Review Article
Current Evidence on Role of Zinc in Immune Function
Madan J1, Lingutla K2, Sreenivas V3, Mulye A4 amd Adhav C5
1Department of Food Nutrition & Dietetics, Sir Vithaldas Thackersey College of Home Science (Autonomous) SNDTWU, Juhu, Mumbai, India
2KL Health Centre, Hyderabad, India
3Department of Family Medicine Apollo Hospital, Jubilee Hills, Hyderabad & AFPI-Telangana, India
4Medical Advisor (Internal Medicine), Pfizer, India
5Medical Lead (Internal Medicine), Pfizer, India
*Corresponding author: Madan J, Department of Food Nutrition & Dietetics, Sir Vithaldas Thackersey College of Home Science
(Autonomous) SNDTWU, Juhu, Mumbai, India Phone: 022-26411375/26602504; E-mail: dr.jagmeetmadan@gmail.com
Article Information: Submission: 24/04/2022; Accepted: 27/06/2022; Published: 30/06/2022
Copyright: © 2022 Madan J, et al. This is an open access article distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Zinc is an important micronutrient and is listed as an essential trace element which is required to maintain the smooth functioning of the immune system.
Zinc has a vital role in ensuring normal development of innate immunity, neutrophils, and Natural Killer (NK) cells and warrants smooth functioning of the cells
modulating them. Zinc deficiency impacts the function of macrophages, T and B cells, and cytokine production. It acts as a second messenger in the immune
cells and participates in various signaling pathways including activation of T cells via T cell receptor and by the cytokine interleukin (IL)-2 pathway. Zinc is
required by the pathogens for survival, hence in case of an infection, host body limits the zinc in the milieu by altering zinc distribution. Zinc has also been
linked with antiviral properties against a wide variety of viruses, specifically RNA viruses such as rhinovirus, respiratory syncytial virus, and SARS-CoV. Zinc
is naturally available from a myriad of foods sources. However, it can be taken as supplements by people who are not able to meet the required daily amount
through food. Clinical studies have proven the health benefit of zinc supplements to address the deficiency as well as to ensure zinc-dependent physiological
functions run smoothly. In this review, the role of zinc in immunity and importance of zinc supplementation has been explored.
Keywords
Zinc; Immunity; Respiratory infection; Supplements; Nutrition; Micronutrient
Introduction
Immune system is an essential component of our physiology
which helps in combating infections along with internal and external
threats. Immune system works at three levels: physical barrier,
biochemical barrier, and immune cells. Physical barriers include
skin, mucous membrane, and body hair. They obstruct external
threats from entering the body. If the physical barrier is breached,
the biochemical barrier distinguishes between “self” and “non-self”
to eliminate the “non-self” using a plethora of immune cells (e.g.,
macrophages, natural killer cells, non-specific leukocytes, cytokines).
A more complex and adaptive response is generated by T and B
lymphocytes against the invasions. These cells produce target-specific
antibodies to neutralize the threat [1,2].
For the smooth functioning of this artillery, nutrition plays a
critical role. Macronutrients and micronutrients are needed to have
a healthy immune system and the protection it confers. Vitamins A,
B2, B6, B12, C, D, and E; folic acid; beta-carotene; zinc; selenium; and
iron are the required micronutrients to maintain the functioning of
the immune system [2,3].
Zinc plays a crucial role in innate and adaptive immunity. Zinc
deficiency manifests as thymic atrophy, lymphocyte count ≤ 1100
cells/μL, impaired immune response and mortality [4]. The estimated
global zinc deficiency is between 17% to 20% [5]. The deficiency is
more prominent in developing countries of Africa and Asia. It occurs mostly in the elderly, pregnant women, children from developing
nations, vegans/vegetarians, and people suffering from chronic
diseases (e.g., liver cirrhosis, inflammatory bowel disease) [6-8]. Even
marginal or moderate deficiency of zinc can cause delay in wound
healing, cause inflammation, and increase oxidative stress [9,10].
In this review, the role of zinc in immunity and importance of zinc
supplementation has been explored.
