Research Article
Nutritional Status of Under Five Children of Migrant Labourers at Construction Sites in Haveli Taluka, Pune, Maharashtra
Singh B*
Rostrum India Social Organization, India
*Corresponding author: Singh B, RISO, NGO (Rostrum India Social Organization), India, Email: bharti987123@gmail.com
Article Information: Submission: 09/01/2022; Accepted: 17/02/2022; Published: 28/02/2022
Copyright: © 2022 Singh B. This is an open access article distributed under the Creative Commons Attribution License, which permits
unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Seasonal migration for work is a persistent reality in India. Around 120 million people are estimated to migrate from rural areas to urban labour markets.
This study examines the nutritional status of fewer than five children of migrant construction workers who live on construction sites with their parents. Nutrition
is one of the impacting factors during the growth and development period of a child. India accounts for 40% undernourished children in the world. According
to NFHS- 4, 35.5% under five children are underweight, 38.4% stunted, 21% wasted in India. Community-based cross- sectional study, field work of this study
was undertaken between Jan 2020 and March 2020 at five construction sites in Haveli Taluka of Pune city. Construction sites were conveniently selected. The
study population was children fewer than five age group present at the construction sites during data collection and their mothers. Data was gathered from
children (N=85) using anthropometric measurements and semi-structured questionnaire for their mother. The mean age of study sample was 37.12 months,
44.7% male (n=38) and 55.3% female (n=47). The overall prevalence of Underweight (Weight for age < –2SD) was 41.2%, stunting (Height for Age <– 2SD)
28.2% and wasting (Weight for Height < – 2SD) 32.9%. Birth spacing, intake of IFA during pregnancy, and source of drinking water at construction sites were
significantly associated with prevalence of wasting among children (p <0.05). Birth spacing was significantly associated with stunting (p<0.05). Consumption
of IFA during pregnancy was significantly associated with underweight (p<0.05). Study addresses the gap in context to migrant labourers and the health status
of their children in India. Study highlights the necessity to focus on the specific needs of migrant children.
Keywords
Migrant labourers; Fewer than five age group children; Under nutrition; Construction sites
Introduction
Malnutrition accounts for half of all childhood death worldwide.
Sometimes, young children are not able to utilize the food they eat,
which leads to under nutrition or at times if they consume too many
calories which lead to obesity or over-nutrition [1]. Individuals are
considered malnourished when the calories intake and protein intake
in their diet is not sufficient enough for their overall growth and
development. Malnutrition is one of the significant factors that affect
the growth of children [2]. Food given to the child during the first
five years determines the child’s nutritional status. During the period
of childhood growth, nutrition plays an important influencing factor
[2]. Malnutrition has been accountable for 60% of the 10.9 million
deaths that occur annually among children under five years of age
[3]. Globally, the prevalence of stunting is 20.1%, underweight 13.1%
and wasting 9% in children fewer than five years of age [4]. Globally, 159 million children are stunted. Fifty million children under five age
group are wasted, and 16 million are severely wasted in under five
age group [2,3]. The degree of the problem of malnutrition among
children is high throughout India [2]. India accounts for 40% of
undernourished children in the world. Prevalence of under-nutrition
among the states of India ranges from 27% to 55% [7]. According to
the NFHS- 4, 35.7% of children under the age of five in the country
are underweight, 38.4% are stunted and 21% are wasted.
Across the Indian sub-continent, the movement of workers is
an age-old phenomenon. The 2001 Census of India recorded 309
million internal migrants. While 2007-2008 National Sample Survey
Office recorded 326 million internal migrants in India (UNESCO,
2013). The recent estimates based on the census of 2011 show that the
number of internal migrants in India is likely to touch 400 million
by 2020. A large number of people from rural India, especially from the flood-affected, rain- dependent and drought-prone regions, are
forced to migrate in search of a livelihood [5]. It is usually associated
with the changing patterns of economic development and partly
related to the levels of poverty [8].
In India, there is primarily of two types of migration. Longterm
migration results in the shifting of an individual or household
and short-term or seasonal migration that involves back and forth
movement between a source and destination. Approximately short
term migrants vary from 15 million to 100 million. 30% of the
total Indian population is migrants who have relocated within and
outside the states [13]. Majority of the short-term migrants belong
to socioeconomically deprived groups having negligible educational
attainment, inadequate assets, and resource deficits [8].
