Research Article
Effect of Virgin Coconut Oil on Lipid Profile and Other CVD Risk Factors
Vijaya Kumar M1*, Vasudevan DM2, Sundaram KR3, Krishnan S2, Chandrasekhar R1, Mathew N1 and Nandakumar S1
1Department of Cardiology, Amrita Institute of Medical Sciences and Research Centre, Kochi, Kerala, India
2Department of Bio chemistry, Amrita Institute of Medical Sciences and Research Centre, Kochi, Kerala, India
3Department of Biostatistics, Amrita Institute of Medical Sciences and Research Centre, Kochi, Kerala, India
*Corresponding author: Vijaya Kumar M, Department of Cardiology, Amrita Institute of Medical Sciences and Research Centre,
Kochi, Kerala, India; Phone: +91 9446301348, 0484 2851555, Fax: +91 484 2802020; E-mail: vijaymaniyal@gmail.com, drmvijay@
aims.amrita.edu
Article Information: Submission: 08/04/2022; Accepted: 13/06/2022; Published: 17/06/2022
Copyright: © 2022 Vijaya Kumar M, et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background & objectives: Effect of coconut oil on lipid profile and atherosclerosis is controversial. Saturated fat appears to have favourable effect on
high density lipoproteins (HDL). There are no long-term studies on Virgin coconut oil (VCO) used for human consumption. This study was intended to evaluate
its effect on lipids.
Methods & study design: In a single centre non-randomized study subjects with coronary artery diseases (CAD) (group 1) and without proven CAD
(group 2) were assigned to receive VCO for 6 months. They were followed up with lipid profile, ApoB/ApoA ratio, antioxidants, high sensitive C-reactive protein
(CRP) and Glycosylated haemoglobin (HbA1c) at regular intervals
Results: 42 subjects in group 1 and 32 in group 2 completed 6 months study. There was significant increase in total cholesterol in group 1 (p = 0.033).
There were no changes (Group 1 and group 2 respectively) in low density lipoproteins (LDL) (p = 0.12 and 0.21), Apo B/A ratio (p = 0.47 and 0.97), total
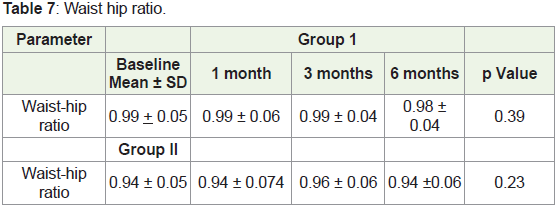
antioxidants (p= 0.24 and 0.57), waist hip ratio (p= 0.39 and 0.229) and hs CRP (p = 0.25 and 0.011) in either group. There was statistically significant increase
in HDL (p = 0.011 and 0.025) levels in both groups.
Conclusion: VCO does not change lipid profile in an atherogenic direction. VCO increases HDL cholesterol without changes in LDL, Apo B/A ratio, redox
potential, inflammatory markers, central obesity and HbA1C. There is an increase in total cholesterol in those with CAD.
Keywords
Virgin coconut oil; Lipids; Atherogenic; Anthropometry; Antioxidants
Introduction
Increased risk of cardiovascular disease has been attributed to
consumption of saturated fatty acid rich food among many other
reasons [1]. There are many guidelines recommending reduction of
SFA for cardiovascular disease prevention [2-5]. Coconut oil and its
effect on the composition of lipids in human is still under debate.
Coronary artery diseases incidence is very high among population
of Kerala state due to many known and unknown reasons [6].
We, in an attempt to understand the biochemical role of this most
commonly used oil media in this part of the country, conducted
many studies including one randomized study [7-10]. Fatty acid constitution of coconut oil also is debatable, some of the researchers
feels that the major fatty acid lauric acid can be no more classified
as medium chain fatty acid [11,12]. While others are of different
opinion, Even though these are debatable facts 2017American Heart
Association Presidential advisory on dietary fats and cardiovascular
disease recommends to limit coconut oil with LDL rising property
in order to prevent cardiovascular diseases [13]. Fatty acid content
in virgin coconut oil (VCO) is essentially the same as in regular oil
but additionally there are phytochemicals and the exact role of these
ingredients in metabolism is not known. However, the changes in
the chemical composition during the bleaching and deodorization of the conventional oil are not seen in virgin coconut oil. There are
many short-term studies with VCO claiming the beneficial effect and
consuming about 30 ml of VCO daily has been reported to have HDL
enhancing capability [14-16]. In the context of people consuming
the VCO for its beneficial effect, we conducted a long-term study to
evaluate its metabolic effect on lipids.