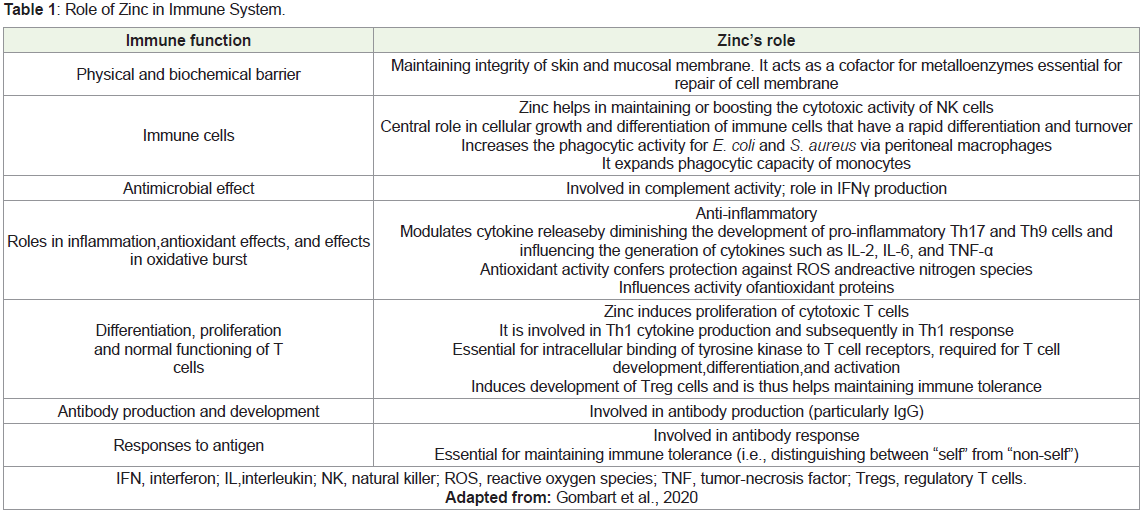
Role of Zinc in Immunity:
Zinc plays a critical role to ensure normal development of innate
immunity, neutrophils, and NK cells and warrants smooth functioning
of the cells modulating them. Macrophages are also impacted due to
zinc deficiency. Functions like phagocytosis, intracellular killing, and
cytokine production are impacted by zinc deficiency. The maturation
and working of T and B cells are adversely affected due to insufficient
zinc. Zinc has antioxidant properties and helps stabilize membranes
thus preventing injury induced by free radicals [11].Zinc acts as a second messenger in the immune cells [12]. Zinc
participates in various signaling pathways including activation of T
cells via T cell receptor and by the cytokine interleukin (IL)-2 pathway
which is the major stimulus for T cell proliferation once activated [13-15]. Immune cells recognize the zinc deficiency before it is identified
in the plasma [16]. The increased susceptibility to infections due
to zinc deficiency is probably caused by zinc dependent alterations
in chemotaxis, phagocytosis, respiratory burst and formation of
neutrophil extracellular traps by innate immune cells [17-19].
The systemic and intracellular zinchomeostasis is strictly
regulated to keep the free zinc ions (Zn2+) at a minimal fraction
of about 0.0001% of total cellular zinc. Majority of zinc is bound
to proteins such as serum albumin or intracellular metallothionein
proteins. This helps in transfer of bound zinc to zinc-binding
enzymes and transcription factors on need basis. Zinc transport is
primarily facilitated by 2 groups of proteins: the ZnT [solute-linked
carrier 30 (SLC30A)] family, which is responsible for efflux of zinc
outside the cell or influx into organelles, and the ZIP [Zrt- and Irtlike
proteins (SLC39A)] family of proteins, which performs the
opposite role, transporting zinc into the cytoplasm from extracellular
sources or cellular organelles. There are more than 30 human proteins
accountable for zinchomeostasis. They collectively warrant that zinc
does not become toxic (in the case of dietary excess), nor limited (in
the case of dietary insufficiency). This balance when not maintained
may result in zinc-induced copper deficiency if zinc intake is in excess
and severe zinc deficiency if there is dietary insufficiency [7]. Zinc and
copper are absorbed via the small intestine. Presence of excess zinc
stimulates production of metallothionein, a copper and zinc-binding
ligand, in enterocytes. These metallothionein proteins are further
stimulated by the zinc to provide more zinc-binding sites in order
to prevent zinc toxicity. Metallothionein proteins have high affinity
for copper as compared to zinc, and increased metallothionein
concentration in enterocytes leads to its preferential binding with
copper. This hampers the absorption of copper into the systematic
circulation, as the copper remains tethered inside the enterocytes,
the metallothionein-copper complex is excreted via the feces, thus
resulting in copper deficiency [20,21]. Zinc absorption is affected by
physiological, disease and dietary factors [4,22,23]. Dietary factors affecting zinc absorption include quantity of zinc intake, protein
quality and quantity (positive correlation), phytate & fiber (negative
correlation), calcium (negative correlation), iron (possible negative
correlation), toxic cadmium levels (negative correlation), lowmolecular
weight ligands and chelators (positive correlation), amino
acids (positive correlation), and organic acids (possible positive
correlation) [22,23]. The physiological state of the mucus layer and
intestinal fluid determines the extent of zinc absorption, since they
are not static. Additionally, albumin concentration is also reported
to have a positive correlation with zinc absorption [23]. Zinc can be
used as therapeutic treatment in diseases like chronic gastrointestinal
disorders,renal diseases, and genetic predispositions, such as sickle
cell anemia and the zinc malabsorption syndrome [4] Table 1.
