Research Article
Management of Amavata/Rheumatoid Arthritis with Langhan (Fasting), Sunthi (dried ginger) and Trikatu - an Ayurvedic Polyherbal Formulation
Deo K1, Pendse N2 and Udipi SA3*
1Former Student, Department of Food Science and Nutrition, SNDT Women’s University
2Seth Tarachand Hospital, Pune
3Integrative Nutrition and Ayurceuticals, Kasturba Health Society- Medical Research Centre and Former Professor and Head,
Department of Food Science and Nutrition, SNDT Women’s University
*Corresponding author: Udipi SA, Integrative Nutrition and Ayurceuticals, Kasturba Health Society- Medical Research Centre,
Jain Sthanakwasi Aradhanadham 17, Khandubhai Desai Road, Santacruz (West), Mumbai - 400 056 Cell: +91 9189324083; E-mail:
drshobhaudipi@gmail.com
Article Information: Submission: 15/01/2022; Accepted: 18/02/2022; Published: 21/02/2022
Copyright: © 2022 Deo K, et al. This is an open access article distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Amavata, a progressively debilitating, disabling condition, is similar to rheumatoid arthritis that occurs in nearly 1% of the population. Rheumatoid arthritis
is generally treated with anti-inflammatory drugs to slow down its progression and save joints and tissues from permanent damage. However, these drugs
have side effects. In Ayurveda, Langhan / modified fasting and use of ginger or Trikatu, a three herbal formulation is recommended. In the present study, a
combination of Langhan plus a decoction prepared from either Ginger powder/Sunthi or Trikatu was studied. Patients were randomly assigned to the Sunthi
group (n=32) or Trikatu (n=36). Functionality was assessed using the HAQ disability index, Ritchie’s articular index and grip strength. Symptoms like pain,
fever, and gastrointestinal problems were assessed on Days 0, 7 and 14. The HAQ-DI assessed the amount/level of difficulty experienced in performing
common daily activities. Ritchie’s Articular Index assessed six joints of fingers, wrist, elbow, shoulder, knee and ankle on the left and the right side as a
single unit for pain, swelling, warmth, and limitation of motion. Both treatments were effective but benefits were better and side effects were less with Sunthi.
Also, benefits with Sunthi were seen in the first week of treatment. The duration of this study was only 14 days, as patients found it difficult to adhere to the
diet particularly because wheat was restricted completely, resulting in a high number of dropouts. Further study on modification of diets for patients with RA/
Amavata to obtain maximum benefits would be worthwhile.
Keywords
Rheumatoid Arthritis; Amavata; Ginger; Trikatu; Functionality; Disability Index
Abbreviations
Rheumatoid Arthritis - RA; Gastrointestinal - GI; HAQ-DI - Health
Assessment Questionnaire-Disability Index; RAI - Ritchie’s Articular
Index; BMI - Body Mass Index; WHO - World Health Organization,
RDA - Recommended Dietary Allowances, IL-6 - Interleukin-6; CRP
- C-Reactive Protein; IgM - Immunoglobulin M; TNF-α - Tumour
Necrotic Factor-α; GLP-1 - Glucagon-like Peptide-1.
Introduction
Amavata is a chronic, progressive disease that clinically resembles rheumatoid arthritis (RA) and is characterized by inflammation of
joints and surrounding tissues, swelling, pain in ankles, knees, hips,
elbows, shoulders, as well as joint deformity. Ayurveda considers
Amavata to be a manifestation of the vitiation of Vatadosha and
localization and accumulation of Ama in the joints, resulting in pain,
stiffness, swelling and tenderness in the joints [1]. Ama is believed
to be cellular and metabolic waste/toxic material generated in the
gastrointestinal (GI) system and cells due to improper diet and
impaired metabolism.
Modern medicine generally relies upon anti-inflammatory drugs i.e., Analgesics, Steroids and disease-modifying drugs for treating RA.
However, there is not much to offer in terms of dietary management.
In Ayurveda however, treatment is multi-faceted in which Deepana
i.e., selected plant materials like ginger (Zingiber officinale), pepper
(Piper nigrum), long pepper (Piperlongum) are used and dietary
measures are advised depending on whether Amavata is chronic
or acute. These include Langhan/ abstinence from food totally or
consuming light and easily digestible foods, while some foods are not
permitted [1]. The treatment aims to remove the accumulated Ama,
keep further production in check, cleanse the circulatory channels and
pacify the vitiated dosha. Furst et al., (2011) conducted one of the first
randomized, double-blind controlled study comparing methotrexate
with ayurvedic treatment and their combination [2]. While efficacy
was similar in all three treatment groups, the Ayurveda only group
had fewer side effects. In this context, we undertook a clinic-based
study of Amavata involving Langhan along with dry ginger/Sunthi,
or Trikatu a combination of Sunthi, pepper and long pepper.
Methodology
Sample selection: Outdoor patients attending the Seth Tarachand
Ramnath Hospital, Pune were recruited after obtaining permission
from the hospital and informed written consent, based on the
following inclusion and exclusion criteria.
Inclusion criteria: Patients between 20 and 70 years of age,
diagnosed with Amavata by the Ayurvedic physician, at least 4
weeks prior to the start of the study, who were not concurrently
taking medications from other systems of medicine and any other
medications. Patients should satisfy at least four of the American
College of Rheumatism criteria: morning stiffness, arthritis of three
or more joints, arthritis of hands, symmetric arthritis, rheumatoid
nodules, positive rheumatoid factor and /or radiographic changes.
Exclusion criteria: Patients concurrently taking allopathic and/
or homoeopathic treatment, pregnant and lactating women, those
clinically not advised langhan e.g., diabetes mellitus or tuberculosis
or serious complications associated with any other systemic disease.
