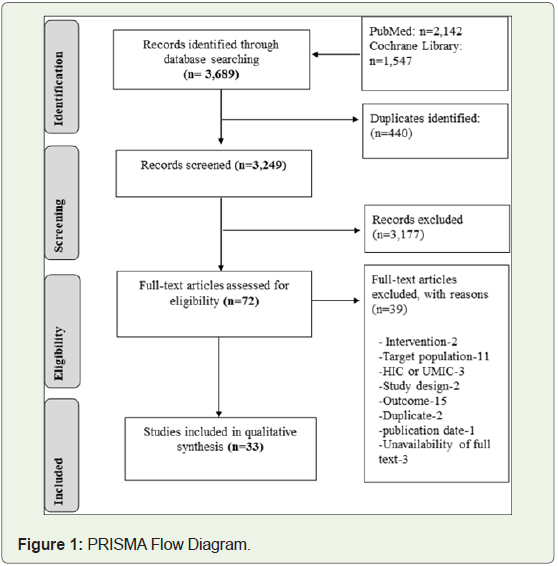
A review of published literature was conducted to determine
the role of statins in the prevention and management of stroke. A
PubMed search was conducted with the search terms ‘statins’ and
‘stroke’ for articles published between 2010 and 2020 and the search
returned 370 results (all randomized controlled trials). Abstracts of
these articles were checked and 9 of these were selected. A search was
then conducted on PubMed and Google Scholar with the search terms
‘statins’, ‘stroke’,‘primary prevention’, ‘secondary prevention’,and
the search duration was 2010 to 2020. The abstracts of the searched
articles were scanned and final articles were then identified and
selected. In a backward chronological search, the reference lists of all
selected articles were checked for citations that could not be detected
in the primary search and relevant articles were selected (Figure 1).
Information from the selected articles was extracted and an
analysis of the selected articles was then conducted by the investigators.
Data were extracted after reading the article. Both primary literature
and gray literature were screened and selected for the purpose of the
review article.
A narrative review was developed based on themes identified on
the analysis of the selected articles.
Results and Discussion
A total of 48 articles were selected. The themes that surfaced after
the analysis of selected literature included role of statins in primary
and secondary prevention of stroke, role of intensive statin therapy
and the economic implications of statins for the prevention of stroke.
Statins in primary prevention of cerebrovascular accident:
Raised cholesterol levels are known to heighten the risk for
cardiovascular disease, including stroke. Atherosclerosis is a chronic
inflammatory disease, with hypertension, raised lipid levels, diabetes,
and smoking is the main risk factors [8]. A plaque builds up in the
walls of the arteries, causing their narrowing and making it harder for
blood to flow. If a blood clot is formed, it stops the blood flow, causing
a heart attack or stroke [8].Therefore, interventions to decrease cholesterol levels are
often resorted to in order to reduce the risk. Statins have proven
effect in cholesterol lowering and hence, are often used to prevent
cardiovascular events in patients at high risk [9].
While low-density lipoprotein cholesterol (LDL-C) lowering
appears to be the leading mechanism by which statins reduce stroke
events, additional factors also play a role in stroke reduction. These
cholesterol-independent actions have additional cardiovascular
benefits [10].
Statins decrease serum cholesterol level as they inhibit
hydroxymethylglutaryl-coenzymeA (HMG-CoA) reductase [11].
Statins are also known to have pleiotropic effects that tend to
mediate their beneficial effects. Statins have been reported to have
a neuroprotective effect and also improve recovery after stroke [9].
Besides reducing LDL-C levels, statins have the properties of plaque
stabilization and endothelial homeostasis; have anti-inflammatory,
antioxidant, anti-proliferative and immunomodulatory effects; and
prevent platelet aggregation [12].
Therefore, in addition to their cholesterol-lowering effects, the
beneficial effects of statins on stroke reduction could be attributed to
their pleiotropic benefits.
Treatment with 3-hydroxy-3-methylglutaryl coenzyme A reductase
inhibitors, i.e., statins, has been shown to reduce the risk of
stroke in patients at high risk for atherosclerosis. Leading guidelines
recommend the use of statins, besides lifestyle modification, for the
primary prevention of stroke, particularly ischemic stroke, in patients
with a high 10-year risk for cardiovascular events [13]. Although they
were primarily employed to improve cardiovascular outcomes in
patients with known coronary artery disease, the use of statins has
now become increasingly common in people at low cardiovascular
risk. Tonelli and colleagues conducted a comprehensive systematic
review of the implications of statin use among low cardiovascular risk
individuals, including indirect comparisons of high-potency and lowpotency
statins [14]. They evaluated the effects of statins for primary
prevention in people at low cardiovascular risk. With 29 trials
including 80,711 participants in the analysis, patients treated with
statins had a significantly lesser likelihood than controls of having
nonfatal stroke (relative risk [RR] 0.81, 95% confidence interval [CI]
0.68-0.96), as well as myocardial infarction (RR 0.64, 95% CI 0.49–
0.84). All-cause mortality was found to be significantly lower among
those who received a statin compared to controls. Low- as well as
high-potency statins could prevent death and cardiovascular-related
morbidity in individuals at low risk of cardiovascular event [14].