It is estimated that around 40 million migrant labourers are
in the construction industry. These labourers have contributed to
the country’s developing economy. Short-duration rural to urban
migration provide livelihood to millions of poor households in India
[6]. Migrant households in the city mostly involved in temporary
work. This temporary work is often characterized by low paid wages,
job insecurity, strict recruitment regimes, and economic vulnerability.
They are mostly engaged in informal work environments. Many of
these labourers migrate with their entire families, including their
young children and live in very challenging conditions [6,7]. Child
migrants in India are estimated to be around 15 million [8].
Literature had documented several threats to the health status
and well-being of migrant children in India. Migrant households in
urban lands face great difficulties in accessing government programs
related to health care and insurance, childcare, education [9,10], and
food rations, which is otherwise accessible in rural settings. But the
interdependent relationship of these threats to the health and wellbeing
of the child is often overlooked [7].
Even though migration provides economic opportunities to
households, but migrant children face several disadvantages in the
destination region.
Assessment of nutrition status is necessary for early detection
of malnutrition and for assessing the effectiveness of preventive
programs. Anthropometry is widely used and recognized as one of
the useful techniques to assess the growth and nutritional status of an
individual or population [11,12].
The goal of this study is ascertain the nutritional status using
anthropometric measurement and to analyze the factors associated
with the nutritional status of under-five children of migrant
construction workers.
Methodology
Study Design & Setting:
A community based cross-sectional study was undertaken in
Pune, located in the western part of the state of Maharashtra. Pune
has 5 district sub-divisions with 15 talukas. The study was conducted
among under-five age group children and their mothers residing at
the construction sites in Pune. The study was conducted from January
2020 - June 2020 at five construction sites in the Haveli Taluka of Pune city. The five construction sites namely Bavdhan, Yewlewadi,
Uttamnagar, Undri, and Padmavati, were conveniently selected
to assess the nutritional status of children under five age groups of
migrant construction workers. Access to these construction sites
was provided by the organization that runs the education center for
workers’ children.Study Participants:
The study population of this study was children fewer than five
age group present at the construction sites and their mothers who
lived for at least more than a month or more than six months at the
construction sites.Inclusion Criteria:
• All the children in the age group of 0-5 years present at the
study site
• Mothers should have had at least one child in the under-five
age group.Exclusion Criteria:
• Children not in the age group of 0-5 years
• Mothers who do not have at least one child in the under-five
age group.Sampling Size & Sampling Technique:
Children in the age group 0-5 years who were present at the
study site were checked for the eligibility criteria. 85 children [44.7%
male (n=38) and 55.3% female (n=47); (Mean age: 37.12 months)]
participated in the study. Mothers (N = 58) of the children enrolled in
the study were interviewed.Data Collection:
The Institute’s ethical committee approval for the study was
obtained before the commencement of the study. Written informed
consent was obtained prior to the study, which was signed by the
mothers. This was followed by a cross-sectional survey conducted at
the study site by taking anthropometric measurements of the children
and conversation with their mothers to obtain information on their
socio-demographic, child feeding and caring characteristics, maternal
characteristics, and WASH practices based on the questionnaire. For
identification and initial contact, the help of co-ordinator from NGO
was obtained to minimize the non-response.Height/length and weight of the children under five years of
age were measured to gather the anthropometric data. The weight
measurements were recorded to the nearest 100 g using Standard
weighing machine. The height of the children was recorded to the
nearest 0.1 cm using anthropometric height rod. For children below
24 months of age, the length was measured using infantometer.
After every case examination, calibration for the weight and height
instruments was done. All measurements were taken twice, and the
mean value was obtained and used for data analysis. Weight of the
child was measured in grams, and height was measured in centimeter.
Data Analysis:
IBM Statistical Program for Social Sciences (SPSS) trial version 25 was used to perform statistical analyses. WHO Anthro (version
3.2.2, 2011) was used to compute z-score values of weight for height
(WHZ), height for age (HAZ), and weight for age (WAZ). The results
were presented using frequency tables and percentages and a chi
square test was performed to investigate the association between
the selected variable and the nutritional status. For anthropometric
measurements, data analysis was performed using “WHO Anthro”
software. This software converts the anthropometric measures;
weight, height/ length and age values into Z-scores values of height
for age (HAZ), weight for height (WHZ), and weight for age (WAZ).