Sample size: Initially 68 patients were enrolled and 32 were
randomly assigned to the Sunthi group and 36 to the Trikatu group,
irrespective of their prakriti or chronicity and severity of the disease.
Weekly follow up was done.
At the first follow up on Day 7, 17 patients from the Sunthi
group did not return. On Day 14, another 10 patients in this group
had dropped out. In the Trikatu group, from the 36 patients initially
assigned, 19 patients did not return for the first follow up and 12 more
had dropped out by Day 14. Due to a lack of sufficient subjects, the
study was discontinued on Day 14.
Intervention: After baseline measurements, each participant in
the Sunthi group was given 14 packets, each containing 6 grams of
Sunthi. Similarly, the Trikatu group participants received 14 packets
of Trikatu (6 g/packet). Each packet of Trikatu contained 2g each of
the three constituents dried ginger powder (Sunthi), powdered long
pepper (Pippali) and powdered black pepper (Marich).
Patients were instructed to prepare a decoction as follows, using
one packet per day. The Sunthi or Trikatu was to be boiled with 1 cup (150 ml) of milk and 2 cups (300 ml) of water on a low flame until
the volume was reduced to 1 cup. Besides this, they were advised to
consume warm water throughout the day and observe langhan as part
of the intervention.
Langhan: This was a modified dietary regimen. Patients were
allowed to consume ad libitum: rice, moong dal (decorticated
Vigna radiata), tur dal (decorticated Cajanus cajan), spinach, shepu
(Anethum graveolens L), drumstick (Moringa oleifera), parwar/
pointed gourd (Trichosanthes dioica Roxb), pumpkin (Cucurbita
pepo), and onion. They were allowed to use only salt, cumin seeds,
ginger, garlic, and asafoetida.
Pilot study: A pilot trial was carried out on six patients who
were not part of the main study, to finalize the amount of Sunthi
and Trikatu, to determine whether there were any side effects and
finalize the instructions to be given to patients. Acceptance of the
dose and reactions were monitored. Two doses - 4g and 6g of the
Sunthi and Trikatu were used. Six grams of the daily dose of each was
well tolerated, none of the patients experienced any side effects and
the degree of relief from pain was better with the 6g dose than with 4g.
Hence, the dose of 6 grams was finalized.
Data collection: A) Baseline data included family history,
prakriti, personal habits such as chewing tobacco/paan, smoking,
duration of disease in terms of years from the onset of disease, and
previous treatments underwent. Prakriti was assessed as per Ashtanga
Hridayam and was confirmed for each patient by a Senior Ayurvedic
Physician in the hospital.
B) Severity of morning stiffness, pain at rest and while moving,
digestive impairment, presence of fever, anorexia, and bowel habits
were recorded at baseline and the follow-up visits. Each symptom was
given a score as follows: 0 - no pain/ no symptom, 1 - for mild, 2 - for
moderate and 3 - for severe. The maximum possible score was 21.
Functionality: This was assessed using the disability index that
examines the difficulty in performing daily activities and a visual
analogue scale.
The HAQ-Disability Index (HAQ-DI)given by Bruce and Fries
was used to record the amount/level of difficulty experienced in
performing eight items/ activities [3], namely dressing and grooming,
arising, eating, walking, hygiene, reach, grip and common daily
activities. The level of difficulty experienced was scored as: ‘0’ - can
perform without any difficulty,‘1’ - with some difficulty, ‘2’ -with
much difficulty and ‘3’ - unable to do and need someone to help with
the task. The total disability index score was calculated as per Fries et
al.,[3].
Pain Faces Scale: The Pain Faces Scale, a visual analogue scale
developed by Wong et al., was used for self-assessment of the
intensity of pain [4]. The scale consists of six different faces to express
the degree of pain. The scores ranged from 1 - very happy, 2 - pains a
little bit, 3 - pains even more, 4 - pains much more, 5 - pains a lot, to
6 - hurts as much as you can imagine. Subjects were asked to choose
the face that best described how he/she was feeling.
Ritchie’s Articular Index (RAI) was used to assess joints of fingers,
wrist, elbow, shoulder, knee and ankle on the left and the right side as a single unit [5]. These joints were assessed for pain, swelling,
warmth, and limitation of motion.
Grip strength: Grip strength and time required to walk a specified
distance were measured at each weekly follow-up. This was measured
using the Grip-D dynamometer with 0.1 kg force accuracy. Each
patient was asked to stand straight with arms extended downwards.
He/she was asked to grip the handle and exert full force without letting
the hand touch any part of the body. Grip strength was measured for
both arms separately, to the nearest 0.1 kg force. The test was repeated
thrice for each arm and the average was calculated.
The time required to walk was used to determine whether there
was any improvement in the lower limbs. Patients were asked to walk
a distance of 110 feet (33.5 meters) at their normal pace and the time
required was recorded using a digital stopwatch (Race make) with an
accuracy of 1/100 seconds.
Dietary assessment: A 24-hour diet recall was done for the day
prior to the hospital visit. Dietary intake was recorded in terms of
household measures and wherever applicable, the number of food
items e.g., biscuits, chapatis were recorded. Household measures
were then converted to raw weights and intakes of energy, protein,
carbohydrate, fat, iron and calcium were calculated using the nutritive
value tables [6].
Anthropometric measurements: Height was measured using
a standardized, flexible non-stretchable, plasticized tape with 1mm
accuracy using standard techniques. Weight was measured using
a weighing balance (Kohinoor make) and recorded to the nearest
0.1 kg using standard techniques. Before every measurement, the
instrument was calibrated to zero. Three readings were taken and the
average of three readings was calculated. Body Mass Index (BMI) was
calculated and subjects were classified using the WHO standards for
Asians [7].