Zinc in Diarrhea:
Zinc causes a direct pro-absorptive effect on transepithelial
ion transport by inducing ion absorption in enterocytes in basal
conditions. Zinc also plays a role in maintaining gastrointestinal
epithelial membrane barrier function. It stimulates enterocyte growth
and differentiation, reduced intestinal permeability and keeps a check
on oxidative stress and inflammation [24], Based on the clinical
studies, WHO has recommended zinc supplement for managing
acute diarrhea as an adjunct to oral rehydration salts (ORS) [25].Zinc in Infectious diseases:
Zinc is essential for the host as well as the invading pathogen.
A competition ensues for securing zinc which the pathogen requires
for survival, multiplication and thus causing the disease. As a defense
mechanism, the host’s body tries limiting zinc in the milieu of the
pathogen by altering the zinc distribution. One of the ways of
achieving this is locking 99.9% of zinc within the cells of the host,
thus locking out the pathogen from gaining direct access. Secretion
of inflammatory cytokines like IL-6 up regulates ZIP14 expression
within hepatocytes leading to zinc getting accumulated in the liver
bound to metallothionein. Zinc concentrations can be altered on
an extracellular level by releasing some antimicrobial peptides
from the S100 family. Macrophages kill phagocytose pathogens like
Histoplasma capsulatum by depriving it of zinc by reducing the
phagosome zinc content. They kill tuberculosis (which is caused by
Mycobacterium) with intoxication of excess amounts of zinc and
copper.Metallothioneins, the small protein molecules responsible for
storage and transfer of zinc, play a role in heavy metal detoxification,
immune response, apoptosis, oxidative stress, and are classified as
interferon stimulated genes (ISGs). Metallothionein inductions occur
as a response to interferons (IFNs). IFNs stimulate an influx of zinc
into the target cell which in turn promotes metallothionein expression.
In vitro and in vivo studies have proved that metallothioneins are
induced by viruses which are subsequently ascribed to zinc influx
or redistribution. Metallothionein upregulation has been noted as a
retort to various viruses like measles, influenza, HIV, hepatitis C, and
coxsackie virus, among others [7]. Zinc has been studied in various
clinical trials. A particularly positive association of zinc supplements
and respiratory infections has been observed. Zinc deficiency has
been associated with pneumonia in pediatric patients. Early symptom
resolution and prevention of respiratory infections was reported
when zinc supplements were taken by the patients [8].
Zinc has been linked with antiviral properties via direct and
indirect mechanisms against a wide variety of viruses, specifically
RNA viruses such as rhinovirus, respiratory syncytial virus, and
SARS-CoV [27]. Zinc can exhibit its antiviral properties by: inhibiting
fusion of virus with the membrane of the host cell, blocking release
of viral particle, disrupt the virus’ protein translation and processing,
destabilize the viral envelope, and hamper the polymerase function
of the virus [27-29]. Zinc is hypothesized to preserve the cellular membrane by blocking the virus’ entry. Zinc regulates proteins of
tight junction structure of the mucosal layer, thus exhibiting antiviral
immunity and preserving the mucosal membrane integrity. Zinc
disrupts the viral replication pathway by altering the proteolytic
processing of RNA-dependent RNA polymerase (RdRp) and replicase
polyproteins. Hence, it is being implied that zinc might alter the RNA
synthesis of COVID-19 [27].