Material & Methods
Approval from scientific committee and institutional ethics
committee was obtained as per guidelines. All subjects signed
informed consent before entering the study.
Clinical Trials Registry of India CTRI/2015/04/005678.
Setting:
Participants were identified from those attending Cardiology
outpatient department as well as from the community.Design:
Non -randomized open label studySample size:
Since it is a pilot study, we recruited 50 subjects in each groupParticipants:
Group I had proven CAD on medication including statins. CAD
was diagnosed by either one of the following. ECG changes consistent
with old myocardial infarction, echocardiogram with regional wall
motion abnormality, coronary angiogram, myocardial perfusion
scan, multi detector CT angiography) on medication including
statins. Group II included subjects without known CAD and not on
cholesterol reducing medications. Both groups were with low HDL
cholesterol (<40 mg /Decilitre in men and less than 50 mg/Decilitre
in female). Patients with uncontrolled hypothyroidism, renal failure
creatinine >2 mg/dl and liver failure, and other illness limiting the life
expectancy <1 year were excluded.Intervention:
On the day of recruitment after signing the informed consent
and initial assessment they were allocated 4 grams of VCO for daily
consumption. They were called at specific time periods for blood test,
anthropometry and for dispensing VCO capsules.Main outcome measures:
The primary outcome was change in serum lipid profile especially
the HDL level, ApoB/Apo A ratio, antioxidant levels and C reactive
protein. The secondary objectives were the change in anthropometric
measures and glycosylated haemoglobin.VCO product used in this study:
The VCO capsules used in this study were manufactured as per
norms and have been certified by food safety and standards authority
of India and registered under worldwide quality assurance.Subject compliance:
Each subject was interviewed by the dietician at the beginning of
the study and a diary was provided to them to note down the capsule consumption. The balance capsules were returned during each visit
and tallied with consumption.Anthropometric measurements:
Body mass index: Height was measured with subjects on bare foot
using standardized extendable measuring rod. Weight was measured
with an electronic Dura weighing machine on empty stomach.Waist hip ratio: Waist circumference was measured with the
patient standing, at the end of expiration midway between the twelfth
rib and anterior superior iliac spine as per WHO STEPS protocol. The
hip measurement was taken at the level of greater trochanter and the
ratio was calculated.
Biochemical parameters:
Lipid profile was estimated after 12 hours fasting as per institution
protocol in Roche COBAS-8000. Apo lipoprotein B, Apo lipoprotein
A, and ultrasensitive C reactive protein were estimated by immunoturbidometry
in Roche COBAS-8000 Glycosylated haemoglobin
was measured by HPLC in Bio rad- Variant. Four clinically
relevant antioxidants catalase (CAT), Glutathione peroxidase (GP)
Glutathione redutcase (GR) and total anti-oxidant status were
estimated. Catalase was estimated by CELLBIOLABS ,INC ELISA
KIT manually. Total antioxidant status (TA), Glutathione reductase
and Glutathione peroxidase were estimated by photometric method
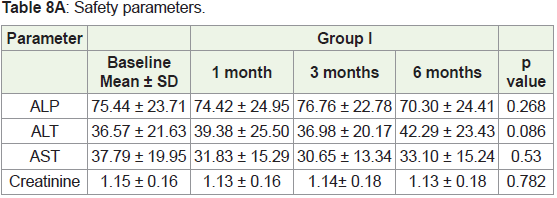
using RANDOX kit in. in Roche COBAS-8000Safety outcome measured:
Both renal (serum creatinine) and liver functions (aspartate
aminotransferase (AST), alanine aminotransferase (ALT) and
alkaline phosphatase) were estimated at one month, three month and
at end of the studyStatistical analysis:
Statistical Analysis was done using IBM SPSS statistics 20
windows (SPSS Inc., Chicago, USA). For all the continuous variables
the results are given in mean ± standard deviation and for categorical
variables as percentage.To compare the mean of numerical variable between cases and
control two sample t- test was applied for parameter test. To test
the statistical significance of association of categorical variables chi
square test was applied.
Probability value (p value) less than 0.05 is considered for
statistical significance. To study the statistical significance of
difference in mean value of continuous variables from the baseline to
different time periods Repeated Measure of ANOVA is used.