Data Analysis: Data was analyzed for only those subjects who
participated until Day 14 of the study (15 in Sunthi group and 17 in
Trikatu group). Data was analyzed using Graph pad instat and SPSS
version 17. Paired t-test was applied to determine whether there were
significant differences between pre- and post-intervention status.
Unpaired t-test was used to compare the Sunthi and Trikatu groups.
Pearson’s and Spearman’s chi-square test and correlation coefficients
were calculated to determine associations between different variables.
Results
Baseline Profile of subjects:
Age and BMI: Subjects’ ages varied from 24 years to 65 years
(Table 1), the mean age in the two groups being fairly similar. A little
more than one-third of the subjects (37.5%) were 40-49 years old
and 28.1% were 30 to 39 years of age. Thirteen of the 15 subjects in
the Sunthi group and 15 of the 17 subjects in the Trikatu group were
female. Mean BMI did not differ significantly between the two groups.
In the Sunthi group, 60% of the subjects (n= 9) had normal BMI
compared to only 46.8% (n=7) in the Trikatu group. In the Sunthi
group, 19.9% (n=3) were in different grades of obesity compared to
28% (n=9) in the Trikatu group. Eighteen percent of the subjects
chewed paan or tobacco, 36% had chewed supari and 27% smoked.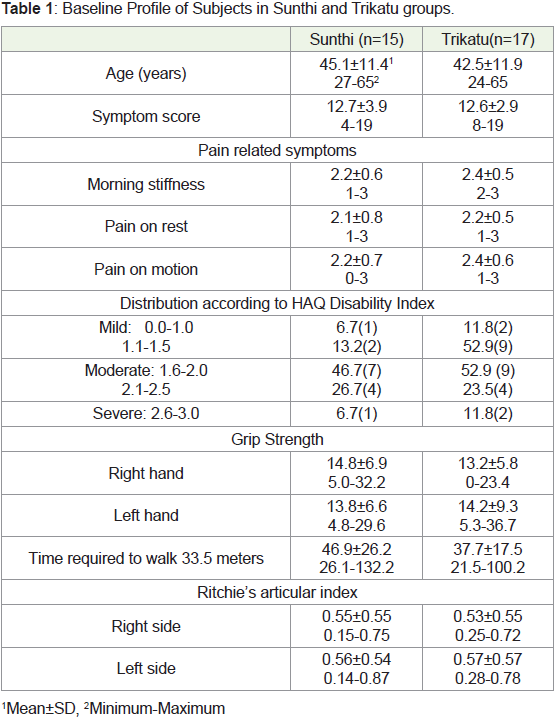
Prakriti: Vata prakriti was predominant 60% of the subjects
overall, with subdominant kapha or predominance of kapha followed
by vata, and only 18% of subjects had pitta predominant prakriti.
There was a significant difference between the two groups (χ2=30.693,
p=0.0001). In the Sunthi group, one third of the patients had kapha pitta
prakriti and 20% had vata -kapha and prakriti. In the Trikatu
group, 28.5% had vata-kapha prakriti and 32.1% had kapha-vata
prakriti.
Disease duration: Duration of disease varied from 1 month to
384 months, although the majority in both treatment groups (60.0%
in Sunthi group and 64.7% in Trikatu group) had suffered from the
disease for less than 2 years. In the Sunthi group, the maximum
duration was 96 months whereas, in the Trikatu group, the duration
was longer, 3 patients reported a duration of more than 97 months.
Almost all the subjects (90.6%, n=29) had been on allopathic
medication alone or along with Ayurvedic treatment. Only 9.3%
(n=3) were new cases seeking Ayurveda as the first line of treatment.
Family history: Eight subjects (25%) had a family history, and
for 87.5% of patients the mother had the same problem. None had a
father or paternal relative with RA or Amavata.
Symptoms: Mean total scores for symptoms did not differ
significantly between the two groups (Table 1). For the Pain Faces
Visual Analogue scale, 46.6% (n=7) in the Sunthi group and 47.0%
(n=8) in the Trikatu group marked ‘pains much more’. Eight patients
in all, six from the Sunthi group and two from the Trikatu group, marked ‘hurts as much as you can imagine’. These patients suffered so
much pain and joint stiffness that they were unable to perform their
daily activities, even if they were helped by other family members.
One-fourth reported having ‘considerable pain’ and needed help in
every activity.
Twenty four of the 32 patients (75%) had gastric upsets, with
37.5% experiencing problems frequently. Six patients (18.8%) had
fever frequently and 68.8% sometimes had elevated body temperature.
Functionality: Functional ability was compromised as the
majority (75%) of the subjects had a moderate disability and 9.1%
had a severe disability, although there was no significant difference
between the two groups. The mean grip strength for the left hand, as
well as right hand, did not differ between the two groups, although
women (right hand - 22.9±6.9kgf, left hand - 12.6±5.2 kgf) had less
grip strength than men (Right hand -30.7±5.8 kgf, left hand -11.5±4.4
kgf). The time required to walk did not differ significantly between the
two treatment groups. The time required for walking was significantly
and positively correlated with the disability index score (r=-0.489,
p=0.004).
Assessment of joints: There was no significant difference
between the two groups and between the left side and the right side,
respectively, in the number of joints affected as judged by mean RAI
values (Table 1).