Zinc has been seen in a favorable light against SARS-CoV-2 (COVID-19) virus. The virus is dependent on the metabolism of the
host cells to exhibit its viral properties. In vitro studies have shown
that zinc cations inhibit SARS-CoV RNA polymerase with assistance
from zinc ionophore pyrithione, thus suggesting an antiviral property
against the virus. It is also indicated that zinc ions decrease the
angiotensin-converting enzyme 2 (ACE2) which is required by the
virus to enter the host cells [28,29].
Zinc possesses anti-inflammatory properties and helps balance
the immune response through an infectious disease. COVID-19
throws the immune system out of harmony induced by hyperinflammation
due to production of pro inflammatory cytokines such
as IL-6, C - reactive protein (CRP), TNF-α, and IL-1β. The cytokines
thus produced (IL-6, C - reactive protein (CRP), TNF-α, and IL-
1β) cause the cytokine storm. Cytokines, Reactive Oxygen Species
(ROS), and nitrogen species recruit a large number of activated
immune cells. These together cause the destruction of the lung tissue
which may permanently damage the lungs and can prove fatal. If
the anti-inflammatory response falls short of expectation, systemic
inflammation, and organ failure are anticipated [29]. Although, it
cannot be conclusively suggested in zinc’s favor, it is recommended
to initiate supplements containing zinc, vitamin D, and selenium to
restore deficiencies in case of COVID-19 infection [30].
Zinc deficiency is widely prevalent, especially in the elderly.
As establishing zinc is challenging, supplements can prove to be a
beneficial approach to address the deficiency and ultimately reduce
the global burden of COVID-19 [31]. Zinc supplements have not
been associated with any serious life-threatening adverse reactions or
deaths. Since zinc-related toxicity has been reported, opinion from
healthcare professionals should be sought before such supplements
are taken. From COVID-19 perspective, standardized doses for
prevention and therapeutic purpose should be established and
advised since zinc supplements are sold as over-the-counter products
[32].
Role of Zinc in Respiratory Infections
Various studies have shown that zinc and some zinc-dependent
proteins aid in anti-viral defense and immune regulation in the
respiratory tract. Zinc has been proposed to reduce the viral titer
following influenza infection, decrease respiratory syncytial virus
(RSV) burden in the lungs, reduce duration of viral pneumonia
symptoms, and prevent acute respiratory distress syndrome (ARDS)
and ventilator-induced lung damage. Zinc deficiency can cause
substantial changes in the epithelial layer of the lungs, possibly
through up-regulation of IFNγ and TNFα, enhancement of FasR
signaling, and enhancement of apoptosis [33].
Beneficial effects of zinc supplementation in respiratory infections
are supported by the results of many reports 34,35].