On similar lines, the Cholesterol Treatment Trialists’ (CTT)
Collaborators had conducted a meta-analysis with 27 randomized
trials to assess the impact of lowering LDL-C with statins in people
at low risk of vascular disease. They noted that in participants with
5-year risk of major vascular events <10% (RR per 1.0 mmol/L
LDL-C reduction 0.76, 99% CI 0.61-0.95, p=0.0012), the reduction in
risk for stroke was similar to that observed in higher risk categories
(trend p=0.3). The meta-analysis suggested that lowering LDL-C with
standard statin therapy led to a reduction in the 5-year incidence
of major coronary events, coronary revascularizations, as well as
ischemic strokes by about one-fifth for every 1.0 mmol/L reduction
in LDL-C [15].
Investigators for the landmark trial - Justification for the Use of
statins in Prevention: an Intervention Trial Evaluating Rosuvastatin
(JUPITER) - noted that the previous primary prevention trials of
statin therapy using the cholesterol criteria for enrolling patients did
not report significant reductions in stroke risk. The investigators thus
assessed if statin therapy could reduce stroke rates among individuals
with low cholesterol but raised high-sensitivity C-reactive protein
(hs-CRP). They evaluated 17,802 apparently healthy individuals with LDL-C levels <130 mg/dL and hs-CRP levels >2.0 mg/L. Participants
were randomized to receive rosuvastatin 20 mg daily or placebo and
followed-up for the occurrence of a first stroke. Statin therapy led to a
48% reduction in the hazard of fatal and nonfatal stroke, following a
median follow-up of 1.9 years (maximum, 5.0 years), in comparison
with placebo, for an incidence rate of 0.18 and 0.34 per 100 personyears
of observation, respectively (hazard ratio 0.52; 95% confidence
interval, 0.34 to 0.79; P=0.002). This was attributed to a 51% decline
in the rate of ischemic stroke (hazard ratio, 0.49; 95% confidence
interval, 0.30 to 0.81; P=0.004). There was no difference in the rates
of hemorrhagic stroke between the active and placebo groups (hazard
ratio, 0.67; 95% confidence interval, 0.24 to 1.88; P=0.44). Statin
therapy, therefore, reduced the incidence of ischemic stroke by over
50% among individuals with low levels of LDL-C who were at risk on
account of elevated levels of hs-CRP [16].
Considering the limitations of several trials for not being able
to determine the difference in individual endpoints, ameta-analysis
was designed by Chan et al with the aim to have the required
power to identify a difference for individual endpoints, including
stroke events, major coronary events, and deaths related to CVD or
coronary heart disease (CHD), and evaluate drug-related adverse
events in studies looking into the results of intensive lipid lowering
by statins. The findings revealed that among individuals at high risk of
cardiovascular events, intensive lipid lowering with statins to LDL-C
level <2.1 mmol/l led to a significant reduction in risk of stroke, major
coronary events and CVD or CHD deaths compared to LDL-C level
≥ 2.1 mmol/l. In the intensive treatment arm, the odds ratio (OR) for
stroke was 0.80 (95% CI 0.71-0.89), for major coronary events was
0.74 (95% CI 0.65-0.83), and for CVD or CHD deaths was 0.84 (95%
CI 0.74-0.95). The results of this meta-analysis took the evidence
further by showing that individual endpoints are reduced by using
high-dose statins to decrease LDL-C to <2.1 mmol ⁄ l [17].
Rheumatoid arthritis (RA) is a condition that is known to be
associated with increased risk of a cardiovascular event (CVE). The
role of statins in this patient population is not well understood.
Therefore, a recent randomized placebo-controlled trial assessed if
statin therapy is better than placebo for the primary prevention of
CVEs in RA patients. Investigators followed 3,002 patients (mean
age 61 years; 74% female) for a median of 2.51 years. The primary
end point comprised of a composite of cardiovascular death,
myocardial infarction, stroke, transient ischemic attack (TIA), or
arterial revascularization. Around 1.6% of the patients receiving
statin experienced a primary end point, compared to 2.4% of those
receiving placebo. Presumed ischemic stroke or TIA was noted in
0.4% of the patients receiving statin compared to 0.8% of the patients
in the placebo group. The trial suggested that statin therapy is safe
for primary prevention of CVEs in patients with RA and may confer
similar risk reduction in this population as in other populations [18].
Of note, there is a possibility that statin therapy might increase
the risk of hemorrhagic stroke. However, it has been noted that the
annual excess risk of hemorrhagic strokes per 1.0 mmol/L decrease in
LDL-C might be around 0.5 per 1000 people treated over a period of
5 years and it is noteworthy that statin therapy leads to a reduction
in overall stroke independent of the predicted risk. Therefore, an increase in hemorrhagic stroke risk is outweighed by the reduced
risk of ischemic stroke, besides reduction in other occlusive vascular
events and deaths, even in those with 5-year risk of major vascular
events < 5%.15
Additionally, in the JUPITER primary prevention trial, the
cardiovascular and mortality benefits of statin therapy outpaced
the diabetes hazard, including in subjects at high risk of developing
diabetes [19].