Nutritional Status and Dietary Intakes: Most subjects (n=25,
78.1%) did not eat breakfast regularly, and 81.3% (n=26) ate dinner
late. Approximately two-fifths (46.9%) of the subjects had a habit of
drinking cold water. Two-thirds of the subjects (62.5%) consumed
stale foods, with 50% doing so regularly. Also, 62% (n=20) reported
that they had a low to moderate degree of anorexia-53.3% in the Sunthi
group and 76.4% in the Trikatu group. One subject suffered from
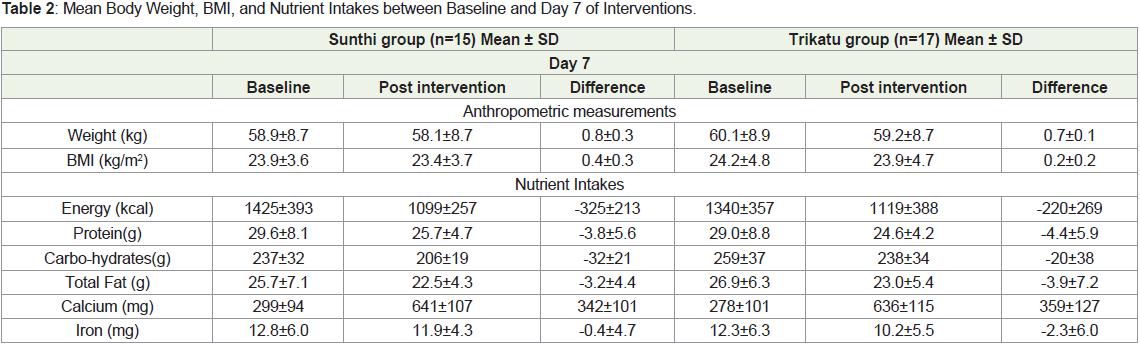
severe anorexia. Nutrient intakes calculated from the 24-hour diet
recall did not differ significantly between the two intervention groups
at baseline (Table 2). The majority of patients met more than 50% of
the recommended dietary allowances (RDA) for energy, protein, fat
and calcium. However, iron intakes particularly among women were
less than 50% of the RDA. Anorexia was significantly and negatively
correlated with total energy intakes (r=-0.456, p=0.015).
Effect of intervention- Day 7:
Nutrient Intakes: The modified diet along with consumption of the decoction of either Sunthi or Trikatu, resulted in a considerable
reduction in the intakes of energy, and carbohydrates with a small
decrease in the protein and fat intakes, while calcium intakes
increased in both groups. Iron intake did not decrease much in the
Sunthi group but reduced more in the Trikatu group (Table 2).
Body weight and BMI: Langhan resulted in a significant loss
in body weight in both groups Day 7 and Day 14 (Sunthi group:
t=8.56, p=0.0001; Trikatu group: t= 4.58, p=0.0003) (Table 2). Only
one patient in the Trikatu group gained 0.6 kg. BMI also reduced
significantly (Sunthi group: t=4.9, p=0.0002, Trikatu group: t= 4.374,
p=0.0005). The mean decrease in BMI was slightly more in the Sunthi
than the Trikatu group, although, the difference was not statistically
significant.
Symptoms: Symptom score reduced significantly (t=2.54,
p=0.01), more in the Sunthi group (t=8.569,p=0.0001) than in the
Trikatu group (t=2.840, p=0.01), (Table 3). Mean scores reduced
significantly- 1.0±0.4 for the Sunthi group (t=9.025, p=0.0001) and
0.7±0.4 (t=6.197, p=0.0001) for the Trikatu group. Patients reported a
significant reduction in morning stiffness after treatment, Sunthi being
more effective in reducing morning stiffness (t=2.196, p=0.035) (Table 3). Similarly, the score for pain on rest decreased (Sunthi group 1±0.5
(t=7.2, p=0.0001) compared to only 0.4±0.6 (t=3.1, p=0.0068) for the
Trikatu group. Reduction in scores for morning stiffness significantly
correlated with the score for pain on rest (r=0.563,p=0.045). In
both groups, the percentage of patients experiencing severe pain
on movement decreased to nil and the percentage of subjects
experiencing pain of mild intensity increased to 33.3%. The mean
reduction in scores for pain on movement was 0.7±0.7 for the Sunthi
group (t=4.036,p=0.001) and 0.7±0.8(t=3.4,p=0.003), for the Trikatu
group, with no significant difference between the two groups. The
number of patients experiencing GI upsets was also reduced.
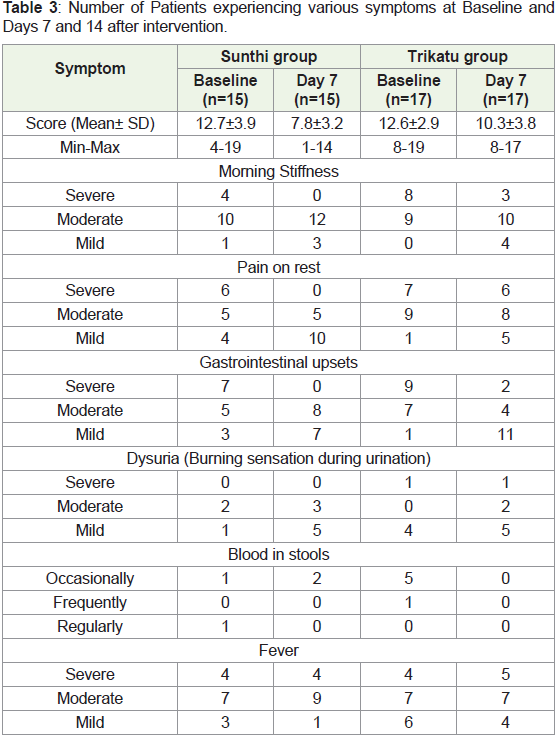
The number of patients who experienced burning sensation while
urinating was greater on Day 7 as compared to baseline, particularly
in the Trikatu group (t=2.7,p=0.01). In the Sunthi group, also the
number of patients experiencing burning sensation increased, but
this increase was not statistically significant.