It categorizes nutritional status as stunting, wasting and underweight
respectively among children who were minus two standard deviations
below the reference population.Children are categorized into two groups, ‘suffering from
undernutrition’ (Z- score less than - 2 SD) and ‘not suffering from
under nutrition (Z-score equal to or greater than – 2SD), for each of
the three indicators.
Results
Socio-demographic profile of under-five children:
Among total of 85 migrant children, 4.7% (n=4) were between
the age group of 6- 11 months, 10.5% (n=19) were in the age group of
12-23 months, 10.5 % (n=19) were in the age group of 24-35 months,
15.29% (n=13) were in the age group of 36-47 months, and 35.29%
(n=30) were in the age group of 48-60 months. The mean age of study
sample is 37.12 months with 44.7% male (n=38) and 55.3% female
(n=47) as seen in Figure 1. Mean height and weight of the sample
is 89.81 cm and 11.4 kg, respectively. Majority of the participants
were in the age group 48-60 months. Majority of the children (91.8%)
were Hindu by religion, followed by Muslims 5.9%, and 2.3% were
Christians. About mother’s education, 32 (37.6%) were illiterate,
31(36.5%) had primary schooling, 21 (24.7%) had higher secondary
and 1 (1.2%) were senior secondary educated mothers. 51 (60%)
mothers were working as labourers, and 34 (40%) were currently not
working as labourers at construction sites. Majority of children came
from the states of Chhattisgarh which was followed by Maharashtra
and Karnataka. And the native state for the remaining children was
Kolkata, Jharkhand, Telangana, Madhya Pradesh, and West Bengal.
According to caste, the majority of children belonged to Scheduled
Tribes (ST), while the others were from Scheduled Castes (SC), Other
Backward Classes (OBC), and general category.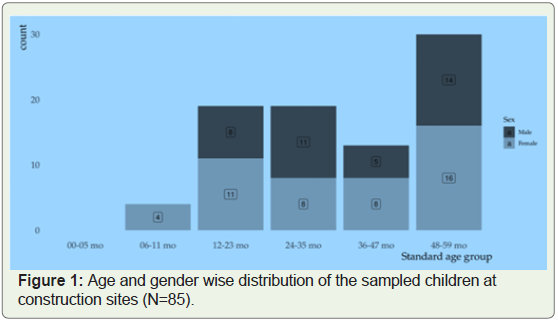
There were 36 (42.4%) mothers who were married before the age