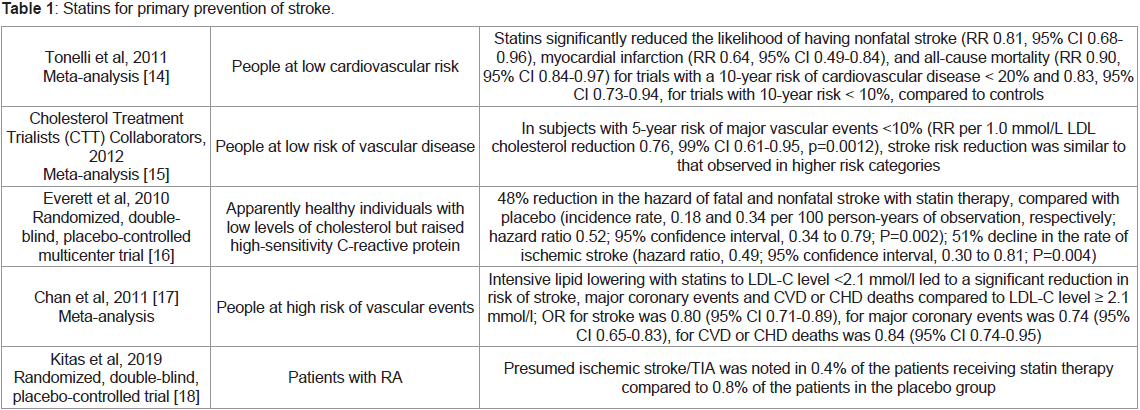
All the evidence that has been cited above thus seems to suggest
that statin therapy is an effective and safe treatment option for primary
prevention of stroke in different patient populations, and in low-risk
patients as well. Table 1 summarizes the findings from the articles
included in the review in terms of primary prevention of stroke.
Statins in secondary prevention of stroke:
Role of statins in ischemic stroke:
Statins are the recommended treatment option for primary and
secondary stroke prevention. Several large randomized, double-blind
trials have demonstrated that the use of statins in ischemic stroke
reduces the risk of incident and recurrent stroke [11].The 2013 American College of Cardiology/American Heart
Association (ACC/AHA) guideline also recommends the use of
statins for decreasing the risk of stroke and cardiovascular events
among patients with ischemic stroke or TIA that appear to have
atherosclerotic origin [20]. Statins have been shown to diminish the
incidence of ischemic stroke time and again. This finding emphasizes
on their non-cholesterol lowering effects as serum cholesterol is
poorly correlated with the risk for ischemic stroke [21].
The pleiotropic effects of statins on recurrent stroke are still not
clearly understood. Therefore, Kitagawa and colleagues assessedhs-
CRP levels during follow-ups with regard to stroke recurrence and
incident vascular events [22]. They studied the effects of statin therapy
on hs-CRP in ischemic stroke, and also looked into the impact of hs-
CRP on recurrent stroke and vascular events. In the statin group, hs-
CRP levels exhibited a significant reduction after 2 months (median
592 μg/L), and continued to be significantly lower till study end. In the control group, baseline hs-CRP was similar to the value after 2
months. Thus, in non-cardiogenic ischemic stroke, treatment with
statins may reduce vascular inflammation as evidenced by hs-CRP.22
of note, hs-CRP, a non-specific marker of inflammatory diseases, is an
independent risk predictor of cardiovascular diseases [12]. The study
by Kitagawa et al is the first to demonstrate the anti-inflammatory
effects of statins in a randomized larger-scale set up among patients
with chronic ischemic stroke. The data from this study support
guideline recommendations of statin treatments for the prevention of
stroke recurrence [22].
Additional evidence of the benefit of statins in reducing the
risk of ischemic stroke comes from a recent systematic review and
network meta-analysis including 9 trials which looked at randomized
controlled trials (RCTs) that evaluated statins in patients with
ischemic stroke or TIA up to July 2017. Statin therapy was tied to
a reduced risk of ischemic stroke, ischemic stroke or TIA, as well as
a cardiovascular event. The meta-analysis suggested that the use of
statins is safe [20].
A prospective cohort study included consecutive patients
diagnosed with an ischemic stroke and aimed to provide real-world
data for the associations between secondary prevention of stroke
and statin use. Patients without statin use had a greater risk of stroke
recurrence as well as worse functional outcomes. Those with poor
adherence to statins or discontinuation of the treatment had worse
prognosis after stroke while early onset of statin use was associated
with better outcomes. The study concluded that statins have a vital
role in treating ischemic stroke, preventing stroke recurrence and
cardiovascular events, and can also enhance functional performance
[23].
Accumulating evidence from trials like Stroke Prevention by
Aggressive Reduction in Cholesterol Levels (SPARCL) and Treat
Stroke to Target (TST) also support the role of lipid management
with statins in ameliorating ischemic stroke recurrence among
patients with a history of ischemic stroke or TIA [24].
Statins are known to improve outcomes after stroke. These agents
have been shown to improve infarct volume and neurological outcome
in animal models, though data from clinical studies have been inconclusive. The North Dublin Population Stroke Study, therefore,
explored the relationship between statin therapy and ischemic stroke
outcome. Investigators hypothesized that statin treatment initiated
prior to stroke onset and started acutely after ischemic stroke, would
lead to greater survival and improved functional outcome, and as
hypothesized, statin therapy at stroke onset and newly initiated statin
therapy were associated with improved early and late outcomes.
