Review Article
Role of Vitamin B12 in Autistic Spectrum and Attention Deficit Hyperactivity Disorders: A Scoping Review
Rawat S1*, Nagpal J and Jain T2
1Sitaram Bhartia Institute of Science and Research, B-16, Qutab Institutional Area, New Delhi, India
2Amity Institute of Food Technology, Amity University, Amity Road, Sector-125 Noida-201301, Uttar Pradesh, India
*Corresponding author: Rawat S, Department of Research and Clinical Epidemiology, Sitaram Bhartia Institute of Science and
Research, B-16, Qutab Institutional Area, New Delhi, India Email: swapnil.rawat@gmail.com
Article Information: Submission: 09/11/2021; Accepted: 10/12/2021; Published: 13/12/2021
Copyright: © 2021 Rawat S, et al. This is an open access article distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Vitamin B12 plays a vital role in normal brain functioning. Its deficiency is associated with developmental delays, irritability, and failure to thrive in children.
Several studies have evaluated the possibility of B-12 deficiency leading to ASD/ADHD with inconsistent results. This review summates the available literature
on B12 deficiency/supplementation and ASD/ADHD in children. The literature search was conducted in Medline and Extended Medline using the following
search words (Vitamin B12 or Cobalamin or Methylcobalamin or Cyanocobalamin) and (Autism, Autistic spectrum disorder or attention deficit hyperactivity
disorder or ASD or ADHD). Total of sixteen studies were retrieved of which four were clinical trials. Most of the observational studies report an association
between B-12 deficiency and Autism. Studies on ADHD are fewer, and the association is weaker. Intervention studies were only available for ASD. Three of
these reported improvement in biochemical and/or clinical behavior ratings for ASD children while one study did not show any improvement in either. There
is observational data documenting the relationship between B-12 dfefficiency and ASD. Studies on ADHD are fewer and less conclusive. Intervention studies
using B-12 in ASD children document biochemical improvement. There is paucity of trial literature on the clinical impact of B-12 supplementation in ASD
especially in terms of behavior ratings. Further work should be urgently considered to address these lacunae.
Keywords
Vitamin B12; Autism; Attention Deficit Hyperactivity Disorder
Introduction
Vitamin B12 is a water-soluble vitamin required for the
development and initial myelination of central nervous system and
normal functioning of the brain. Vitamin B12 (B12) is an essential
cofactor for two enzymes involved in one‐carbon metabolism:
methylmalonyl CoA mutase (reduced function of this enzyme
results in increased serum methylmalonyl acid (MMA) levels) and
methionine synthetase (this enzyme catalyzes the remethylmation
of homocysteine to methionine). A serum B12 level below the
normal expected range may indicate B12 deficiency [1]. Levels of
B12 along with methylmalonic acid (MMA) and homocysteine are
usually measured to detect the B12 deficiency [2]. Well-documented
adult consequences of B12 deficiency include pernicious anemia,
megaloblastic anemia, peripheral neuropathy neuropsychiatric syndromes and subacute combined degeneration of spinal cord
[2,3,4]. Vitamin B12 (cobalamin) deficiency has been previously
thought to be rare in children; however, recent studies suggest that the
condition is more common than previously recognized [5]. Vitamin
B12 deficiency in children is known to present with nonspecific
manifestations, such as developmental delay, irritability, weakness,
and failure to thrive. B-12 deficiency is becoming increasingly
critical in India with the high prevalence of deficiency and the
rising prevalence of vegetarianism. Recently many researchers have
attempted to evaluate the potential role of the deficiency in childhood
neurological syndromes like Autistic spectrum and Attention Deficit
Hyperactivity Disorder. The current review seeks to summate the
current evidence in this regard.
Metabolism:
Vitamin B12 is found primarily in foods of animal origin. When consumed, vitamin B12 is released from food proteins in
the stomach and binds to R-binder proteins, made in the saliva and
stomach. After exposure to pancreatic proteases, vitamin B12
is released from the R proteins in the small intestine and forms
a complex with intrinsic factor, produced in gastric parietal cells.