The number of patients reporting the presence of blood in
stools decreased in both groups (Table 3), although the number of
patients suffering from fever, a sign of Amavata, did not change much. Anorexia was experienced at baseline by 53.3% of patients in
the Sunthi group, which reduced to 33.7% on Day 7 of intervention.
In the Trikatu group also, the percentage of patients reduced from
76.4% at baseline to 58.8% on Day 7.
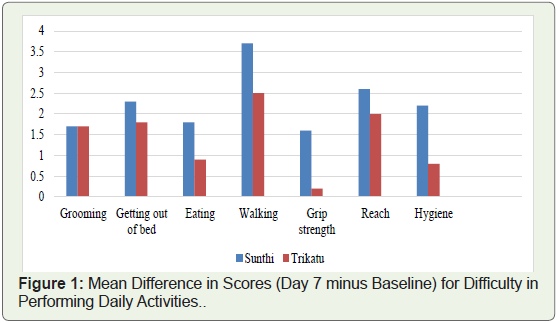
Functionality: The HAQ-DI scores between baseline and Day
7 showed a significant reduction in all components in the Sunthi
group whereas (Figure 1), in the Trikatu group, the reduction was
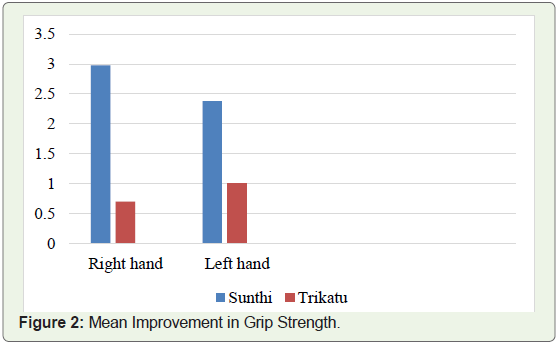
comparatively less. Grip strength increased with both treatments
(Figure 2), for both the right hand and left hand (scores- for right
hand, t=2.839, p=0.0085; for left hand, t=20.7, p=0.048).
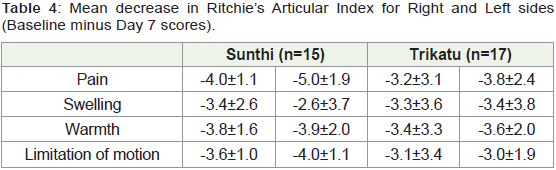
There was a considerable reduction in RAI on Day 7 for both
sides (Table 4), particularly in the reduction of scores for pain and
swelling. There was no significant difference between the Sunthi- and
Trikatu - treated groups.
Effect of Intervention - Day 14:
Only five patients in both groups reported for follow-up. There was a reduction in symptoms from Day 0, to Days 7 and 14 of
treatment, respectively in the mean scores for different symptoms,
functionality and disability index for these five patients were lower
and in the difference between these scores during follow up (Table 5 & 6 ). In the Sunthi group, the symptom scores decreased
progressively between baseline and Day 14 when the trial was
terminated. In contrast for the Trikatu group, a significant decrease
in the symptom score was seen only between Days 7 and 14. Dysuria
was an exception as it was experienced in both groups as reflected by
the increase in the score.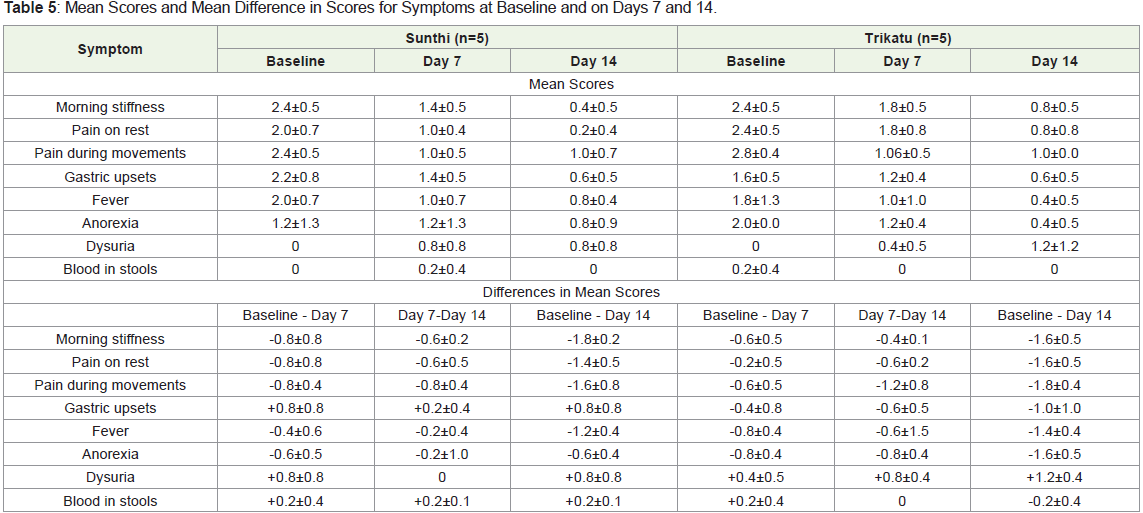
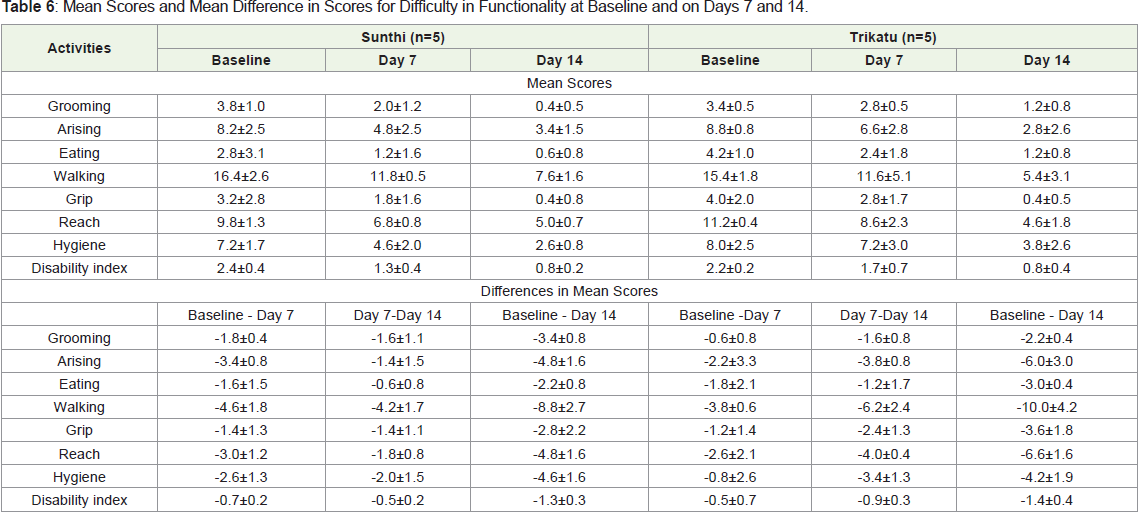
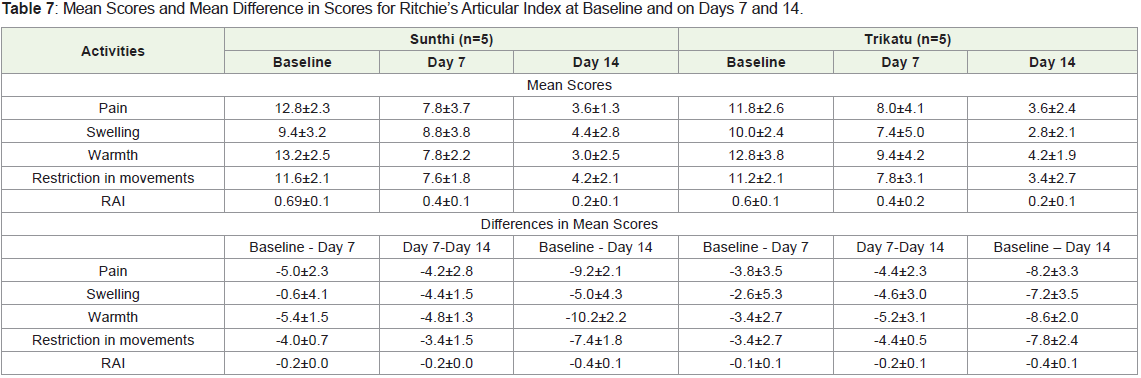
The functional ability scores of the patients improved as indicated
by the lower scores and the mean differences in scores on Days 7 and
14 as compared to the baseline scores (Table 7). On Day 14, there
was not much difference between the Sunthi and Trikatu groups.
The mean scores at the three time points and the mean differences in
scores for RAI between baseline, Days 7 and 14, respectively; indicated
that for all five patients in pain, swelling, warmth and limitation of
motion reduced.
Discussion
Treatment of RA and preventing its aggravation and the
consequent disability requires attention, as it affects approximately