of 18 years. 14 (16.5%) children were born as low birth weight babies.
Majority, 58 (68.2%) of childbirth were in the hospital, whereas 27
(31.8%) children were born at home.
Under nutrition among under-five children:
Among study subjects, the overall prevalence of Underweight was
41.2 %, stunting was 28.2% and, wasting was 32.9% as seen in Table 1.
Wasting was found to be more prevalent among males (36.8%) than
females (29.8%). Underweight was found to be more prevalent among
males (42.1%) as compared to females (40.4%). Stunting was found to
be more prevalent among males (31.6%) than females (25.5%). The
category wise prevalence of under nutrition among boys and girls are
seen in Table1. Underweight was found to be most prevalent (53.8%)
in the age 36-47 months’ group. Stunting was found to be more
prevalent (36.8%) in the 24-35 months’ age group, while wasting was
more prevalent (46.7%) in the 48-60 months’ age group as seen in
Table 1.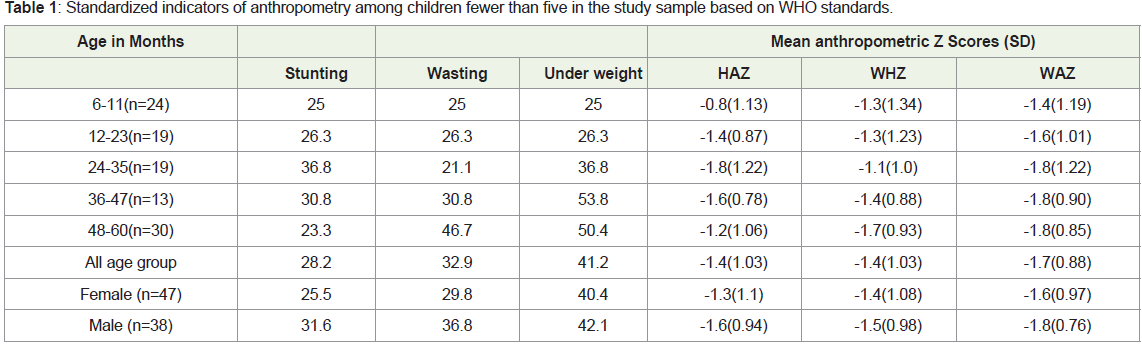
Childhood illness and WASH Practices:
There were 45.9% (n=39) children with the history of eating junk
food. The source of drinking water for majority 69.4% (n=59) was
tanker, followed by bore well 20% (n=17), and 10.6% (n=9) was filter
bottle (10 liter). 55.3% (n=47) study participants had sharing toilet
facilities at the construction sites. There were 49.4% (n=42) children
who defecate in open. More than half of the study participants 54.1%
(n=46) don’t wash their hands before eating food. Almost 37.6%
(n=32) children fell ill in the last two weeks. 43.55 (n=37) mothers
noticed their child eating sand at construction sites. About 32.9%
(n=28) had given deworming medicines to their children. Only 14.1%
(n=12) mothers’ carried their child’s immunization card from their
native state.Statistical Association:
Birth spacing, intake of IFA during pregnancy, and source of
drinking water at construction sites was significantly associated with