The intrinsic factor-vitamin B12 complex is taken up in the terminal
ileum, after recognition by specific ileal receptors. The complex
dissociates in the enterocyte, and the free vitamin enters the portal
circulation bound to transcobalamin II, which transports vitamin
B12 to tissues. Vitamin B12 is secreted in bile and reabsorbed in the
ileum, conserving B12 in individuals with normal absorption [5].
Although the adult recommended dietary allowance for vitamin B12
is 2.4 μg/d, an adult stores about 2 to 3 mg (primarily in the liver) [6].Dosage and mode of administration:
Table 1 lists the current Recommended Dietary Allowances
(RDA) by National Institute of Nutrition, 2020 for vitamin B12 across
all age groups [7].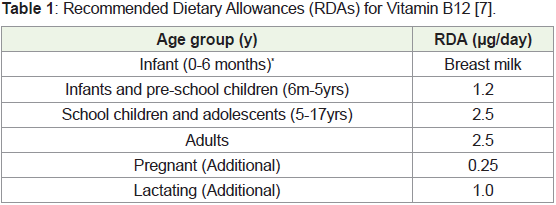
Safety profile:
The Institute of Medicine (IOM) did not establish a Upper Limit
for vitamin B12 because of its low potential for toxicity. In Dietary
Reference Intakes, the IOM states that “no adverse effects have been
associated with excess vitamin B12 intake from food and supplements
in healthy individuals” [6].Therapeutic dosages:
In patients with vitaminB12 deficiency, two oral regimens have
been shown to achieve neurologic and hematologic response in the
short term. Effective dosages were 2,000 μg daily or 1,000 μg daily for
10 days, then weekly and monthly [8].Contraindications and cautions [9]:
Vitamin B12 is contraindicated in known hypersensitivity to
the vitamin or to cobalt. Patients who have early Leber’s disease
develop severe and swift optic atrophy on treatment with vitamin
B12. Hypokalemia and sudden death are reported when severe
megaloblastic anemia is treated aggressively. Indiscriminate
administration of vitamin B12 may mask the true diagnosis of
pernicious anemia. Multiple vitamin deficiency is expected in any
dietary deficiency.Drug interactions:
Most antibiotics, methotrexate and pyrimethamine invalidate
folic acid and vitamin B12 diagnostic microbiological blood assays.
Chloramphenicol may antagonize the hematopoietic response to
vitamin B12. Hematopoietic response in such patients should be
monitored.Colchicine, aminoglycosides, certain anticonvulsants (e.g.,
Phenytoin, Phenobarbital, Primidone), para-aminosalicylic acid or
excessive alcohol intake may impair the absorption of vitamin B12.
Vitamin C may destroy vitamin B12. Patients should avoid ingesting
large amounts of vitamin C within 1 hour of oral vitamin B12
administration.
Histamine2-Receptor Antagonists (cimetidine, ranitidine, nizatidine, famotidine):
May cause vitamin B12 insufficiency by reducing gastric acid
cleavage of vitamin B12 from food sources. This may be important
in patients with low stores of vitamin B12 or in patients taking H2-
antagonists for extended periods of time (>2 years).Pregnancy:
No adverse effects have been reported.Lactation:
Vitamin B12 is distributed into the milk of nursing women in
concentrations that approximate the maternal blood vitamin B12
concentration. No adverse effects have been reported.Autistic spectrum and attention deficit hyperactivity disorder
Autism Spectrum Disorder (ASD) is a neurological and
developmental disorder characterized by impaired social interaction,
abnormal communication and repetitive or unusual behavior [10,11].
Prevalence of ASD is reported to be 1 in 160 children globally [12].
ASD begins from childhood and tends to persist into adolescents
and adulthood. By the age of three, all typical symptoms such as
impaired social reciprocity, poor communication skills and restricted
for repetitive behavior, affecting three major domains are observed.
Associated co-morbidities include epilepsy, bowel disorder,
intellectual disability and type -I diabetes. ADHD on the other hand
includes attention difficulty, hyperactivity and impulsive behavior.
Children with ADHD have difficulty in concentrating on single task
or sitting still for long period of time [13]. Its presence increases
difficulties in academic performance and social interactions besides
leading to low self-esteem. Up to 9.4% of United States children are
diagnosed with ADHD [14].