Results
We included 50 subjects with known CAD status on medication
(Group I) and 39 non-CAD subjects (Group II) in to the study over a
period of 2 years. Out of these 43 subjects in group I and 32 in group
II completed the study. The baseline characteristics are shown in Table 1.
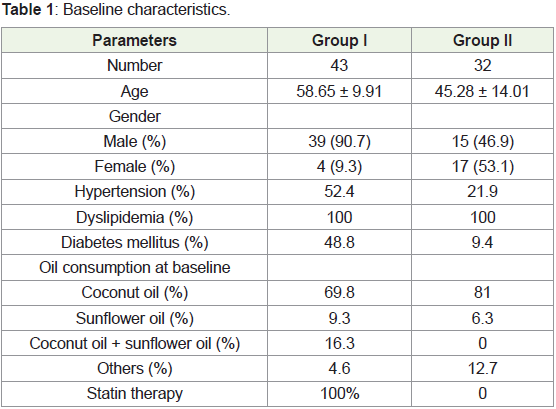
The number of male participants were high in group I and the
second group participants were younger than group one. Both groups
had low HDL cholesterol. CAD group subjects were on cholesterol reducing statins. Risk factors were high in group I compared to group
II (Table 1). Both groups were consuming the oil of their choice at
the time of recruitment and thereafter. Significant number of subjects
was taking coconut oil at baseline.
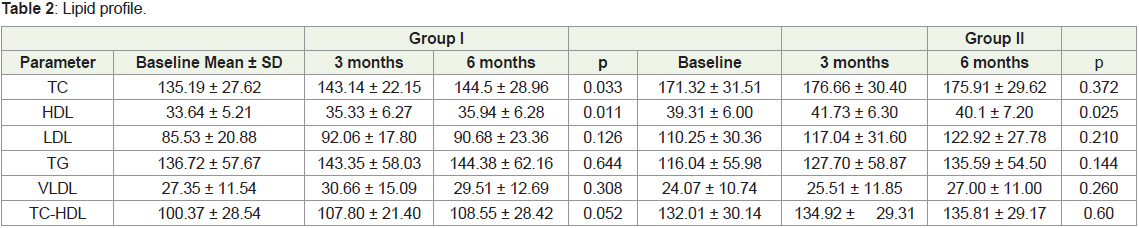
The total cholesterol levels showed steady increase in group I at
the same time there was no change in group II. HDL cholesterol shows
statistically significant increase in both groups. The LDL cholesterol
in group I subjects, who were consuming the statins was significantly
lower compared to non-CAD group (Table 2). LDL Cholesterol was
not significantly elevated in either group during the study period. No
statistically significant changes occurred in triglycerides and VLDL
level.
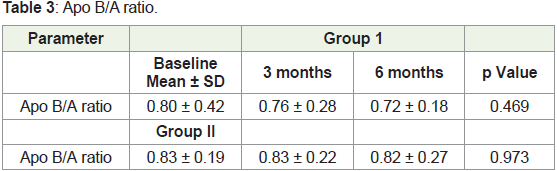
The best indicator of non-atherogenic versus atherogenic lipids,
the ApoB/A ratio did not change during the study (Table 3).
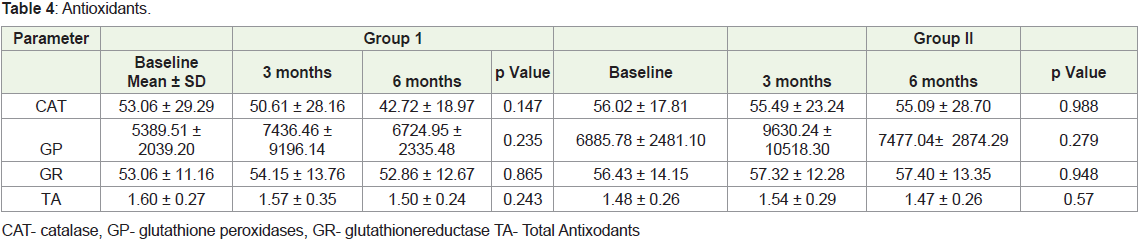
In both groups the main anti-oxidants did not show statically
significant changes (Table 4).
Ultra-sensitive CRP did not show statistically significant changes
in group I but the high USCRP in group II declined toward the end
of the study (Table 5).

Glycosylated haemoglobin levels were little high in CAD group
as result of their diabetic status but there were no changes during the
study period (Table 6).

The consumption of VCO over 6 months did not show any
changes in the anthropometric measurements (Table 7).