Dietary Zinc and Supplements
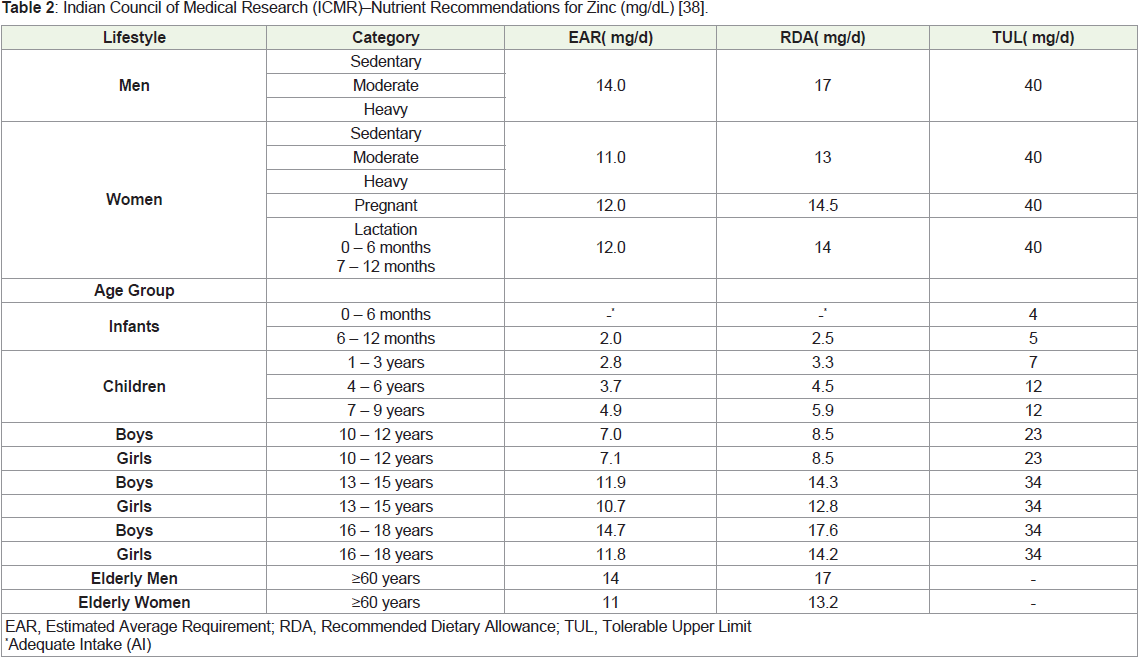
Zinc is listed as an essential trace element [36]. The recommended
dietary allowances (RDAs) for zinc for age 0-6 months for both males
and females is 2 mg. For children between 7-12 months and 1-3
years, 3 mg is recommended for both genders. For ages 4-8 years and
9-13 years, 5 mg and 8 mg are recommended, respectively. For male population above and equal to14 years, 11 mg is the recommended
RDA. In females aged 14-18 years, 9 mg and for females above 19
years, 8 mg are recommended RDA. Pregnant women between 14-
18 years need 12 mg and for pregnant women above and equal to 19
years of age 11 mg is the recommended RDA. For lactating women,
13 mg is recommended for women between 14-18 years and 12 mg
for women above and equal to19 years of age [37] Table 2.
Zinc is naturally available from a myriad of foods sources. The
highest zinc content is present in shellfish (74 mg per serving). The
second highest source is red meat. Zinc bioavailability is relatively
high in animal sources. The reason for such vast difference is absence
of phytic acid which inhibits absorption of zinc and the presence
of certain amino acids that enhance absorption. Vegetarian food
sources include beans, nuts, and whole grain products [36,37]. The
Dietary Guidelines for Americans recommend inclusion of zinc rich
food items in the diet of infants starting at about 6 months especially
in infants fed human milk [39].
Elderly individuals (above ≥ 65 years of age), children and
adolescents, pregnant and lactating women, vegetarians, alcoholics,
and infants born premature or having low birth weight are at a risk of
developing zinc deficiencies. Diseases or disorders increasing risk of
zinc deficiency include malnourishment, persistent or severe diarrhea,
malabsorption syndromes, inflammatory bowel disease (e.g., Crohn’s
disease,ulcerative colitis), Chronic kidney disease, Sickle cell anemia,
and patients who have undergone gastric by-pass surgery [36], Zinc
deficiency is often discovered after infants are weaned off breast milk,
and can be due to acrodermatitis enteropathica, a rare, autosomal
recessive inherited disorder of zinc metabolism, or an acquired
deficiency. These infants present with diarrhea, failure to thrive, and
skin lesions as a result of impaired gastrointestinal zinc uptake and
can be corrected using oral supplements [40].
Zinc supplements are available in various pharmaceutical
formulations like tablets, capsules, and lozenges. The supplements
contain zinc salts in the form of gluconate, sulfate, and acetate [37].
Zinc supplementation in children is associated with reduction in
all-cause childhood mortality. Zinc supplements reduce incidence
of diarrhea and the associated morbidity [41,42]. Fortification with
zinc can be an effective strategy to rectify deficiencies in at-risk
populations but the evidence is insufficient. Zinc supplementation
has been proven to meet the dietary requirements in vulnerable
groups of infants, children, adolescents, and pregnant women [41].
