Research Article
Correlates of Vitamin D Status among Adults in Western India
Muley A1* and Iyer U2
1Symbiosis Institute of Health Sciences, Symbiosis International (Deemed University), Pune, India
2Department of Foods & Nutrition, Faculty of Family & Community Sciences, The Maharaja Sayajirao University of Baroda,
Vadodara, India.
*Corresponding author: Muley A, Symbiosis Institute of Health Sciences, Symbiosis International (Deemed University), Pune,
India; Email: arti@sihspune.org
Article Information: Submission: 25/11/2021; Accepted: 27/12/2021; Published: 30/12/2021
Copyright: © 2021 Muley A, et al. This is an open access article distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Vitamin D deficiency (VDD) prevalence has been addressed in many studies covering all continents and having enormous public health consequences.
Though VDD is highly prevalent in India, there is paucity of data about it among population in Western regions which receive ample sunlight round the year.
Hence this cross-sectional research attempted to investigate the vitamin D levels and the probable determinants in apparently healthy Indians from urban
Vadodara in Gujarat state. About 129 subjects (30-60 years of age) from five zones of Vadodara were enrolled through snow-ball effect. Along with informed
consent, demographic data and risk factors of VDD were gathered using a semi-structured questionnaire. Fasting blood samples of the participants were
collected, and the serum was used to analyze vitamin D by ELISA. Serum 25(OH) D levels of more than equal to 75 nmol/L i.e. ≥30 ng/mL were considered
sufficient while levels less than 75 nmol/L were reported as insufficiency or deficiency. The data was subjected to appropriate statistical analysis using
SPSS v20. The results revealed that almost 88% of the subjects had VDD, with significant high prevalence among females (p<0.01). Percent body-fat, LDLcholesterol
and thyroid hormones- TSH & T3 showed significant negative correlation with the vitamin D levels, while hemoglobin was positively correlated.
These along with age emerged as significant predictors for the vitamin D status in the multivariate regression model. Thus it was concluded that VDD was
high among the population. So, there is a need to address the predictors for low vitamin D status by adopting a healthy dietary pattern and an active lifestyle
with adequate exposure to sunlight.
Keywords
Vitamin D; Risk factors; Determinants; Apparently healthy adults; Gujarat; India
Introduction
Vitamins are organic compounds that are required in minute
quantities to sustain life. Two compounds of vitamin D, namely-
Ergocalciferol and cholecalciferol are important in living creatures.
The prominent breakdown product of vitamin D in the body is
25-hydroxyvitamin D (written as 25 (OH)D), as it takes into account
both the vitamin D obtained from cutaneous synthesis as well as the
dietary sources. The of 25(OH)D concentration in serum is believed
to be an accurate index of one’s vitamin D levels (Holick, 2004) [1
].
VDD has assumed pandemic proportions globally with the prevalence
ranges between 31-98% based on this index (Wacker & Holick, 2013)
[2
]. Due to availability of good amount of sunlight, it is presumed
that those residing in tropical countries may be little safer against
developing VDD. However, data available so far proves it wrong. In a research among 3,262 adult subjects residing in Beijing and Shanghai,
it was observed that the mean 25(OH)D level was about 40 nmol/l,
and 69% and 24% of the subjects were having VDD and insufficiency
respectively (Lu et al., 2009) [3
]. Similarly in Korean population also
VDD defined as values less than 20 ng/mL, was reported in 56.9%
of the subjects (47.3% males and 64.5% females). Only about 20% of
male the population had levels greater than 30 ng/mL (Choi et al.,
2011) [4
].
India is also a tropical country. Hence maybe it was never thought
that VDD would be prevalent here. However about 90% of evidently
healthy people in north India (Delhi) showed significant prevalence of
hypovitaminosis D among themselves, when a sensitive and specific
assay was used to measure serum 25(OH)D levels (Goswami et al.,
2000) [5
]. In a survey among hospital staff the mean serum levels were 30 nmol/L (Arya et al., 2004) [6
], while among pregnant women
it was 35 nmol/L [7
] and 36 nmol/L for the post-menopausal women
in India [8
]. In a cross sectional study among 444 subjects belonging
to higher socioeconomic population of different age groups and
gender in Ahmedabad City, Gujarat majority of the subjects (46.4%)
were severely deficient [8,9] also in their previous study reported
sub-optimal serum 25(OH)D quantity among adult population with
significantly low amounts among women as compared to males
(11.49±6.9 vs 17.24±3.5, p<0.001). A study from north India among
healthy individuals above the age of 50 years VDD was present in
91.2% of the population while 6.8% reported insufficiency [10
].