Role of B12 in ASD and ADHD
Vitamins and minerals are required for normal growth and
development of children. Vitamin B-12 is known to be necessary
for the synthesis of myelin in the body. The development and
pattern of myelination follows a well-described neuroanatomical
arc [15], progressing in a posterior-to-anterior and centre-outwards
spatiotemporal pattern that corresponding to maturing cognitive
functions [16]. That is, there is a strong overlap in the emergence of a
specific cognitive function and the myelination of brain regions and
networks sub serving that function.
Hence it was hypothesized by several researchers that childhood
neurodevelopmental anomalies like ASD or ADHD could be related
to a deficiency of Vitamin B-12. Hence we undertook a review of
literature of the subject to define the scope of existing knowledge on
the subject.
Search strategy
We conducted searches in Medline, Extended Medline (1950
to 22 July 2020) using the following search words (Vitamin B12 or
Cobalamin or Methylcobalamin or Cyanocobalamin) and (Autism,
Autistic spectrum disorder or attention deficit hyperactivity disorder
or ASD or ADHD). We imposed no age or language restrictions. We
also reviewed reference lists of identified articles and hand-searched
reviews, bibliographies of books, and abstracts. We scanned the titles
and abstracts of the trials identified in the computerized search to
exclude studies that were obviously irrelevant. We scrutinized the full
texts of the remaining studies and identified relevant observational
and interventional studies. The studies identified by this exercise are
presented in Table 2.
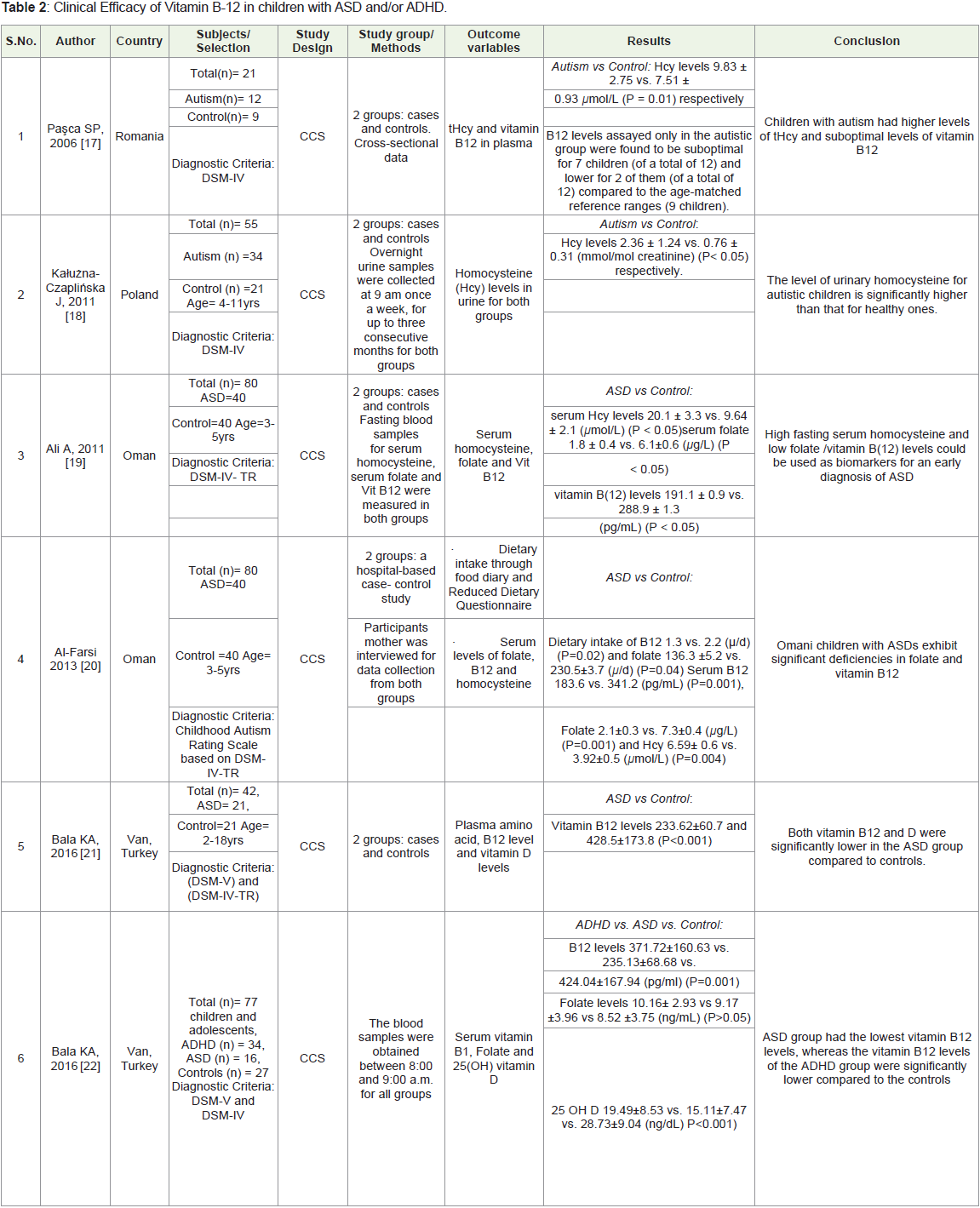
Observational studies:
Several observational studies have documented that children with
ASD or ADHD are deficient in B-12 as reflected in the biochemical
B-12 parameters [17-27]. Table 2 summaries the observational
data on the subject. As presented Pasca et al and Altun et al noted
that children with autism have significant higher levels of total
homocysteine and lower levels of B12 in plasma as compared to age
matched controls [17,26]. A study of Omani children found that
ASD have low dietary intake of B12 and thus have low serum B12
levels compared to neurotypical controls [20]. Another research
on homocysteine levels in urine found to be significantly higher in
autism children [18]. While most studies on ASD children document