Logistic regression analysis, after adjustment for age, prestroke
disability (modified Rankin scale), National Institutes of Health
Stroke Scale (NIHSS) score, hypertension, and aspirin use, revealed
that new post-stroke statin treatment had an independent association
with improvement in early and late survival, in comparison with
patients not treated with statins. Similar findings could be seen for
statin therapy prior to stroke onset [25].
Flint and colleagues also assessed if statin use is tied to improved
discharge disposition after ischemic stroke. It was noted that statin
users, before and during stroke hospitalization, had higher odds of
having a good discharge outcome (OR for discharge to home = 1.38,
95% CI 1.25–1.52, p < 0.001; OR for discharge to home or institution
= 2.08, 95% CI 1.72–2.51, p < 0.001) [26]. A systematic review and metaanalysis
looking into the relationship between statin therapy and
outcome after ischemic stroke also revealed that statin therapy at
stroke onset was associated with improved outcome [27].
Besides being effective in secondary prevention of ischemic
stroke, statins are also a safe class of drugs. The most conservative
analysis has revealed that statins might have a link with an increased
relative risk of hemorrhagic stroke of about 50%. However, only a
minority of patients, i.e., <2%, would be exposed to the increased
risk, which would correspond to an absolute risk increase of only
0.6%. Interestingly, the raised risk of hemorrhagic stroke is primarily
attributed to data obtained from the SPARCL trial wherein there
seems to be a failure to maintain the integrity of the treatment
intervention over time. Therefore, the observation could possibly
be an artifact [20]. Additionally, Heo and colleagues assessed the
effect and safety of statin therapy in patients with acute stroke and
noted that hemorrhagic infarction or parenchymal/subarachnoid
hemorrhage occurred less often in the statin group compared to the
placebo group. Statin use was thus found to be safe and decreased
hemorrhagic transformation [28].
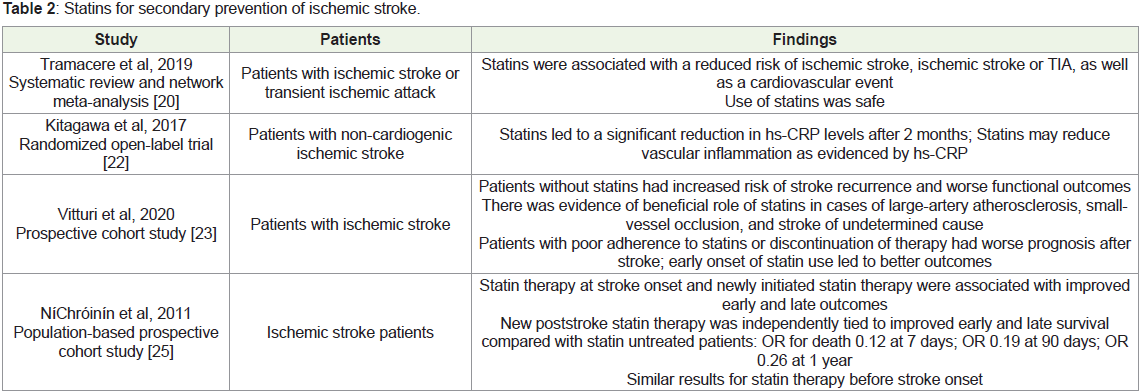
Available evidence therefore clearly points to the beneficial effects
of post-stroke statin therapy in ischemic stroke and suggest that they
are safe. Table 2 summarizes the findings from the articles included in
the review for secondary prevention of ischemic stroke.
Preventive and therapeutic role of statins in cardioembolic stroke:
Evidence is scarce on the administration of statins in patients with
cardioembolic stroke.Cardioembolic stroke appears to be associated
with atherosclerotic disease, either directly, such as in myocardial
infarction, or indirectly, such as in cases of atrial fibrillation (AF),
cardiomyopathy, and left ventricular wall thrombus. Statins appear to
have an impact on the outcomes of cardioembolic stroke [29].Atrial fibrillation is a risk factor for cardioembolic stroke. Statins
prevent AF, possibly by a reduction in inflammation, as markers such
as C-reactive protein are elevated in AF and are reduced by statins
[30].
Statins have pleiotropic effects on atherosclerotic plaque
stabilization. Collateral status in patients with AF-related stroke is
poor as emboli tend to block a large proximal artery. Use of statins
in AF patients has been shown to be linked with excellent collateral
flow [31]. However, there have been studies that advised against the
initiation of statin therapy in cardioembolic stroke patients unless
additional cardiovascular indications were present [32].
Therefore, this review evaluated the literature on the role of
statins in patients with cardioembolic stroke.
In a 2014 study, statin treatment was reported not to affect the
incidence of recurrent stroke in patients with cardioembolic stroke.
Choi and colleagues had assessed the effects of statin treatment on
mortality and stroke recurrence after cardioembolic stroke. Data
was evaluated from 535 patients with first cardioembolic stroke.
Statins were associated with reduced mortality. Treatment with
statins was shown to have an independent association with reduced
mortality (hazard ratio, 0.237; 95% confidence interval, 0.080–0.703
for nonstatin versus low-potency statin; hazard ratio, 0.158; 95%
confidence interval, 0.037–0.686 for nonstatin versus high-potency
statin). However, statin therapy had no effect on the incidence of
recurrent stroke [29].