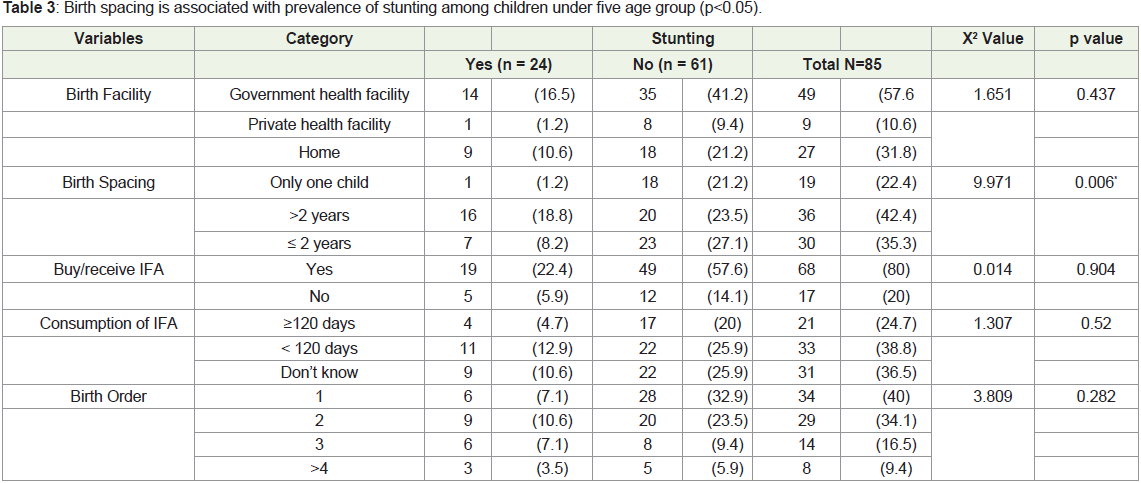
the prevalence of wasting among children (p <0.05) as seen in Table 2. Birth spacing was significantly associated with stunting among
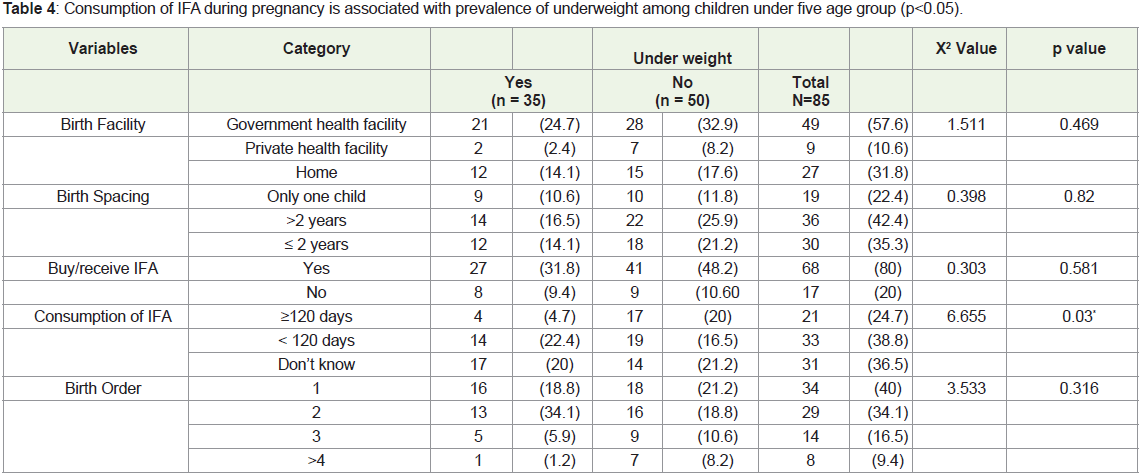
children (p<0.05) as seen in Table 3. Consumption of IFA during
pregnancy was significantly associated with underweight (p < 0.05)
as seen in Table 4.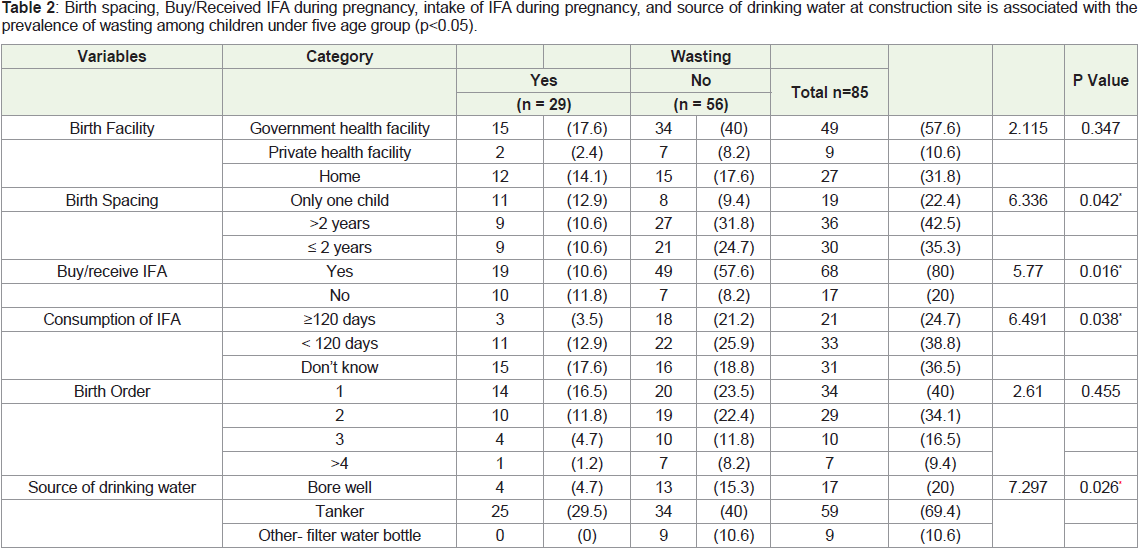
Discussion
Stunting:
The percentage of children who were stunted (28.2%) was less
as compared to a similar study carried out at construction sites of
Ahmadabad [6]. Stunting indicating chronic malnutrition accounted
for around 28.2% of total under nutrition among fewer than five
children residing in the study area. This creates a picture of concern
and need for immediate attention to reduce the burden of a nutritional
problem country is facing from a long way.Underweight:
Underweight accounted for around 41.2% of total under nutrition
among fewer than five children residing in the study area. Different
studies conducted in a similar setting in urban areas of various places in India reported the prevalence of underweight ranging from 40 -
60% among under five children [6,12,13,14].Wasting:
Wasting was prevalent in 32.9% of the study subjects. Similar
studies conducted at Maharashtra (Mali et al at Panvel Taluka) also
reported that 36% of fewer than five children were victim of wasting.
Prevalence of wasting lower than this study was reported in study by
Divya et al (22.1%) and Agarwal and Srivastava (17.6%).According to National Family Health Survey (NFHS 2015-2016),
the prevalence of stunting, wasting, and underweight is 38.4%, 21%,
and 35.7% respectively. The percentage of stunting (28.2%) among
migrant children in this study was less than the national average. The
percentage of underweight children (41.2%) and wasting (32.9%) was
noticeably higher.
