Case Report
Saltzman Type III Persistent Trigeminal Artery: A Case Report and Review of Medical Literature
Benoît Nolet1, Rouillard-Bazinet N2 and Régis Olry3*
1Medical Faculty, University of Montreal, Quebec, Canada
2Department of Pediatric Otolaryngology, Assistant Professor, Centre Hospitalier Universitaire Sainte-Justine, University of Montréal, Québec, Canada
3Department of Anatomy, Full Professor, University of Québec at Trois-Rivières, Québec, Canada
Corresponding author: Régis Olry, Department of Anatomy, University of Québec at Trois-Rivières, C.P. 500, Québec, Canada, Tél: 819 376 5011; Fax: 819 376 5084; E-mail: regis.olry@uqtr.ca
Citation: Benoît Nolet, Rouillard-Bazinet N, Régis Olry. Saltzman Type III Persistent Trigeminal Artery: A Case Report and Review of Medical Literature. Indian J Neurol. 2017;1(1): 101.
Copyright © Régis Olry 2017. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Neurology | Volume: 1, Issue: 1
Submission: 05/08/2017; Accepted: 26/09/2017; Published: 05/10/2017
Abstract
The trigeminal artery belongs to a series of embryonic transient arteries referred to as persistent carotid-vertebrobasilar anastomosis. Since its anatomical discovery in the mid-nineteenth century and its first angiographic observation about a century later, many case reports of persistence of the trigeminal artery after birth and into adult life have been published, most of them being fortuitous angiographic discoveries. In this paper, we describe a new case of trigeminal artery we discovered during a gross anatomy course, and review its anatomical, epidemiological, and pathogenic features in the medical literature.
Keywords:
Brain vascularisation; Persistent carotid-vertebrobasilar anastomosis; Trigeminal artery; Amyotrophic lateral sclerosis
Abbreviations:
AICA: Anterior Inferior Cerebellar Artery; BA: Basilar Artery; ECA: External Carotid Artery; HA: Hypoglossal Artery; ICarA: Internal Carotid Artery; ICerA: Intersegmental Cervical Artery; PA: Proantlantal Artery; PCA: Posterior Cerebral Artery; PCoA: Posterior Communicating Artery; PICA: Posterior Inferior Cerebellar Artery; SCA: Superior Cerebellar Artery; TA: Trigeminal Artery
Introduction
The discovery of persistent carotid-vertebrobasilar anastomosis dates back to 1844 in gross anatomy and to 1950 in angiography [1,2]. Since that time, five different types of persistent carotidvertebrobasilar anastomosis have been described: the Trigeminal Artery (TA), Hypoglossal Artery (HA), Otic Artery (OA), Proatlantal Artery (PA), and Intersegmental Cervical Arteries (ICerA) (Table 1) [3]. Over 400 observations of persistent TA were published before 1982, but reports of TA found during gross anatomy dissection courses are very scarce [4,5]. We describe in this paper a new case to be added to those previously well documented, and discuss its place in our current knowledge of its features: Saltzman type, correlations with the classical epidemiological data and associated pathologies [6-12].
Table 1: First published observations of the five types of persistent carotidvertebrobasilar anastomosis.
Embryology of the cerebral vascular system
The embryological development of the vascular cerebral system begins very early, before the closure of the neural groove, and achieves its adult configuration at the 40 mm/52 days embryonic stage [13,14]. Both arterial systems supplying the encephalon, that is the bilateral ventral carotid axis and the dorsal longitudinal neural channels (the fusion of which giving rise to the basilar artery), are temporarily interconnected by more or less symmetrical anastomosis. In rostrocaudal order, these anastomoses are the trigeminal, otic, hypoglossal, proatlantal, and intersegmental cervical arteries. They appear at the 4-5 mm/29 days embryonic stage and persist for approximately 1 week [15]. The three pre-segmental arteries (TA, OA and HA) regress when the posterior communicating artery develops, while the PA does not completely disappear, a segment of it being incorporated into V3 segment of the vertebral artery and part of the occipital artery [16]. However, some of them may persist after birth and into adult life: the TA is the most common one and represents about 85% of all persistent carotid-basilar anastomosis, the OA is by far the rarest one [17,18]. Exceptional observations of two different persistent anastomosis in the same patient have also been published: TA and OA, TA and HA [19,20].