0.92% of the adult population in India, with an annual increase of 20-
40 new cases per 100000 populations [8].
Amavata often considered to be equivalent to RA is attributed
to ama formation due to weakened agni i.e., digestive capacity, consumption of inappropriate diet and foods, as well as disequilibrium
in the three doshas (Vata, Kapha and Pitta), resulting in improperly
formed Anna rasa. This is considered as the initiating factor is vitiated
and propelled throughout the body and lodges in Sandhisthana
(joints) [1].
Ayurvedic literature indicates that Langhan and tikta-katu ahara
i.e., modified diet with hot and pungent potency,with use of aushadhi
dravyas, generally Sunthi and Trikatu help in treating Amavata [1].
Therefore, in the present study, we explored the effect of Langhan
with Sunthi or trikatu on patients with Amavata. Langhan i.e., fasting
or consumption of a light diet is considered the first line of treatment
in Ayurveda. Restriction or elimination of food breaks the vicious
cycle of improper digestion and ama production, contributes to the
digestion of already formed ama besides enhancing digestive and
metabolic capacities [1]. Charaka stated that consuming heavy, cold
and/or excess food, and impure diets contribute to Ama formation,
resulting in inflammation typically seen in Amavata/RA and the
obstructive processes that are said to occur in Amavata.
Fasting and reduced caloric intake have been associated with
improved outcomes for metabolic, autoimmune and inflammatory
diseases including RA [9]. Inflammation is a crucial event in the
complex chain of events involved in the development of RA.
Inflammatory cytokines stimulate fibroblasts and chondrocytes,
resulting in inflammation. And there is the degradation of
peptidoglycans and cartilage [10]. Anti-inflammatory medications in
modern medicine help to reduce pain and stiffness, however, with
long-term use; they can have adverse effects on the bone marrow,
kidneys and liver. Inflammatory arthritis presents with dysregulation
of cell metabolism and dysfunctional lymphocytes. Alterations in
CD4 T cell metabolism, particularly in glucose metabolism could
increase the severity of joint inflammation [10]. Fasting alters cellular
metabolic pathways, immune function, erythrocyte sedimentation
rate and expression of pro-inflammatory cytokines, IL-6, CRP [9]. A
subtotal fast for seven days resulted in decreased CD4+ lymphocyte
number and function, Relief from pain and reduced disease activity
score. However, there are indications that when fasting ceases,
symptoms reappear or flare-up.