Around the same time, Ntaios et al, in a long-term registry of
patients with AF-related stroke, noted that statin treatment improved
survival and decreased the risk for later cardiovascular events.
Consecutive patients from the Athens Stroke Registry with AFrelated
stroke without a prior history of coronary artery disease or
clinically manifest peripheral artery disease were part of the analysis.
Participants were segregated in two groups based on whether statin
was prescribed at discharge of 1602 stroke patients, 404 with AFrelated
stroke were included in the analysis. Of these, about 25.2%
were discharged on statin. Multivariate Cox-proportional-hazards
model revealed that statin therapy had an independent association
with reduced mortality and a diminished risk for the composite
cardiovascular endpoint over a median follow-up of 22 months, but
not with stroke recurrence [33].
A relatively recent study by Ko and colleagues evaluated the effect
of pre-stroke statin use on functional outcome in AF and noted that
statin use at time of stroke onset among these patients was associated
with less severe stroke. Pre-stroke statin use was tied to a 32%
reduction in frequency of severe stroke. So, statin use at the time of
stroke onset among patients with AF was shown to be linked to less
severe stroke in this study [34].
Another study has shown the benefit of pre-stroke statin use
[32]. Kotlęga and colleagues assessed the effects of pre-stroke statin
use on in-hospital outcomes and mortality in cardioembolic stroke
patients. The study recruited ischemic stroke patients with AF. Group
I (n=181) included patients who had been treated with statins directly
prior to the stroke. Group II (n = 153) was the non-statin group.
Patients in the non-statin group demonstrated greater initial and
discharge NIHSS scores. Statin group had a greater improvement in
NIHSS score. Additionally, in-hospital mortality was more frequently
reported in the non-statin group. So, despite the fact that statins are
predominantly used in atherothrombotic stroke patients, this study
revealed the benefits of statins in cardioembolic stroke patients [32].
Another recent study looked into the effect of statin therapy
for theprevention of the major vascular events in patients with
acutecardioembolic stroke without any other known indication for
statin therapy. Among 2,888 patients with cardioembolic stroke,
64.5% were on statin therapy while hospitalized. Following a median
follow-up of 359 days, patients given statin therapy had cumulative
incidences of major vascular events (a composite of stroke recurrence,
myocardial infarction, and vascular death) of 9.3% compared to
20.5% among those not given statins. The adjusted hazard ratios of
statin therapy for major vascular events, stroke recurrence, vascular
death, and all-cause death were 0.39, 0.81, 0.28 and 0.53, respectively.
The study thus revealed that statin therapy could potentially diminish
the risks of major vascular events, vascular death, and all-cause death
in patients with acute cardioembolic stroke with no clear indication
for statin therapy based on current guidance [35].
An exploratory subanalysis of the THRombolysis and Statins
(THRaST) study, among 701 patients diagnosed with cardioembolic
stroke at discharge revealed that statin use in the acute phase was
tied to neurological improvement, major neurological improvement,
favorable functional outcome, and a decreased risk of neurological decline and death. The study reinstated the role of statins within 72 h
after IV thrombolysis [36].
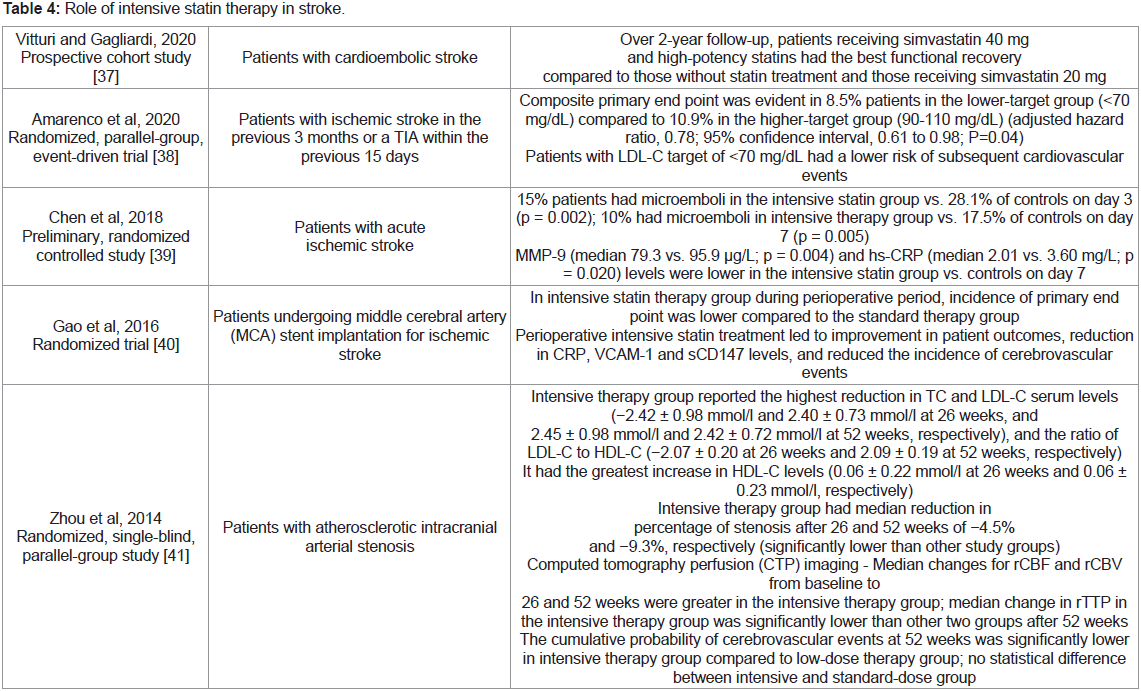
Vitturi and Gagliardi recently demonstrated that in patients with
cardioembolic stroke, statin use may be beneficial in some cases.