Case Report
A new case of TA was found in the anatomy laboratory of the University of Quebec at Trois-Rivieres during a gross anatomy course intended for Montreal Medical Faculty otorhinolaryngologists (Figure 1). This artery was found during the dissection of a 72-year old woman who had died of amyotrophic lateral sclerosis, and had no other documented neurological medical history.
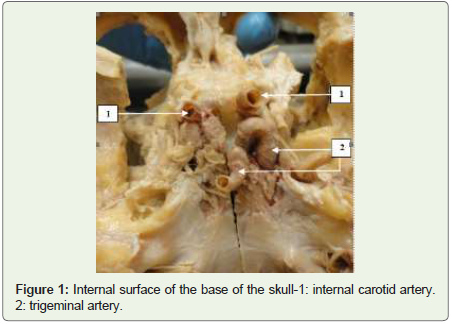
Figure 1: Internal surface of the base of the skull-1: internal carotid artery. 2: trigeminal artery.
The TA was 4 millimeters in diameter. It arised from the C4-C5 junction of the right Internal Carotid Artery (ICA), and joined the Basilar Artery (BA) between the Superior Cerebellar Artery (SCA) and the Anterior Inferior Cerebellar Artery (AICA). The caudal segment of the BA was hypoplastic. The TA supplied both SCA and the left Posterior Cerebral Artery (PCA). The first segment of the right PCA was absent; its distal segment was totally supplied by a thick right posterior communicating artery (PCoA). The left PCoA was present but hypoplastic (Figure 2).
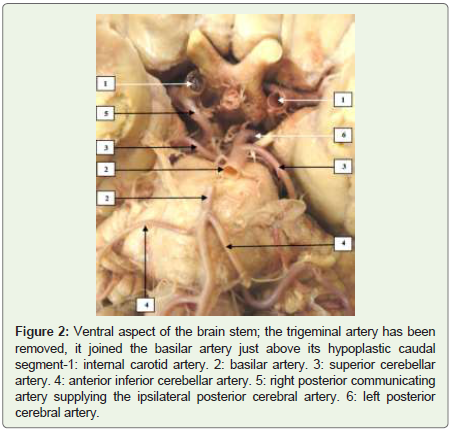
Figure 2: Ventral aspect of the brain stem; the trigeminal artery has been removed, it joined the basilar artery just above its hypoplastic caudal segment-1: internal carotid artery. 2: basilar artery. 3: superior cerebellar artery. 4: anterior inferior cerebellar artery. 5: right posterior communicating artery supplying the ipsilateral posterior cerebral artery. 6: left posterior cerebral artery.
Saltzman’s classification differentiates 3 types of TA [21]. Type I is characterized by the fact that all branches of the vertebrobasilar complex (both CSA and PCA) are injected via the TA, the ipsilateral PCoA being absent or hypoplastic. In Type II, the TA supplies both SCA, each PCoA supplying the ipsilatéral PCA. In Type III, one PCA is supplied by the ipsilateral PCoA, the other PCA and both SCA being injected by the TA. Our case report therefore belongs to Saltzman type III TA. Subtypes III a, b and c have been described when the TA supplies directly the SCA, AICA or PICA, respectively; unfortunately, the dissection of the specimen was too far ahead to make it possible to know which subtype it matches [22].
Epidemiological features of the persistent trigeminalartery
The reported prevalence of TA may vary, due to differences in the imaging modalities employed, from 0.1% to 0.63% [23,24]. It may be observed on either side, bilateral reports being exceptional [25]. Some studies could not find any statistical significant difference between male and female, though women were much more concerned than men in the 160 case reports we compiled (103 women / 57 men) [26].
Associated pathologies
We could find over 30 different pathologies related to or at least associated with a persistent TA in the medical literature. These pathologies are mainly of neurological (peripheral and central), tumoral, or vascular (other than cerebral) natures:
Peripheral nervous system: Cranial nerve symptomatology associated with a persistent TA may concern the optic nerve [amaurosis], the oculomotor nerve [palsy], the trigeminal nerve [trigeminal neuralgia], the abducens nerve [paresis], the cochleovestibular nerve [neurinoma; intermittent vertigo]. A recurrent Horner syndrome has also been found in association with a persistent TA [27-35].