The major reasons attributed to VDD in India are duskier skin
complexion, less exposure to sunlight, predominantly vegetable
oriented dietary pattern and scarcity of vitamin D fortified foods in
the market [11
]. Thus though a fair body of literature on prevalence
of VDD for Indian population exists, there is a scarcity of data from
western states of India; especially on risk factors and determinants
of vitamin D status among apparently healthy population in spite
of sunlight. Thus to challenge the hypothesis that availability of
ample sunshine decreases the risk of VDD, the current research was
conducted in Vadodara city. It is the eighteenth biggest city in India
and the third largest of the state. Its location is 22.30°N 73.19°E in
central Gujarat and is blessed with sunshine almost all long the year
because of its strategic location. An attempt was made to determine
the factors for poor vitamin D status among the participants.
Materials and Methods
The present research is a cross-sectional study carried out among
apparently healthy individuals residing in city of Vadodara in Gujarat
state, western India.
Selection of participants:
For the enrolment of participants living in different localities of
the city, the city was divided into five zones- north, south, central,
west & east. Through snowball effect, 129 participants (twenty-six
each from north, south, east and west zone and twenty-five from the
central zone) were enrolled (Figure 1).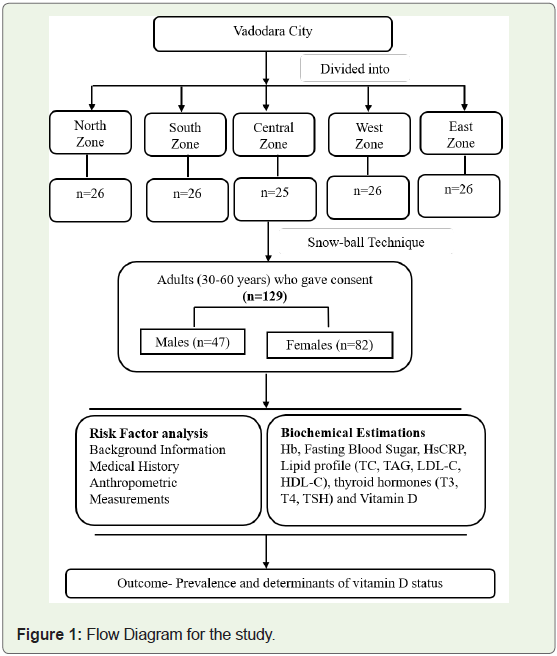
Inclusion-exclusion criteria:
The inclusion criterion was subjects should be in the age group
30-65 years; they should be residents of the city and give a positive
consent to participate in the study and for the blood estimations as
well. Pregnant women and lactating mothers and those suffering
from diabetes mellitus were not included in the study along with
those taking vitamin D supplements present and past six months.Ethical approval:
Ethical approval was obtained from the Institute’s Ethic
Committee. Informed written consent was obtained from all the
participants in English as well as local language (Gujarati).Data collection:
Information pertaining to social and demographic background,
health information was collected using a questionnaire which was
pilot tested before use in the study. Body measurements like weight,
height, waist circumference and hip circumference were noted for all the subjects using standard tools and procedures. Weight
was recorded by a standardized electronic bathroom scale and
height by non stretchable tape. The waist and hip circumference
measurements were recorded as per the standard definitions and
protocols [12,13
]. Percentage body fat was calculated using the
Omron body fat monitor (Model HBF-306). Researcher was trained
to take all the measurements. Standard formula was used to compute
BMI. Blood pressure was measured by clinically validated digital BP
meter (Omron HEM-7203 model). An average of the three recorded
readings was considered.The participants were asked to observe an over-night fast (12
hours post dinner). Blood samples were collected by a certified
technician for the biochemical profile. CLIA technique using kit
procured from Simens-ADVIA Centaur was used to estimate 25(OH)
D for vitamin D status. The serum level of 25(OH)D gives a correct
picture of combined values obtained from sunlight exposure and
intake through food and hence considered as a ‘gold standard’ for
the present study also [14
]. The definition given by Lips (2001) was
used to classify the subjects based on their vitamin D status. Lipid
profile (total cholesterol, triglycerides, low density lipoprotein and
high density lipoprotein), was estimated using Olympus AU2700
and Advia 1800 and the detection technology was by Photometry.
Haemoglobin was estimated by cyanmethemoglobin method in
autoanalyser, HsCRP by Nephelometry and fasting blood glucose
using GOD/POD method by enzymatic kit from Ecoline. Detection
Technology used for the estimation of TSH was ultrasensitive
sandwich chemiluminescent immuno assay by Advia centaur CP and
XP systems. These biochemical analyses were carried out by a private
laboratory certified by ISO 9001:2008 and NABL (India).