Patients in the study were divided into non-statin, simvastatin 20
mg, simvastatin 40 mg, and high-intensity statin (atorvastatin 40
mg or rosuvastatin 10 mg) groups. It was noted that statin therapy
may prevent stroke recurrence and improve functional outcomes in
these patients. There were 27 cases of stroke recurrence in the study (6
from the nonstatin group, 11 from simvastatin 20 mg group, 6 from
simvastatin 40 mg group, and 4 from the high-potency group) during
follow-up [37].
Statin use, therefore, has beneficial effects in cardioembolic stroke
patients, both as pre-stroke therapy and post-stroke intervention.
It can be stated that statins may act as effective adjuvant therapy
to improve the efficacy of thrombolytic therapy, on account of
their profibrinolytic and antithrombotic effects [36]. The use of statin
treatment after a cardioembolic stroke should be further explored in
randomized clinical trials [37].
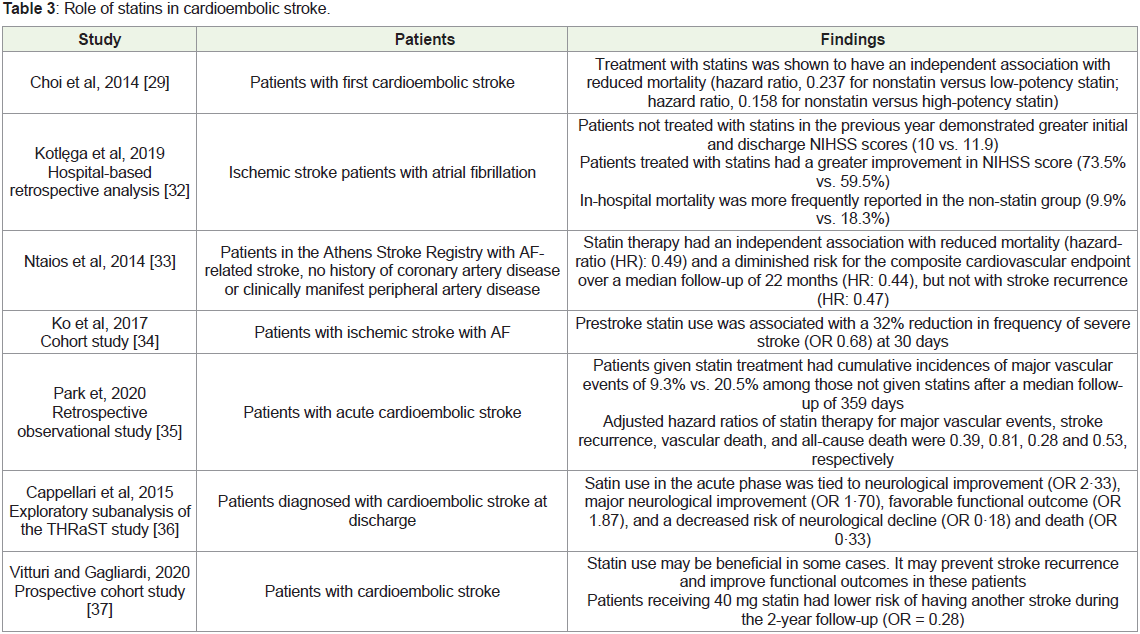
Table 3 summarizes the findings from the articles included in the
review on the role of statins in cardioembolic stroke.
Intensive statin therapy and CVA:
Intensive lipid-lowering therapy using statins is recommended
following a TIA or an ischemic stroke of atherosclerotic origin.
The recommendation is based on the findings from the SPARCL
trial showing a lower incidence of recurrent stroke by 16% with
atorvastatin 80 mg per day, compared to placebo in patients with
stroke and no proven coronary heart disease. The American Heart
Association and the American Stroke Association also advocate
intensive statin therapy after an ischemic stroke of atherosclerotic
origin [38].Ischemic stroke recurrence has usually been reported within 1
week of a minor stroke. Therefore, there is a particular significance of
early active treatment after ischemic stroke [39].
Intensive statin therapy has been shown to reduce the occurrence
of microemboli and inflammation in patients with acute ischemic
stroke [39]. Chen and colleagues conducted a study among patients
with acute ischemic stroke who were randomized to either intensive
statin therapy or control treatment within 72 hours of onset. They
noted that 58.3% patients had microemboli in the intensive statin
group compared to 52.6% in the control group on day 1. On day 3,
15% patient’s had microemboli in the intensive statin group compared
with 28.1% of controls. Metalloproteinase-9 (MMP-9), hs-CRP, and
NIHSS score were also evaluated on days 1 and 7. On day 7, MMP-9
and hs-CRP levels were lower in the intensive statin group compared
to control group. There appeared to be no overt adverse events and
the liver function of the included patients was not impacted. The
study made a strong suggestion that intensive statin therapy could be
safely used in patients with acute ischemic stroke [39].