Central nervous system: Ischaemic lesions, intracranial aneurisms, carotid-cavernous fistula [36-38].
Tumors: Intrasellar chordoma, pituitary adenoma [39,40].
Vascular anomalies (others than cerebral): Anatomical variant of the superior thyroid artery, aortic arch vessel anomalies [41,42].
Though amyotrophic lateral sclerosis is known to affect lower motor neurons in the brain stem, the association of a persistent TA and amyotrophic lateral sclerosis is in all likelihood to be regarded as coincidental: we could not find any publication pointing out a putative link between them [43]. However, we think it pertinent to publish a new case of persistent trigeminal artery discovered during a gross anatomy course.
References
- Quain R (1844) The anatomy of the arteries of the human body and its applications to pathology and operative surgery, with a series of lithographic drawings. Taylor and Walton, London.
- Sutton D (1950) Anomalous carotid basilar anastomosis. Br J Radiol 23: 617-619.
- Olry R, Haines DE (2004) Nomenclature of persistent carotid vertebrobasilar anastomosis. J Hist Neurosci 13: 190-192.
- Agnoli AL (1982) Vascular anomalies and subarachnoid haemorrhage associated with persisting embryonic vessels. Acta Neurochir (Wien) 60: 183-199.
- Alcalá-Cerra G, Tubbs RS, Niňo-Hernández LM (2012) Anatomical features and clinical relevance of a persistent trigeminal artery. Surg Neurol Int 3: 111.
- Kempe LG, Colonel MC, Smith DR (1969) Trigeminal neuralgia, facial spasm, intermedius and glossopharyngeal neuralgia with persistent carotid basilar anastomosis. J Neurosur 127: 445-451.
- Batujeff N (1889) A rare artery anomaly (origin of the basilar artery from the internal carotid artery). Anat Anz 4: 282-285.
- Gottschau M (1885) Two rare varieties of the stem of the aortic arch. Arch Anat Dev pp. 242-252.
- Lucarelli S, De Ferrari V (1960) Diagnostic studies of a case of abnormal origin (from the external carotid artery) of the left vertebral artery. Radiol Med (Torino) 46: 963-974.
- Pinstein ML, Gerald B (1976) Anomalous communication of the external carotid and vertebral arteries: Persistence of the proatlantal artery. Radiology 118: 626.
- Flynn RE (1968) External carotid origin of the dominant vertebral artery: Case report. J Neurosurg 29: 300-301.
- Chan PN, Yu SC, Boet R, Poon WS, Ahuja AT (1979) A rare congenital anastomosis between the vertebral artery and internal carotid artery. Am J Neuroradiol 24: 1885-1886.
- Padget DH (1948) The development of the cranial arteries in the human embryo. Contr Embryol 32: 205-261.
- Padget DH (1954) Designation of the embryonic intersegmental arteries in reference to the vertebral artery and subclavian stem. Anat Rec 119: 349-356.
- Luh GY, Dean BL, Tomsick TA, Wallace RC (1999) The persistent fetal carotid-vertebrobasilar anastomosis. AJR Am J Roentgenol 172: 1427-1432.
- Brismar J (1976) Persistent hypoglossal artery, diagnostic criteria: Report of a case. Acta Radiol Diagn (Stockh) 17: 160-166.
- Yilmaz E, Ilgit E, Taner D (1995) Primitive persistent carotid-basilar and carotid-vertebral anastomosis: A report of seven cases and a review of the literature. Clin Anat 8: 36-43.
- Bracard S (1983) Variations des artères cérébrales du normal au pathologique. Nancy, md thesis.
- Karazawa J, Kikuchi H, Furuse S, Sakaki T, Yoshida Y, et al. (1976) Bilateral persistent carotid basilar anastomosis. Am J Roentgenol 127: 1053-1056.
- Resche I (1979) The hypoglossal artery. Rennes, md thesis.
- Saltzman GF (1959) Patent primitive trigeminal artery studied by cerebral angiography. Acta Radiol 51: 329-336.
- McKenzie JD, Dean BL, Flom RA (1996) Trigeminal-cavernous fistula: Saltzman anatomy revisited. Am J Neuroradiol 17: 280-282.