In a single-blind study of 53 patients with RA; participants in the
experimental group fasted for 7-10 days and then followed a vegan
diet for 3.5 months (doctors were blinded about the allocation to
fasting and control groups). After this, milk and dairy products were
introduced singly but were withdrawn if symptoms were aggravated.
Thirteen months of this regimen brought about significant
improvement [9]. Other benefits include lower duration of morning
stiffness, articular index, increase in hemoglobin and reduced release
of lysozyme associated with inflammation and joint destruction,
leukotriene B4 that is pro-inflammatory and involved in activation of
neutrophils that mediate tissue damage [11,12].
Recently, Rose and Strombom reported that vegan or vegetarian
diets improved the leukocyte count [13], levels of rheumatoid factor,
IgM, C3 and C4 and symptoms. Jordan and co-workers observed that
fasting decreased the size of the circulating monocyte pool [14], a
favorable effect as monocytes produce pro-inflammatory cytokines.
Metabolic activity and gene expression patterns were modified. Also, short-term and intermittent fasting did not compromise tissue
regeneration.
From the Ayurvedic perspective, further production of Ama
needs to be controlled, generally using foods and/or drugs having
katu, tikta rasa and deepana properties. Among the food items that
have this capacity with was Sunthi/ginger, turmeric, garlic, pepper.
All three are well known for their anti-inflammatory effects. Ginger
provided relief from pain and swelling with no side effects when it was
consumed over a long duration from 3 months to as long as 2.5 years
[15]. Prakash and Dwivedi reported that Sunthi reduced stiffness of
joints, anorexia, heaviness and changes in taste [16].
In an animal model, Funk et al., observed that a crude ginger
extract prevented both joint inflammation and bone destruction
[17]. The crude extract that contained both polar compounds and
essential oils has more therapeutic potency than did gingerol and its
derivatives. Shrivastava and coworkers reported a reduction of pain
upon treatment with ginger powder [15]. Phan et al., demonstrated
that in human synoviocytes, the ginger extract significantly inhibited
cytokine expression [18].
In the present study, we demonstrated the beneficial effects of
ginger and Trikatu for their ability to mitigate the symptoms. Trikatu
possessed immunomodulatory, and anti-inflammatory potential at a
dose <1 g/day, and was found to be safe to use [19]. Active principles
in Trikatu like piperine, 6-shogaol and 6-gingerol have an antiinflammatory
effect in RA and acute gouty arthritis [19]. Studies
on paw edema in animal models have shown that Trikatu reduced
edema, levels of circulating immune complexes and the inflammatory
mediators TNF - α and Interleukin-1β [20,21]. Piperine in pepper
and long pepper in Trikatu has anti-inflammatory activity.
However, a common side effect of Trikatu is heartburn and
acidity. In the present study, we found that more patients given
Trikatu experienced side effects than those who were given Sunthi. A
lower number of patients experiencing side effects with ginger could
be attributed to the analgesic effect of gingerol and gingerdione, in
addition to their anti-inflammatory effect. In a rat model of human
RA, a blend of turmeric and ginger was effective against the extraarticular
complications of RA [22].
Diets that are typically calorically rich, particularly containing
processed foods that are low in micronutrients, ‘phytobioactives’
and fiber can result in chronic low-grade inflammation and increase
the risk of chronic diseases. Nutrients and dietary constituents can
modulate immune-metabolic homeostasis [23]. Sunthi, milk, pippali/
long pepper and foods like mung gruel that were used in the present
study, have been recommended for use in RA. Consumption of stale
foods, irregular meals and/or long gaps between consecutive meals
is considered to increase susceptibility to ama formation. Ayurveda
recommends the inclusion of certain food items such as barley
(yava), horsegram (kulith/kulatha) sama millet (shyamaka), red rice
(raktashali), drumstick, bitter gourd, brinjal, pointed gourd among
vegetables, consumption of lukewarm water(ushnajala), and to avoid
consumption of curd, milk, fish, jaggery and pishtanna i.e., foods
made out of flour [1].
In the present study, our patients were allowed to consume ad
libitum - rice, mung dal or tur dal; among vegetables, spinach, shepu (Anethum graveolens) drumstick, parwar/pointed gourd, pumpkin
and onion, but no other vegetables. They were allowed to add salt,
jeera (Cuminum cyminum), ginger, garlic and asafoetida to flavor the
preparations but to try and avoid other foods and spices/condiments.
This restricted diet along with the use of decoctions made with
either ginger/Sunthi or Trikatu was beneficial. Khanna, Jaiswal and
Gupta reported that subtotal fasting with limited consumption of
carbohydrates [24], vegetable juices, and limited vitamin and mineral
supplements reduced the CD4+ number and lymphocyte activation.
There was transient immunosuppression that contributed to the
suppression of RA. Intake of vegetable broth, juice and controlled
energy intake was associated with a decrease in swollen and tender
joints, pain, erythrocyte sedimentation rate and CRP levels. Also,
vegan diets have been shown to be clinically beneficial in terms of
decreased immune reactivity to certain food antigens in the diet and
allergenic foods can increase inflammatory mediators like TNF-α and
interleukin-1 [14,20,21,25].
Patients with RA generally have gastrointestinal problems such
as bloating, postprandial fullness, nausea, epigastric pain, burning,
belching, constipation or diarrhoea and early satiety [26]. In our
study, before the intervention, 75% of the participants experienced
varying degrees of gastric problems, with 46.8% having them
frequently. We observed that the use of Sunthi particularly reduced
GI problems such as GI upsets, burning sensation and blood in stools.
Nanda et al., reported that intestinal mobility was strengthened
in 111 patients given 3g of Sunthi powder thrice daily with warm
water for one month [27]. In a randomized, double-blind controlled
trial with 11 dyspeptic patients, Hu et al., [28] observed that ginger
stimulated gastric emptying and antral contractions, although fundus
dimensions, serum concentrations of GLP-1, motilin and ghrelin
were not affected.
