Case Report
Diet Analysis and Counseling for Caries Prevention: A Case Report
Amra S* and Pushpanjali K
Department of Public Health Dentistry, Faculty of Dental Sciences, MS Ramaiah University of Applied Sciences, Bengaluru-560054,
India
*Corresponding author: Amra S, Department of Public Health Dentistry, Faculty of Dental Sciences, MS Ramaiah University of
Applied Sciences, Bengaluru-560054, India; Phone: +91 9731723236; E-mail: dramra.sultana@gmail.com
Article Information: Submission: 28/04/2022; Accepted: 03/06/2022; Published: 08/06/2022
Copyright: © 2022 Amra S, et al. This is an open access article distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Dental caries is a diet-related disease that continues to be a problem for certain dental patients. Frequent consumption of fermentable carbohydrates
that have low oral clearance rates increases the risk for caries. This report emphasises on the significance of diet counseling in prevention of dental caries.
A 21-year-old female patient reported to the clinic with a chief complaint of brownish discoloration on the posterior region. On eliciting detailed case
history it was found that patient had adequate oral hygiene practices, however, the patient had a habit of snacking and not rinsing her teeth immediately
afterward. Detailed dietary analysis revealed on patients habit of ‘in-between’ consumption of sugary foods. Hence the intervention was aimed at reduction of
in-between consumption and replacement with alternate diet. Multiple oral health education sessions, positive reinforcement and allowing the patient to decide
the alternate by explaining her food pyramid followed by convincing the patient to change her pattern of diet were the measures taken. All these measures
resulted in changing the eating habit of the patient.
Hence it is important to understand the risk of patient to develop dental caries and to plan tailor made interventions for a caries preventive regimen.
Keywords
Dental caries; Diet; Diet counseling; Diet chart; Sugars; Cariogram
Introduction
Many chronic health problems are associated with increased
consumption of free sugars. The term free sugars refers to
monosaccharides and disaccharides that are naturally present in
honey, syrups, and fruit juices, as well as also added by manufacturers
or consumers to food and beverage [1]. According to the WHO, free
sugars should make up less than 5% of one’s daily total energy intake,
to reduce one’s risk of obesity and dental decay. This recommendation
is based on the recognition that dental caries has cumulative health
effects, affecting both children and adults. Even a small reduction in
the risk of dental caries in childhood is significant in later life since
dental caries is the consequence of lifelong exposure to a dietary risk
factor [2].
Despite dental caries is highly preventable disease, but increased
intake of free sugars considers as major risk factors for chronic disease
among population [3]. Age wise prevalence was 62% in patients above 18 years and 52% among 3-18 years of age in India [4]. Dental caries
occur when bacteria metabolize sugar, which produces organic acids,
leading to the demineralization of the hard tooth structure [5]. Dental
caries is a multifactorial disease and one of its factors is behaviour
related diet. With this background, it seems logical that dental
practitioners should conduct risk assessment based on the primary
findings. This will enable planning interventions specific to risk
identification ranging from diet counselling to complex treatment.
Case Report
A 21-year-old female patient reported to the Comprehensive Oral
Health Care Unit with a chief complaint of brownish discoloration on
posterior region since 1 year with no history of pain and sensitivity
and any other related signs. Patient had past dental history of
restorations and oral prophylaxis which was done 1 year ago. The
patient confirmed adequate oral hygiene practices. However, the 24
hour diet chart revealed that she ate sugary snacks during and after the college times and taking dinner without brushing or rinsing her
teeth immediately afterward.
On Intra-oral examination, it was found that following teeth had
been restored with glass ionomer cement: teeth numbers 47, 37, 17
and 26 in addition, teeth numbers 46, 48,and 36 had deep pit and
fissures. Since we were looking at more sensitive index, ICDAS was
used because it had continuum to caries pathway from sound tooth to
distinct cavitation [6]. Considering patients caries status, we planned
to conduct a risk assessment using cariogram including one week
diet chart. Caries risk assessment was done and data was collected as
suggested by Bratthall [7].