Vitturi and Gagliardi assessed the effects of statins on the
neurological outcomes in patients following a cardioembolic stroke.
Simvastatin 40 mg treatment was tied to a significantly lower incidence of stroke recurrence in comparison with simvastatin 20 mg
and statin non-use. Simvastatin 40 mg and high-potency statins were
associated with the best functional recovery [37].
While intensive statin therapy is recommended following an
ischemic stroke of atherosclerotic origin, the ideal LDL target level
is not known. So, investigators in the Treat Stroke to Target trial,
investigated the hypothesis that a target LDL-C of <70 mg/dL would be
superior to a 90-110 mg/dL in reducing overall cardiovascular events
after an ischemic stroke or a TIA in patients with atherosclerosis. In
the randomized, parallel-group study in France and South Korea,
patients with ischemic stroke in the previous 3 months or a TIA
within the previous 15 days were randomized to a target LDL-C level
of <70 mg/dL(lower-target group) or to a target range of 90-110 mg/
dL(higher-target group). The composite primary end point of major
cardiovascular events, which included ischemic stroke, myocardial
infarction, new symptoms leading to urgent coronary or carotid
revascularization, or death from cardiovascular causes, was evident
in 8.5% patients in the lower-target group compared to 10.9% in the
higher-target group (adjusted hazard ratio, 0.78; 95% confidence
interval, 0.61 to 0.98; P=0.04). It was noted that patients with LDL-C
target of <70 mg/dL with the use of statins and, if needed, ezetimibe,
had a lower risk of subsequent cardiovascular events compared to
those who had a target range of 90-110 mg/dL [38].
The study by Chan et al, mentioned in a previous section in
this article, also suggested that among patients at high risk of
cardiovascular events, intensive lipid lowering with statin therapy to
LDL-C level <2.1 mmol/l significantly decreased the risk of stroke,
major coronary events and CVD or CHD deaths, in comparison with
LDL-C level ≥ 2.1 mmol/l.17
Data also suggest that perioperative intensive statin treatment
in patients undergoing stent implantation for ischemic stroke can
also improve patient outcomes [40]. A study evaluating intensive
statin therapy during perioperative period in patients undergoing
middle cerebral artery (MCA) stent implantation for ischemic stroke
evaluated serum levels of CRP, vascular cell adhesion molecule-1
(VCAM-1), and soluble extracellular matrix metalloproteinase
inducer (EMMPRIN/CD147) at 24 h before and 24 h after the
intervention. The study revealed that the primary end point
[procedure-related intra-stent thrombosis, 1-month incidence of
major adverse cerebrovascular events (stroke, transient ischemic
attack, in-stent restenosis, death or unplanned revascularization)]
occurred less often in intensive therapy group compared to the
standard therapy group. Perioperative intensive statin treatment led
to improvement in patient outcomes, reduced CRP, VCAM-1 and
sCD147 levels, and reduced the incidence of cerebrovascular events
[40].
A study by Zhou and colleagues evaluated the efficacy of
intensive statin treatment in patients with atherosclerotic intracranial
arterial stenosis (AICAS). Investigators assessed changes in serum
lipid profiles, degree of stenosis, perfusion-related parameters and
occurrence of cerebrovascular events during the study period. Patients
were randomized to receive low-dose, standard-dose statin therapy
or intensive-dose statin therapy. Fifty-two weeks following treatment,
there were significantly better improvements in serum lipid profiles,
degree of stenosis, and perfusion-related parameters in the intensive
therapy group. The cumulative probability of cerebrovascular events
was found to be significantly lower in the intensive treatment group
compared to the low-dose therapy group. In terms of serum lipid
profile, the intensive therapy group reported the highest reduction in total cholesterol (TC) and LDL-C serum levels (2.45 ± 0.98 mmol/l
and 2.42 ± 0.72 mmol/l at 52 weeks), and the ratio of LDL-C to highdensity
lipoprotein cholesterol (HDL-C) (2.09 ± 0.19 at 52 weeks).
This group also had the greatest increase in HDL-C levels (0.06 ±
0.23 mmol/l) among the three study groups. Intensive therapy group
had median reduction in percentage of stenosis after 26 and 52 weeks
of -4.5% and -9.3%, respectively, which was significantly lower than
other study groups. In terms of computed tomography perfusion
(CTP) parameters, median changes for relative cerebral blood flow
(rCBF) and relative cerebral blood volume (rCBV) from baseline to
26 and 52 weeks appeared to be greater in the intensive therapy group
and the median change in relative time to bolus peak (rTTP) in this
group was significantly lower than other two groups after 52 weeks
of therapy. The safety profile of intensive therapy was comparable to
that of the other therapies [41].
The available evidence, therefore, indicates that intensive lipid
lowering leads to stroke risk reduction in comparison with moderate
lipid lowering and has been found to be safe as well. High-intensity
statin treatment, therefore, appears to be beneficial for stroke patients.