In the present study, morning stiffness, pain on rest and during
motion, fever and anorexia were reduced. At the end of the study,
the number of patients who had severe pain on movement reduced
to nil, while there was an increase in the percentage that experienced
mild pain. This may be attributed to the digestion of Ama by Sunthi/
Trikatu and mobilization of vata from the joints. However, dysuria
and digestive upsets increased after treatment, particularly in the
Trikatu group. This may be attributed to the ‘hot’ potency of Trikatu.
As per Ayurveda, Sunthi has better Vata pacifying action and can be
taken for a longer duration.
Diet also influences gut microflora. Recently,an in vitro simulated
digestion and fermentation model, showed that ginger extract
had a prebiotic effect, with the growth of beneficial organisms
such as Bifidobacterium and Enterococcus. Ginger, black pepper
and pipali (Piper longum) all increased the relative abundance
of Bifidobacteriaceae. Ginger was observed to strongly select for
Coriobacteriaceae that are involved in isoflavone bio-transformation,
bile acid conversion, and generation of cholesterol-derived
compounds, while black pepper and pipali (the latter having a greater
impact) induced Bacteroidaceae, modulated the relative abundance
of taxa that produce butyrate and propionate taxa, and reduced the
relative numbers of pathogenic and opportunistic organisms. The
authors attributed these effects to the diverse glycans present in these
spices that serve as substrates for the microflora [29].
These studies support the use of both Trikatu and Sunthi in
Ayurveda for improving digestive function. Trikatu is often used
to treat Agnimandya/ decreased digestive ability and, ginger is said
to strengthen intestinal motility [30]. In our study, the number of
patients experiencing digestive disturbances/upsets decreased after
treatment. However, Trikatu consumption resulted in patients
experiencing more severe symptoms than those consuming Sunthi.
Gogate stated that Trikatu can cause stomach ache, abdominal
cramping and increase stool frequency [30]. In the present study, none
of the patients from the Trikatu group had severe digestive problems
at baseline, however on Day 7, two patients reported having severe
gastric upsets, that may be attributed to ‘ushna veerya’ of Trikatu.
Fever is considered to be an important sign of amavata because
the ama blocks perspiration channels leading to elevation of body
temperature, which is considered to be a defence mechanism of
digesting ama. After treatment, the percentage of patients having
fever reduced, which may be attributed to a reduction of ama in the
body. Also, the percentage of patients experiencing anorexia reduced,
with both Sunthi and Trikatu being equally effective.
The HAQ-DI scores were considerably lower after the
intervention. The Sunthi group showed a significant reduction in
all indicators i.e., grooming, arising, eating, walking, grip, reach and
hygiene-related activities whereas, in the Trikatu group, significant
improvement was observed for only three activities- grooming, arising
and reach. Mishra and Pandya in their review of various treatments
reported that Shunthi kwath used alone or in combination with
castor oil showed significant beneficial effects on subjective criteria
like Sandhishoola (joint pain), Sandhishotha (swelling of joints),
Sandhigraha (stiffness), Sparshasahatva (extreme tenderness in the
afflicted joints) as well as in objective criteria such as improvement
in handgrip [31], walking time and foot pressure. The modified
dietary regime used in the present study may also have contributed to
improvement in functionality.
Sunthi is generally used more often than Trikatu in all formulations
for Amavata. The present study also showed that Sunthi was more
effective and was accompanied by fewer side effects than was Trikatu.
Trikatu was tested in the present study because conceptually it was
expected that it would have an effect sooner than would Sunthi.
However, with Trikatu, the benefits were seen only between Days 7
and 14, whereas Sunthi showed beneficial effects by Day 7 itself. This
suggests that there may be a time lag before Trikatu exerts its effects
and/or the mechanism(s) of action of Sunthi and Trikatu may differ.
In Trikatu, piperine is the bioactive substance in both pepper and long
pepper.
In conclusion, the results of the present study indicated the
effectiveness of Sunthi alone or in combination with pepper and long
pepper in Trikatu. However, a major limitation of the study was the
small number of subjects and the high number of dropouts, probably
because of the restrictive diet. Subjects who dropped out were asked
why they dropped out when they presented to the treating Ayurveda
Physician after the study was completed. They all stated that they were
not given any medications or Panchakarma treatment in contrast
to other patients who had received treatment earlier at the hospital
and on whose recommendation, they had sought treatment. They also felt that the diet was too challenging to adhere to, especially
because wheat was eliminated. It must be pointed out that all the
study participants were habitual wheat eaters who missed consuming
chapati at both meals. Thus, recommendations for inclusion of the
foods advised in the present study need to be considered in modern
dietetic practice, the limited food choices may limit adherence
to such diets, particularly since RA is a chronic health problem.
It would be worthwhile to determine how to modify the diets and
make them more consumer-friendly, particularly in the present-day
context of easy availability of processed foods. Integrating Ayurveda
with a modern system of medicine and modern dietetics for better
management of RA/Amavata would be worthwhile as there are
limitations to treatment with modern medicine.
Acknowledgement
We would like to extend our sincere gratitude to the authorities
at Seth Tarachand Hospital, Pune for permitting us to conduct this
study and their assistance in during the entire process. We would
also like to thank Ms. Aditi Goyal, Nutritionist, MRC-KHS for her
assistance during the editing of this paper.
References
Citation
Deo K, Pendse N, Udipi SA. Management of Amavata/Rheumatoid Arthritis with Langhan (Fasting), Sunthi (dried ginger) and Trikatu - an Ayurvedic Polyherbal Formulation. Indian J Nutri. 2022;9(1): 248.