Clinical studies have concluded that giving zinc supplements as a
preventive measure in at-risk populations increases children’s weight
gain and promotes linear growth [5]. Medical dosage of zinc i.e. >40
mg/d of elemental zinc may be useful for managing the nutritional
status and supporting optimal levels of zinc. The medical dose of zinc
has been proven to be safe, but the posology may vary depending on
specific physiopathology. High zinc intake for longer duration may
inhibit its absorption. Zinc supplements can help with various clinical
situations like infections, liver diseases, and disorders of the central
nervous system, cancers, and heart diseases [43].
Zinc is known to play a pivotal role in metabolic syndrome
development, inflammation suppression, scavenging free radicals,
modulating insulin, regulating cytokines, lipid metabolism, confirmed via various clinical studies. Zinc supplements have been
proven to help in regulating blood pressure, blood glucose, serum
cholesterol, and low-density lipoproteins (LDL) [44].
Clinical Evidence:
Numerous clinical studies have explored the effects of zinc
supplementation in various age groups for its role in infections and as
a general nutrient supplement.Zinc sulphate monohydrate at a dose of 3 mg/kg given twice a
day for 10 days orally along with standard antibiotics to neonates in
intensive care units with clinical symptoms of sepsis, significantly
reduced the mortality rate as compared to the group that did not receive
the supplement. The study was conducted at Jawaharlal Institute of
Postgraduate Medical Education & Research, Pondicherry, India in
between from September 2013 to December 2016 on 203 neonates
[45]. In another single-arm, open-label, study on pediatric population
(aged 6 months to 5 years), 465 healthy children with and without
zinc deficiency were given zinc syrup 5 ml (containing 20 mg zinc
sulfate) once daily, for 14 days. Zinc supplementation was associated
with a 48% reduction in the acute upper respiratory infection (AURI)
episodes and 68% reduction in the acute lower respiratory infection
(ALRI) episodes in the zinc deficient children [46].
In a community based, double-blind randomized controlled
trial, efficacy of high zinc biofortified wheat flour was evaluated in
children (aged 4-6 years) and non-pregnant, non-lactating woman of
child-bearing age (WCBA) against low zinc biofortified wheat flour,
in Delhi, India. The mean zinc levels did not differ between the two
groups. However, beneficial effect of the high biofortification was
observed in self-reported morbidity indicators such as a reduction in
days with pneumonia and vomiting, days with fever, days with ear
discharge in both children and WCBA [47].
In a placebo-controlled study on 53 elderly patients with zinc
deficiency, zinc supplements (30 mg/day for 3 months) were evaluated.
The group receiving the supplements achieved a significant increase
(16%) in serum zinc levels. However, participants with zinc
serum levels of ≥60 mg/dL did not notice a further climb to ≥70 mg/
dL. A significant increase in anti-CD3/CD28, phytohemagglutinin stimulated
T cell proliferation and peripheral T cells were also
reported with the supplement [48].
Conclusion
Zinc is an essential trace element and plays a vital role in
ensuring optimal functioning of the immune system. Zinc deficiency
is associated with increased risk of infections and inflammation,
especially in at-risk population. Zinc supplements provide medical
dosage of zinc to meet the RDA which may prove particularly
useful in vegetarians and in populations at a risk of developing
zinc deficiency. Zinc supplements have a certain health benefit to
address the deficiency and thus ensure zinc-dependent physiological
functions run smoothly. However, the interactions between the
micronutrients may hamper the overall benefits of the supplements.
Excess quantities consumed via zinc supplements may lead to toxicity
and copper deficiency. Recent studies in COVID-19 have teased a
beneficial role of zinc in preventing and fighting the infection. It is hence vital to meet the daily dietary requirement of zinc which can be
achieved by zinc supplements. Further studies may be warranted to
establish standardized doses for prevention and therapeutic purpose.
Acknowledgement
The authors would like to acknowledge Ms. Vaidehi Wadhwa
(Medical Excellence, Pfizer Ltd.) for medical writing support for
preparing this manuscript.
References
Citation
Madan J, Lingutla K, Sreenivas V, Mulye A, Adhav C. Current Evidence on Role of Zinc in Immune Function. Indian J Nutri. 2022;9(3): 262.