Birth spacing and childhood malnutrition:
Analysis of the H/A and W/H measurement showed a significant
association between malnutrition and Birth spacing. The findings
of this study are similar as well as comparable [15]. This could be
explained by the fact that if a pregnancy occurs too soon after the
previous birth, the mother may not have recovered her nutritional
status, which can contribute to preterm birth and low birth weight.
Knowledge regarding birth spacing among women will allow women
to recover and be healthy for their next pregnancy. Mothers who
adequately space their pregnancies are able to provide their children
with the necessary nutrition for growth development and a strong
immune system, thereby reducing the likelihood of childhood under
nutrition [12].A survey in urban setting of Indore, Madhya Pradesh by Ahmed
Shahjada reported that the children with birth interval of less than
24 months suffered more from different grades of malnutrition [16].
Survey by NFHSIII (2006, India) confirmed that 48% children were
malnourished when interval between two pregnancies was ≤ 24
months [3]. All evidences support low birth spacing as a risk factor
of children malnutrition irrespective of demography of population.
IFA and childhood malnutrition:
The major cause of anemia among pregnant women in India
is Iron deficiency [17]. There has been a focus on providing IFAs
to pregnant women through national nutritional programmes.
Iron-deficiency anemia is still prevalent in India despite of various
nutritional programmes [16]. A study conducted on the role of
IFA supplements in influencing the birth weight through the data
from NFHS 2005-06 findings state that birth weight increased by
6.46 g after intake of IFAs during pregnancy for 1 month [16]. In
this study, 20 % of mothers did not buy/receive IFA tablets during
their last pregnancy. About 38.8 % reported intake of IFA for less
than 120 days during pregnancy and 24.7% for more than 120 days
during pregnancy. Nutritional status of pregnant women can be
improved through multi-pronged approach. All private and public
health centers should have IFA tablets accessible for women. Sessions
should be offered for adequate intake of IFA tablets. Intake of IFA
tablets should be monitored throughout the pregnancy.Source of drinking water at construction sites and childhood malnutrition:
In this study source of drinking water showed a significant
association with child malnutrition. A similar study in Bangladesh
and Rwanda reports a significant association between the source of
drinking water and malnutrition [10,17]. These are plausible because
safe source of drinking water is the pre-conditions for maintaining
good hygiene and nutrition among children. Various water-borne
illnesses can be prevented with the improved supply of drinking
water. Therefore, increasing access to safe drinking water is important
to improve the nutritional status of under-five children [10,17]. The
study did not find any association with the mother’s education, birth
order, caste which is consistent with other studies [1,6,7].Conclusion & Recommendation
Indian economy will continue to expand and urbanize. Labour
migration will play an important role in expanding the Indian
economy. Labor migration will undoubtedly continue as a mode of survival among rural households. In India over the last decade in
spite of economic growth the improvement in childhood nutritional
status has been slow. The values of undernutrition have changed in
the last two NFHS surveys. The present values of stunting, wasting,
and underweight are still high among children below five years of age.
The nutritional status of fewer than five children is also considered as
a measurement of quality of life along with a susceptible indicator of
the health of a country.
The government programs should expand their services. Also,
special provisions should be made to reach migrant communities.
These communities are among the most vulnerable communities in
the country. Through this study a critical gap in the literature have
been addressed. This study also explains the need to broaden the
policy framework to incorporate and address the concerns of migrant
workers.
When children have adequate access to affordable food, variety
of nutrient-rich food, combined with good maternal health and
childcare practices, then the optimal nutritional status of children can
be achieved. Also access to good healthcare services along with good
environmental conditions has an influence on child’s nutritional
status. These factors are further influenced by Social, economic,
and political variables. This study proposes the urgent need for
strengthening the existing health and nutritional programmes which
will help to reduce the prevalence of malnutrition in such children of
the migratory population. As growth impairment during childhood
has several consequences on physical and cognitive development.
These consequences include decreased school performance and
productivity in general. It adds to being a risk factor for chronic
diseases later in life. These consequences are more prevalent in the
children of the migratory population. Migrant children living in
poverty will have similar labor and productivity outcomes as their
parents, thereby continuing the poverty and malnutrition cycle.
References
Citation
Singh B. Nutritional Status of Under Five Children of Migrant Labourers at Construction Sites in Haveli Taluka, Pune, Maharashtra. Indian J Nutri. 2022;9(1): 249.