B-12 deficiency in children with ASD the results of Chen et al and
Guo et al differed from this general trend. Chen J, in China studied
68 ASD children and documented that maternal serum levels of
vitamin B12 and homocysteine were not significantly associated with
risk of ASD.23 Guo et al, in China studied 371 children (274 ASD)
aged 2-7 years using the Autism Behavior Checklist and their Social
responsiveness scale. No significant difference was found regarding
vit B12 between ASD group and control group (p = >0.106) [26].Two studies report observational data on B-12 levels in children
with ADHD. Both recorded lower B-12 levels in ADHD children than
in controls but the levels in ADHD were higher than those of children
with ASD. Bala et al analysed and compared B-12 levels in ASD
(n=34) [22], ADHD (n=16) and controls (n=27) and noted that the
ASD group had the lowest vitamin B12 levels, whereas the vitamin
B12 levels of the ADHD group were significantly lower compared
to the controls. Similarly, Yektas et al compared vitamin B12,
folate and homocysteine concentrations in ASD (n=48), ADHD
(n=35) and controls (n=35) [28]. ASD had the lowest vitamin B12
and the highest homocysteine levels while ADHD had intermediate
levels. They also noted that Oppositionality and hyperactivity and/or
impulsivity may be related to vitamin B12 and homocysteine levels in
children with ADHD.
Clinical trials:
Pubmed search yielded only 4 Intervention studies using B-12
in children with ASD/ADHD (all were for ASD). Of these only two
studies report the impact of supplementation on behavioral rating
and biochemical B-12 status together. Hendren et al randomized 57
children with ASD to receive either 8 weeks of treatment with methyl B12 (75 mcg/kg) or saline placebo every 3 days in a subcutaneous
injection [29]. The primary outcome measure was overall improvement
in symptoms of ASD as measured by the Clinical Global Impressions-
Improvement (CGI-I) score. Secondary outcome measures included
changes in the Aberrant Behavior Checklist (ABC) and the Social
Responsiveness Scale (SRS). Laboratory measures of methionine
methylation and antioxidant glutathione metabolism were assessed
at baseline and 8 weeks. The primary outcome measure - the clinician
rated CGI-I score -was statistically significantly better (lower) in the
methyl B12 group (2.4) than in the placebo group (3.1) (0.7 greater
improvement in the methyl B12 group, 95% CI 1.2–0.2, p = 0.005).