- Allen JW, Alastra AJ, Nelson PK (2005) Proximal intracranial internal carotid artery branches: Prevalence and importance for balloon occlusion test. J Neurosurg 102: 45-52.
- O’Uchi E, O’Uchi T (2010) Persistent Primitive Trigeminal Arteries (PTA) and its variant (PTAV): Analysis of 103 cases detected in 16,415 cases of MRA over 3 years. Neuroradiology 52: 1111-1119..
- Son B, Yang S, Sung J, Lee S (2013) Bilateral persistent primitive trigeminal arteries associated with trigeminal neuralgia. Clin Neuroradiol 23: 45-49.
- George AE, Lin P, Morantz RA (1971) Intracranial aneurysm on a persistent primitive trigeminal artery: Case report. J Neurosurg 35: 601-604.
- Bronner A, Ruolt J, Vrousos C (1964) Persistent amaurosis and angiographic discovery of a trigeminal artery. Bull Ophtalmol Soc Fr 64: 951-954.
- Yin S, Zhang HT, Zhang DP, Zhang SL (2015) Persistent primitive trigeminal artery associated with monocular blindness and external carotid-vertebral artery anastomosis. Saudi Med J 36: 626-629.
- Bosco D, Consoli D, Lanza PL, Plastino M, Nicoletti F, et al. (2010) Complete oculomotor palsy caused by persistent trigeminal artery. Neurol Sci 31: 657-659.
- Jackson IJ, Mercado RG (1960) Persistent carotid-basilar artery anastomosis: occasionally a possible cause of tic douloureux. Angiology 11: 103-107.
- Park CK, Choi HJ, Lee SH, Rhee BA (2014) Trigeminal neuralgia caused by persistent primitive trigeminal artery. J Korean Neurosurg Soc 56: 278-280.
- Nakamagoe K, Mamada M, Shiigai M, Shimizu K, Koganezawa T, et al. (2012) Recurrent isolated abducens nerve paresis associated with persistent trigeminal artery variant. Intern Med 51: 2213-2216.
- Szdzuy D, Lehmann R, Feldmann H (1973) Rare association of primitive persistent trigeminal artery with acoustic neurinoma. 118: 98-100.
- Parthasarathy R, Derksen C, Saqqur M, Khan K (2016) Isolated intermittent vertigo: A presenting feature of persistent trigeminal artery. J Neurosci Rural Pract 7: 161-163.
- Rigamonti A, Lauria G, Prone V, Fumagalli C, Longoni M, et al. (2012) Recurrent horner syndrome and persistent trigeminal artery. Neurologist 18: 406-408.
- Uhlig S, Kurzepa J, Czekajska-Chehab E, Staśkiewicz G, Polar MK, et al. (2015) Persistent trigeminal artery as a rare cause of ischaemic lesion and migraine-like headache. Folia Morphol (Warsz) 74: 133-136.
- Benedek P, Uriarte AM (1966) Persistent trigeminal artery: A case associated with multiple bilateral aneurisms. Acta Neurol Latinoam 12: 61-65.
- Yoshida M, Ezura M, Mino M (2011) Carotid-cavernous fistula caused by rupture of persistent trigeminal artery trunk aneurysm: Case report. Neurol Med Chir (Tokyo) 51: 507-511.
- Navas M, Martinez P, Shakur SF, Barbosa A, Barcena E, et al. (2015) Intrasellar chordoma associated with a primitive persistent trigémial artery. Turk Neurosurg 25: 146-153.
- Machado MC, Kodaira S, Musolino NR (2014) Persistence of interstellar trigeminal artery and simultaneous pituitary adenoma: Description of two cases and their importance for the differential diagnosis of sellar lesions. Arq Bras Endocrinol Metabol 58: 661-665.
- Carella A, Lamberti P, Cavone L (1969) Persistent primitive trigeminal artery associated with superior thyroid artery anomaly. Acta Neurol (Napoli) 24: 814-819.
- Lotfi M, Nabavizadeh SA, Foroughi AA (2012) Aortic arch vessel anomalies associated with persistent trigeminal artery. Clin Imaging 36: 218-220.
- Kumar V, Abbas AK, Aster J (2013) Robbins basic pathology, (9thedn). Elsevier Saunders, Philadelphia, pp. 928.