There were no changes in the liver function and renal function at
different stages of the study (Table 8).
Discussion
Virgin coconut oil extracted directly from the coconut milk
which varies significantly from traditional coconut oil with respect
to the various phytochemicals and Vitamin E content. Large number
of populations started using VCO as food supplement and in this
context, we studied the metabolic effect this oil.
Pre-screening for this study has shown that 65% CAD patients
uses coconut oil for their dietary purpose and still higher numbers in
group II. In both arms subjects with low HDL was recruited to see the
effect of VCO on low HDL.
There are no previous long-term studies to understand the dose
of VCO capable of making metabolic effect and a short-term study
done in the past used 15 grams twice daily for 8 weeks [17]. The dose
of 4 grams/day of VCO and the capsule form are selected mainly
for long term convenience of the subject. Four grams/day of VCO
constitutes about 720 grams of oil over 6-month time equivalent to
6500Kcal which is sufficient to produce metabolic effects.
The groups were significantly different in many aspects regarding
the risk factors, diseases and the drugs they are consuming. Group I
had higher incidents of risk factors (50% hypertension, 48% diabetes
and 100% dyslipidaemia) compared to group II. In group I all the
subjects were on different class of statins in spite of achieving desired
level for their secondary prevention.
The lipid profile at baseline shows significantly less total
cholesterol and LDL in group I because of their statin therapy. The
total cholesterol in group I was significantly elevated at the end of
6 months but not in group II. The non -HDL cholesterol, which
represents the cholesterol content present in all the atherogenic
lipoproteins and was used in Helsinki study [18]. Elevated levels of
non-HDL-C in combination with normal levels of LDL-C identify
a subset of patients with elevated levels of LDL particle number,
elevated apo B concentrations, and LDL of small, dense morphology
[19]. In our study the non-HDL cholesterol didn’t show significant
changes. In group II the non-HDL cholesterol even though high
compared to group I didn’t change significantly at the end of the
study indicating that VCO is not altering the lipids in atherogenic
direction in the dose used.
ApoB/A ratio, the best reflector of the atherogenic lipids in the
blood and the cut-off values for the apoB/apoA-I ratio that define a
high cardiovascular risk were proposed to be 0.9 for men and 0.8 for
women [20,21]. Elevated LDL Cholesterol and non -HDL cholesterol
does not indicate the so called particle size which is more important
for the genesis of atherosclerosis and can be better indicated by Apo
B levels The MESA study showed that discordantly elevated Apo B is
associated with coronary calcification [22]. The ratio of this remains unaltered in both groups at the end of the study and is in accepted
level for cardiovascular risk.
Diseases like atherosclerosis results from the damage of cell
membrane and nucleic acid by these ROS (Reactive oxygen species)
molecules. There are many data to support this redox potential
involvement in CAD [23,24].
The metabolic effect of the major median chain fatty acid like
lauric acid in coconut oil on redox potential is not clear. Unsaturated
fatty acids in oils like sunflower oil is likely to increase the oxidative
stress compared to coconut oil [7]. Our study also shows that there is
no change in oxidation related parameters on long term consumption
of virgin coconut oil, even in group I with elevated total and LDL
cholesterol probably indicating that the lauric acid rich coconut oil
is not susceptible for oxidation. The anti-oxidants in both groups
remain unchanged during the study period indicating that the VCO
use during 6-month time does not alter the redox balance.
Ultra-sensitive CRP is a marker of inflammation in the body
and is very much correlated with the atherogenic CAD. There were
few reports stating that the VCO is an anti-inflammatory property.
In our study there was no significant change in this very important
biomarker at the end of the study in those with CAD but shows
reduction in group II. The major concern about the oil was the safety
on prolonged use and it has been shown that there was no hepatic or
renal function alteration during 6-month period.
Limitation
Small study and confounding factors were not considered in
analysis.
Conclusion
Considering the overall effects of VCO on lipoprotein profile
it seems that it does not change the profile in atherogenic direction even though there is an increase in total cholesterol in subjects with
CAD but not in others. Long term use of VCO in our subjects did
not show change in redox potential, inflammatory markers, central
obesity and glycosylated haemoglobin.
References
Citation
Vijaya Kumar M, Vasudevan DM, Sundaram KR, Krishnan S, Chandrasekhar R, et al. Effect of Virgin Coconut Oil on Lipid Profile and Other
CVD Risk Factors. Indian J Nutri. 2022;9(3): 260.