Statistics:
Data entry was done in Excel; checked and verified by the
investigator. Statistical analysis was done using SPSS v20. p value
of <0.05 was considered for significance. Chi square values were
computed for checking the significance for categorical variables.
Pearson ‘r’ value was calculated to study the correlations for vitamin
D status and risk factors. To identify the predicators of serum vitamin
D status a stepwise multivariate analysis (Linear regression) was
computed.Results
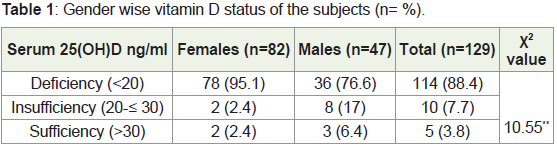
This study reports the results on 129 participants. A part of
the results are published elsewhere. Mean serum vitamin D for the
enrolled participants was observed to be 13.7 ng/mL, which is much
lower than the recommended optimum level of >30 ng/mL [15
]. As
seen from Table 1 almost 88% of the subjects were vitamin D deficient
and only 4% were in the sufficiency range with levels >30 ng/mL. The
deficiency was significantly higher among females as compared to
male subjects.
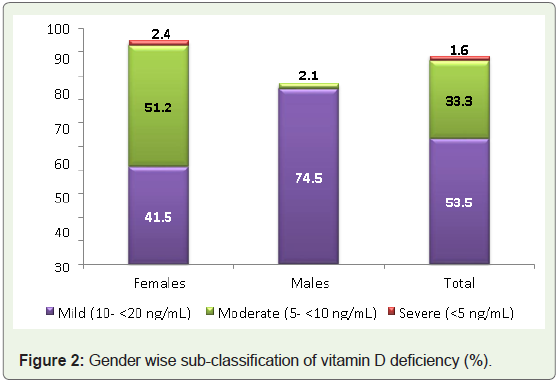
The vitamin D deficient subjects were further classified into subcategory
of mild, moderate and severe deficiency. As can be seen from
Figure 2, about 53.5% subjects were falling under mild category with
higher number of males (74.5%) as compared to females (41.5%),
while nearly half (51.2%) of the deficient female population showed
moderate vitamin D deficiency. It was heartening to see that only
two of the females (2.4%) had severe deficiency i.e,, levels <5 ng/mL.
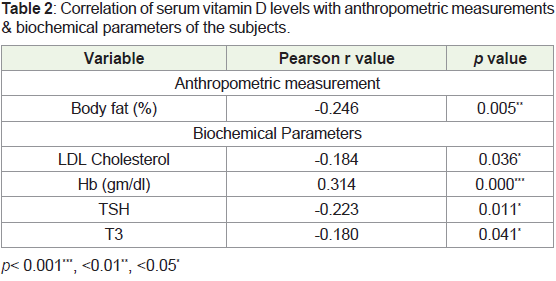
The correlation of various parameters with serum vitamin D levels
revealed that among the anthropometric measurements, percent body
fat was negatively significantly correlated with the subjects’ vitamin D
status. While for biochemical parameters LDL cholesterol and thyroid
hormones- TSH & T3 had a significant negative correlation, while
hemoglobin showed to be positively significantly correlated (Table 2).
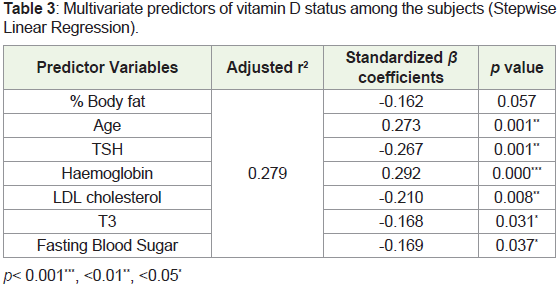
Considering serum vitamin D levels as the dependent variable
in the multivariate analysis (Table 3), showed that the model that
explained maximum amount of variation (27.9%) consisted of seven
variables: % body fat, age, TSH, hemoglobin, LDL cholesterol, T3 and
FBS; with six predictors being statistically significant except percent
body fat which just missed the significance.