Clinical improvement among children treated with methyl B12
was positively correlated with increases in plasma methionine (p =
0.05), decreases in S-adenosyl-l homocysteine (SAH) ( p = 0.007)
and improvements in the ratio of S-adenosylmethionine (SAM) to
SAH ( p = 0.007), indicating an improvement in cellular methylation
capacity. No improvements were observed in the parent-rated ABC
or SRS.However, Bertoglio et al in a cross over trial did not find any
statistically significant differences in the overall [30]. However,
Nine (9 of 30) subjects (30%) demonstrated clinically significant
improvement on the Clinical Global Impression Scale and at least
two additional behavioral measures. More notably, these responders
exhibited significantly increased plasma concentrations of GSH
and GSH=GSSG means for behavior or glutathione endpoints
between active and placebo groups. This led the authors to conclude
that methyl B12 may alleviate symptoms of autism in a subgroup
of children, possibly by reducing oxidative stress. An increase in
glutathione redox status (GSH=GSSG) may provide a biomarker
for treatment response to methyl B12. Also, the cross-over design of
the study may not be most appropriate to answer the study question
given that cobalamin could be stored in the liver for a long time up
to 2 to 3 years.
The other two studies primarily evaluated the impact of
supplementation on biochemical parameters. James SJ, et al. in 2009,
supplemented 40 autistic children with 75 μg/kg methylcobalamin
(2 times/wk) and 400 μg folinic acid (2 times/d) for 3 months
[31]. Plasma concentrations of transmethylation/ transsulfuration
metabolites and glutathione redox status in autistic children were
measured as compared to controls. There were significant increases in
cysteine, cysteinylglycine, and glutathione concentrations (P < 0.001).
The oxidized disulfide form of glutathione was decreased and the
glutathione redox ratio increased after treatment (P < 0.008). Kaluzna
et al recruited 51 children (30 ASD and 21 controls) [2,3]. Autistic
children were supplemented daily with Group A1: vitamins B6, B12,
and folic acid and Group A2: vit B6 and B12 in the dose of 200 mg, 1.2
μg, and 400 μg, respectively. All children followed a sugar-free diet.
Pre vs post-treatment (A1 and A2) in autistic children: Homocysteine
levels:
2.41 ± 1.10 vs 1.13 ± 0.44 and 1.33 ± 0.39 mmol/mol creatinine for
A1 and A2 groups, respectively. The authors concluded that the intake
of vitamins B6 and B12, together with folic acid, was more effective
in lowering the levels of urinary homocysteine than the intake of
vitamins B6 and B12 alone.
Conclusion
In conclusion, there is strong theoretical basis for the role of
Vitamin B-12 in DNA methylation and nerve myelination and hence it
is a potential suspect for neurodevelopmental disorders of childhood
like ASD and ADHD. Deficiency of B-12 is common worldwide
and especially in India. The deficiency is reported to be particularly
severe in vegetarian populations. There is ample observational data
(with a few exceptions) from developed countries documenting the
relationship between B-12 deficiency and ASD. Studies on ADHD
are fewer and hence less conclusive. Intervention studies using
B-12 in ASD children have consistently demonstrated biochemical
improvement. There is paucity of trial literature on the clinical
impact of B-12 supplementation in cases with ASD in terms of
behavior ratings. The few existing studies were only from developed
countries and support a potential role for B-12 supplementation in
children with ASD although the evidence is not strong. The studies
were conducted with small sample sizes, showed weak differences
and were weak in design. While it is possible that B-12 might be the
effect of restricted dietary preferences in neurologically compromised
children. It is also possible that some of the neurological effects of
deficiency at a developmentally sensitive stage may not be reversible.
None of the studies were conducted in micro-nutritionally highrisk
settings or in developing countries. Also, none of studies have
evaluated the preventive or longer-term impact of supplementation.
Further work should hence be urgently considered to address these
lacunae.
Funding:
The authors did not receives any financial compensation for
creating this manuscriptConflict of interest:
The authors declare no conflict of interestAuthor contributions: SR and JN conceived the idea. SR
conducted review of literature. SR drafted the manuscript. All authors
have read, reviewed, edited and approved the final manuscript.
Consent: All the authors consent for publication
Ethical Approval: No ethical approval was taken as per
institutional policy.
References
1. Pirkle JL (2016) Laboratory Procedure Manual Vitamin B12 (B12) Roche E‐170 Vitamin B12 " ECLIA ".
4. