Research Article
Obesity and Health Related Quality of Life among the Housewives in a Selected Rural Community of South India - A Correlation Study
Mokshitha* and Fernandes SL
Laxmi memorial college of Nursing, Balmatta, Mangaluru, Karnataka, India
*Corresponding author: Mokshitha, Laxmi memorial college of Nursing, Balmatta, Mangaluru, Karnataka, India; E-mail:
mokshabantwala@gmail.com
Article Information: Submission: 07/03/2022; Accepted: 05/05/2022; Published: 09/05/2022
Copyright: © 2022 Mokshitha, et al. This is an open access article distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Obesity is a global health problem. It has emerged as the most prevalent serious public health problem. A descriptive correlative approach was adopted
to find out the correlation between obesity and Health Related Quality of Life (HRQoL) among housewives in selected rural community of Bantwala,
Dakshinakannda, Karnataka. A number of 200 housewives who are aged between 18-70 years were selected by using purposive sampling technique.
Housewives were categorized as normal weight, overweight, obese using Body Mass Index (BMI) calculation formula i.e, BMI=Weight in (kg)/Height in
(m2) and HRQoL measured by using SF36 questionnaire. Result showed that, maximum percentage (37.5%) of obese housewives were in the age group
of 58-70 years. Among subject’s majority (46%) of housewives were had normal weight, 20% were obese and 34% were overweight. Correlation between
obesity and physical functioning (r= -0.45P=0.004), Energy/Fatigue(r= -8.91P=<0.00001) and Pain (r= -0.49 P=0.0013) shows positive correlation and highly
Significant. Results also showed that there was significant association of HROoL with age (p=.001). It is recommended to conduct longitudinal studies to find
the relationship between and obesity and Health Related Quality of Life (HRQoL) among rural housewives.
Keywords
Obesity; Health Related Quality of Life; Housewives; Rural community
Introduction
Obesity due to increased weight has become a global epidemic
everywhere. World health organization estimated that, there will be
about 2.3 billion overweight people and over 700 million obese people
worldwide in 2015 [1]. Over the period of 1960 to 2004 adults between
the age of 20 and 74 years were classified as obese raised from 44.9%
to 66.2% respectively. The rate of individual who are overweight but
not obese ranged from 31.5% to 33.4% over the same time period [2].
India, with 1.2 billion people is the second most populous country
in the world and is currently experiencing rapid epidemiological
transition and witness higher prevalence of non-communicable
diseases in adults [3]. In addition, 44% of the diabetes burden, 23% of
the ischemic heart disease and between 7% and 41% of certain cancer
burdens are contributing to the problems of overweight or obesity
[1]. Under nutrition due to poverty dominated the past, is being
rapidly replaced by obesity. Industrialization and urbanization also contributes to increased prevalence of obesity. Studies from different
parts of India have provided evidence of the rising prevalence of
obesity. However, most reports have been region specific. The
prevalence rate of generalized obesity in urban south Indians was
4% using BMI>30; 9.9% using BMI>27.5; 26.5% using BMI>25; and
45.9% using BMI>23 kg m−2 [4,5]. Further, different studies have
used different methodologies, definitions and cut-off points for
defining obesity, making comparisons difficult [6,7]. Researcher had
interactions with many women in the rural communities found that
most of them appeared obese for their size and stature and felt the
need to conduct a study on the correlation of obesity and health related
quality of life among women in the selected rural communities.
Materials & methods
A descriptive correlative approach was adopted to find out
the correlation between obesity and Health Related Quality of Life
(HRQoL) among housewives in selected rural community of Bantwala, Dakshina Kannda, Karnataka. A number of 200 housewives who
are aged between 18-70 were selected by using purposive sampling
technique. Prior to data collection, permission was obtained from the
concerned authority for conducting the study. Subjects were selected
according to the selection criteria and confidentiality was taken into
account. The purpose of the research study was explained to the
subjects. Height and weight were measured by using inchtape and
calibrated weighing machine. Housewives were categorized as normal
weight, overweight and obese by using BMI calculation formula, i.e,
BMI=Weight in (kg)/ Height in (m2) and HRQoL was measured by
using SF36 questionnaire. The data obtained was analysed by both
descriptive and inferential statistics on the basis of objectives of the
study. Karl Pearson correlation coefficient and scatter diagram were
used to find the correlation between Obesity and HRQoL.
Results
Result showed that, maximum percentage (37.5%) of obese
housewives were in the age group of 58-70 years, whereas maximum
percentage (39.71%) overweight housewives were in the age group
of 38-47years. Among subject’s, majority (46%) of housewives were
normal weight, 20% were obese and 34% were overweight. BMI of
the housewives ranged between 19.6 - 37.1 and mean was 23.04±4.24.
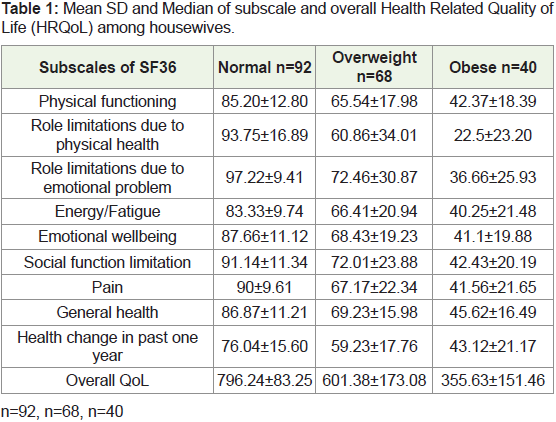
Table 1 shows that obese and overweight housewives had
less mean score in all sub scales of HROoL in comparison with
normal weight housewives. Overall HROoL mean of, obese
housewives were 355.63±151.46, overweight housewives were
601.38±173.08 and Normal housewives were 796.24±83.25.
Correlation between obesity and physical functioning (r= -0.45
P=0.004), and Pain (r= -0.49 P=0.0013) shows negative correlation
and Significant. Correlation between obesity and Energy/Fatigue
(r= -0.20 P=0.21) , Role limitations due to physical health (r=
-0.15P=0.36), Role limitations due to emotional problem(r= -0.01
P=0.95), Emotional wellbeing (r= -0.22 P=0.172), Social functioning
(r= -0.17P=0.29), General health (r= -0.13P=0.42), Health change(r=
-0.24 P=0.14)and overall QoL among obese sub scales shows negative
correlation and non-significance. Results also showed that there was
significant association of HROoL with age (p=.001).
Discussion
The findings of the present study showed that majority of (37.5%)
of obese housewives were in the age group of 58-70 years, whereas
(39.71%) overweight housewives were in the age group 38 to 47.
The study on Overweight and obesity among women by Economic
Stratum in Urban India contradicts the present study findings where
prevalence of overweight and obesity is higher among urban women
than their rural counterparts. More than 23% of women in the urban
area are either overweight or obese compared to only 7% of women
in rural areas [8].
A cross-sectional analysis on obesity and health-related quality
of life of the US population by M k Hassan, AV Joshi, SS Madhavan,
showed approximately 36% overweight, 14% obese, and 7% severely
obese [9]
Research conducted among 10,308 British civil servants reported
a significant linear trend between increasing BMI and poor physical
functioning [10]. In the present study Correlation between obesity
and physical functioning (r= 0.45 P=0.004) shows significance. Lack of
association was observed when more detailed mental health subscales
were used, and whether or not the mental health was adjusted for
clinical (and sub threshold) depression. The lack of significant
differences in mental health between obese and non obese subjects has
been reported previously in U.S. community-based studies [11,12].
Current study shows Correlation between obesity and Role limitation
due to emotional problem(r= -0.01 P=0.95), Emotional wellbeing (r=
-0.22 P=0.172), Social functioning (r=ions due to physical health(r=
-0.15P=0.36), Social functioning (r= -0.17P=0.29),General health (r=
-0.13 P=0.42), Health change(r= -0.24 P=0.14)and overall QoL among
obese sub scales shows negative correlation and non-significance.
Obese and overweight women overall health more negatively have
poor health than normal weight women [13,14]. This finding was
more generalized when perception of subscales results about general
health was showing negative correlation , Further decreases in vitality
were prominent in obese women. Other investigators have also
shown lower SF-36 scores for general health perceptions and vitality
in patients seeking treatment for obesity (mean BMI, 38.1 kg/m2) [15].
Furthermore, IT IS recommended to conduct longitudinal studies to
find the relationship between and obesity and Health Related Quality
of Life (HRQoL) among rural housewives.
Conclusion
Obesity has emerged as the most prevalent serious public health
problem. It is a complex disorder, which is a detrimental to good
health and well being. There is a growing body of literature describing
its association with lower Health Related Quality of Life (HRQoL).
When comparing these two variables a common or unique feature
arises i.e., both these variables can be prevented and the effect of these
variables can be reduced to some extent by adequate precautions. As
a nursing personnel, it is our duty and responsibility to ensure that
the mortality and morbidity caused by obesity can be reduced as soon
as possible.