Discussion
Deficiency of vitamin D is prevalent in countries which are
‘sunshine deficient’ as well as ‘sunshine sufficient’. It is considered
a public health concern in country like India too [16
]. Thus this
research attempted not only to study the vitamin D deficiency levels
but also to recognize the determinants for poor 25(OH) D status. In
the present study it was observed that almost 88% of the participants
had vitamin D deficiency, with significantly among females. These
results are similar to studies reported elsewhere. A cross sectional
study in an existing Malay cohort in Kuala Lumpur reported that
women possesed significantly poor vitamin D status compared to
men (36.2 against 56.2 nmol/L respectively). About 41% of men and
87% women had levels <50 nmol/L (p<0.001) [17,18] reported that
about 25.2% were vitamin D deficient and 36.2% were insufficient
among 365 participants, enrolled clinics in the state of Kuwait.
Females and participants of 60 years and above showed significant
frequency of being vitamin d deficient. Similar results have been
reported by Indian authors also. A study carried out in Kashmir
valley among 150 healthy volunteers, aged 18-40 years observed
83% as vitamin D deficient, with females having significantly higher
prevalence compared to males (94.4 and 76.6%, p<0.001) [19]. The
possible reasons contributing to this gender difference may be that
Indian women especially the homemakers and those who work from
home; spend a big amount of day time doing indoor household work, or home employment like taking coaching classes, running a beauty parlor, tailoring activities, and restricts them to sunlight exposure.
The clothing style of females, such as wearing long sleeves salwar kameez,
sari, or using hand gloves or sun-coat and covering the face
with dupatta while going out reduces the total body area exposed to
sunlight and thus reducing vitamin D production beneath the skin.
To see the extent of deficiency among the population the subjects
were further categorized in various stages of VDD as proposed
by [20
]. The segregation showed that majority were in mild to
moderate category and only 1.6% of the population had levels <5ng/
mL comprising the severe category, also reported similar analysis,
wherein the reported prevalence of severe deficiency (27.9% and
27.5% respectively) was more in comparison to the present study. In
the present study age emerged as significant determinant for vitamin
D status. As age advanced the levels too increased [21
], also reported
a significant age related increase of vitamin D levels among healthy
Omanis of age 18 to 55 years. Females, as compared to males,
possessed significantly less values of vitamin D (28.2 against 36.8
nmol/L, p<0.0001). The overall prevalence of VDD in the population
was about 88%. In the KNHANES study also poor vitamin D status
was most prevalent in the age of 20-29, with 65% of males and 80%
females being deficient as compared to the older age groups. A study
conducted among 77 healthy women, aged 19 to 66 years, working in
nursing homes in Japan also reported low serum levels among the
young age group [22
].
The correlations and multivariate analysis revealed that age and
hemoglobin levels had positive associations with vitamin D levels
while percent body fat, LDL-cholesterol, thyroid hormones and
serum glucose emerged as negative determinants for poor vitamin
D status. A study among healthy Omani population also reported,
poor vitamin D status to be associated moderately with BMI and
prominently with indices of abdominal obesity. Waist-to-Hip ratio
emerged as the main predictor of serum 25(OH)D levels among the
participants also reported that being a women (Odds Ratio= 8.68;
95% CI: 5.1-14.8) and having abdominal obesity defined by high
WC (OR 2.57; 95% CI: 1.51-4.39) had significantly higher odds for
insufficient Vitamin D status. [23] reported some very favorable
results in his study on 171 healthy Korean adults who had no cardiac
disease history. Vitamin D levels were positively correlated with age
(p<0.05), HDL-C (p<0.05), and the inflammatory marker adiponectin
(p<0.05) levels. These results clearly emphasize the requirement of
regular exercise to maintain desired anthropometry measurements
and biochemical parameters, more so if one is a woman.
Conclusion
Thus from this cross sectional study it can be concluded that
VDD was highly present in the apparently healthy adult population
with women being a vulnerable gender. All the significantly emerged
variables can ultimately be managed and maintained by adopting a
healthy dietary pattern and an active lifestyle with adequate exposure
to sunlight which needs due attention. The results though cannot be
generalized to entire nation as our participants belonged only to the
urban setting of a city in western India. However, as per our review,
this is the only study of its kind to map the prevalence of VDD in
Vadodara and investigate the relationship of vitamin D levels with
clinical conditions. This study will also add to the exciting literature that reports a high prevalence of VDD in India, thus emphasizing the
need for a nationalized vitamin D supplementation and fortification
program.
Acknowledgment
The authors would like to acknowledge University Grants
Commission (UGC), New Delhi for supporting the study in form of
research fellowship to corresponding author.
The paper was presented in the Asian Science Congress at Bali,
Indonesia from August 4-7, 2019. The abstract is published in Annals
of Nutrition and Metabolism, 75 (suppl-3): 194.
References
Citation
Muley A, Iyer U. Correlates of Vitamin D Status among Adults in Western India. Indian J Nutri. 2021;8(3): 244.