Cariogram assessment:
Patient data was obtained for all the parameters enlisted in the
cariogram and it revealed that patient had 44% actual chance to avoid
new cavities and contribution of planned diet was 22% (Figure 1).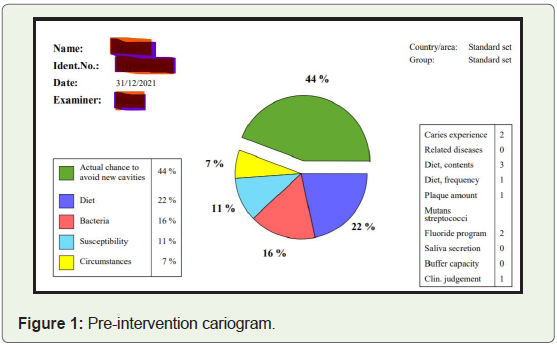
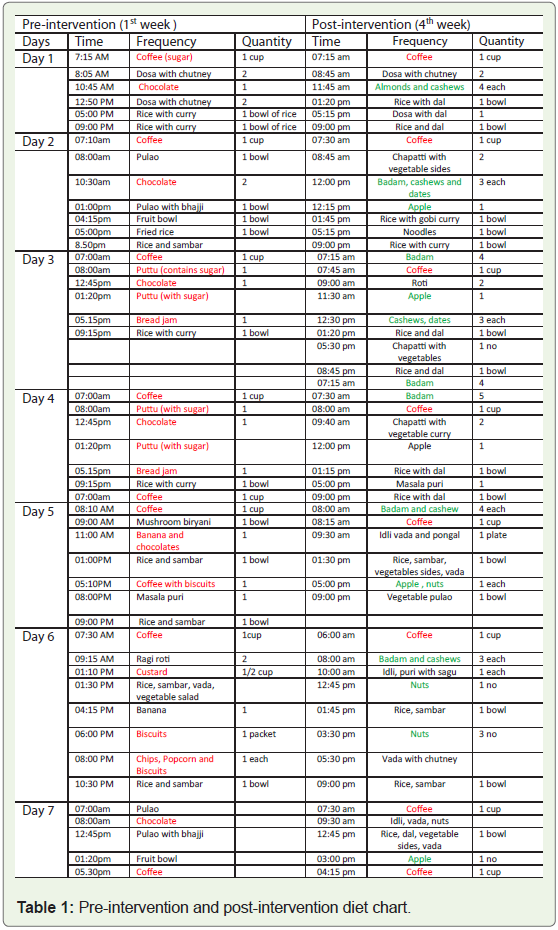
Diet chart analysis:
Patient was asked to submit the diet chart for 7 days including
time, frequency and consistency of food that she ate. The detailed
analysis of the 7 days diet chart revealed the in-between sugar
snacking and the frequency of consumption was 4-5 times per day
and consistency of food was predominately retentive and the average
sugar-score for a week was 37.14, hence intervention was to reduce
in-between consumption.Intervention plan:
The cariogram output suggested that the diet with respect to its
content of fermentable carbohydrates is a problem - a reduced intake
of such products would be an advantage. Hence intervention was
planned for diet counseling and for preventive regime. Rationale for
diet counseling was the frequency of cariogenic diet, consistency, and
in-between consumption.First session:
It included familiarizing patient with balance diet, food
pyramid, and the beneficial effects of all the foods in the pyramid
and importance of balanced diet. Patient was also informed about
oral health including types of dentition, simple oral diseases and
emphasizing dental caries. Patient was also explained about the role
of cariogenic diet in causing dental caries, stages of dental caries andremineralization and demineralization using Stephen’s curve [5].
However comprehension was maintained and technical terms were
not used.Second session:
It started with reinforcing first session contents and diet chart
analysis of the patient. And patient herself was able to appreciate the
frequency, consistency and in-between snacking behaviour being
responsible for dental caries. The second session ended up with
requesting the patient to submit alternate replacements for the snacks
she was consuming.Third session:
The patient came up with alternate diet with suggestion of nuts
and fruits. Basically patient was into the behaviour of consuming
quick snacks to overcome the stress.Considering the patient suggestion, it was reinforced the
importance of planned diet and beneficial effects of these foods and
the patient was motivated to adhere to this plan. Following which
patient was asked to maintain diet chart for subsequent second and
third week. Timely Whatsapp messages were sent to the patient
reinforcing the beneficial effect and exactly at those timings were in
the habit of consuming sugary snacks.
Similarly, second and third week diet chart was submitted by the
patient. The analysis indicated that, there were not many changes in
the diet chart in the second week whereas in the third week diet chart
showed drastic improvement. Sugar score was calculated based on
the form, frequency and consistency of sugar intake by classifying
each sugarintake into liquid, solid and sticky or slowly dissolving
using Nizel and Papas 24 hour diet method [5]. Table 1 shows pre
and post intervention of diet chart and Table 2 shows the average and
composite score for sugar consumption for each week. The average
sugar score calculated for fourth week was 5.7. Along with this patient
was also instructed to rinse her mouth each time after consumption
of food.

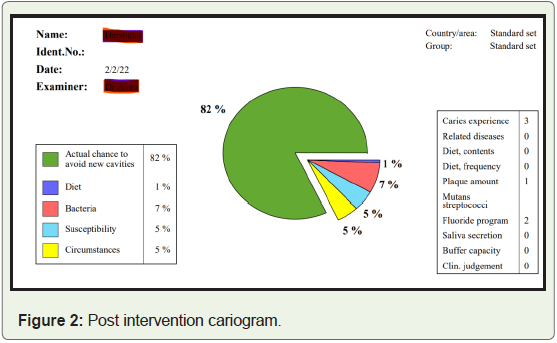
Fourth week risk assessment revealed that patient had 82% actual
chance to avoid new cavities and contribution of diet was 1% (Figure 2).
Discussion
It was very clear that consistency, frequency and in-between
snacking habit played a major role in causing dental caries [8]. This
relationship between dietary habits and dental caries was proven
by Vipeholm study [8]. Tailor made interventions, active patient
participation in planning diet, motivation and reinforcement for
patient compliance to treatment regimen contributes to effectiveness
of interventions demonstrated as decreased total diet score and change
in diet pattern [9]. Rather than considering the total score, from the
diet chart, detailed analysis of diet chart is more beneficial. It gave
us better idea about the in-between meal consumption, frequency of
snacking and quality of food which facilitated in patient education
about diet and dental caries and also planning interventions. The
change in diet pattern was evident after 4 weeks which was backed
with 3 face to face sessions and frequent reinforcement messages.
However, the sustainability of the changed behaviour is yet to be
studied.
Also, patient had the background of science therefore using the
language such as balanced diet, food guide, and pyramid helped us
to maintain the comprehension level. Understanding literacy level
of patient is very important for patient compliance and successful
dietary intervention. Hence this method appears to be promising
in bringing about changes in individual level, however for future
direction we would recommend to develop a diet chart which can
be scored for type of food, frequency and time which can enhance
sensitivity and contribute to evidence. This particular case report
has shown promising results with diet counseling as an intervention,
however more number of cases in the future is recommended.
References
Citation
Amra S, Pushpanjali K. Diet Analysis and Counseling for Caries Prevention: A Case Report. Indian J Nutri. 2022;9(2): 259.