Table 4 summarizes the findings from the articles included in the
review for the role of intensive statin therapy in patients with stroke.
Economic implications of statins for the prevention of CVA:
Numerous clinical trials and meta-analyses have shown that
statins are beneficial in reducing mortality and cardiovascular
morbidity in different populations and risk groups [42]. While in
developed countries, the majority of the individuals are insured or governments take care of healthcare expenditure of the people, in
developing countries like India, most of the healthcare expenditure
is out of the patients’ pockets [43]. It, therefore, seems prudent to
understand the economic implications of statin use.A study conducted by Chawan et al noted a wide variation in
the cost of different brands of oral hypolipidemic drugs available in
India [44]. Greving and colleagues evaluated the cost-effectiveness of
low dose statin therapy for primary prevention of vascular disease,
and noted that statin treatment was not cost-effective for primary
prevention in populations that had a low risk of vascular disease.
The study emphasized on the need to improve adherence to statin
treatment in order to improve the cost-effectiveness of these drugs for
primary prevention. Costs of treatment in this study were segregated
into those incurred by the drug, laboratory tests, doctors’ visits, and
pharmacists’ fees. All cost estimates were updated to 2008 with Dutch
consumer price indices. Cost-effectiveness analysis was done using a
Markov model. Incremental cost-effectiveness ratios were calculated
[42]. However, a later study noted that 5 years’ primary prevention
treatment of middle-aged men with a statin was cost saving.
Treatment of even younger, lower risk individuals appeared to be
cost-effective. In this study, the investigators assessed the costs and
benefits of the first 5 years of treatment with statin over the complete
follow-up period of approximately15 years in a cost-utility analysis.
The perspective of the National Health Service (NHS) for costs and
savings, and health benefits [quality-adjusted life years (QALYs) over
the follow-up period of 15 years] for patients were employed [45].
A study conducted in the Netherlands revealed that in spite of
nonadherence in actual practice, statin treatment was cost-effective for primary prevention among newly diagnosed type 2 diabetes
mellitus patients. In this study, cost-effectiveness analysis was
conducted with the help of a Markov model with a time horizon of
10 years. Investigators ascertained the difference in QALYs between
no lipid-regulating treatment and statin treatment [46]. A study from
Taiwan suggested that reducing the target LDL-C level to 70 mg/
dL among treatment-naïve coronary artery disease patients could
prove to be cost-effective. This study also used a Markov cohort statetransition
model to build up disease progression, understand the
health outcomes, and determine overall estimates of cost and QALY.
The direct costs and rate of fatal events were obtained from national
claims database. Incremental cost-effectiveness ratio (ICER) per
QALYs was calculated, and sensitivity analyses were conducted [47].
While treatment with statins has been shown to be cost-effective
in some studies, it could be more cost-effective for lower-risk patients
as drug prices decline. Clinicians should be more aggressive in treating
low-risk patients, and guidelines must consider recommending
therapy for a broader patient population [48].
Conclusion
Statins are a class of drugs with well-known role in reducing
the cholesterol levels, thereby decreasing vascular event incidence.
Primary and secondary prevention trials have often shown the
beneficial effects of statins in the prevention and management of
stroke. The pleiotropic benefits of statins, besides their cholesterollowering
effects, are accountable for their potential beneficial effects
in the management of stroke. Statins have been shown to be safe
and effective for primary prevention of stroke in several trials, such
as the JUPITER and the CTT trials. Pre-stroke and post-stroke
statin therapy has both been found to be effective in ischemic stroke
andcardioembolic stroke. Though statin treatment needs to be
explored further in cardioembolic stroke. Evidence also indicates that
intensive statin treatment is beneficial for stroke patients and appears
to be a safe option.
While there could be a wide variation in the cost of different
brands of lipid lowering drugs, treatment with statins could prove
to be more cost-effective if the clinicians aggressively treat low-risk
patients, and guidelines consider the therapy for a broader patient
population.
Declarations
Funding: The authors did not receive support from any
organization for the submitted work. No funding was received to
assist with the preparation of the manuscript.
Conflicts of interest/competing interests: The authors have no
conflicts of interest to declare that are relevant to this article’s content.
Author’s contributions
Aditya Mahamankar (AM): Conception and design, literature
search, data extraction of the relevant studies, drafting and critically
revising the article, and final approval of the version to be submitted.
Ashutosh Sonawane (AS): Literature search, data extraction of
the relevant studies, qualitative assessment of the eligible studies,
drafting and critically revising the article, and final approval of the
version to be submitted.
Suman Kotwal (SK): Data extraction from the relevant articles,
drafting and critically revising the article and final approval of the
version to be submitted.
R Ramkumar (RR): Conception and design, data extraction from
relevant articles, qualitative critically revising the article, and final
approval of the version to be submitted.
Subramanyam Kannan (SK): Literature search, data extraction of
the relevant studies, qualitative assessment of the eligible studies, final
approval of the version to be submitted.
References
Citation
Mahamankar A, Sonawane A, Kotwal S, Ramkumar R, Kannan S. The Role of Statins in Stroke Management. Indian J Neurol. 2021;2(1): 103.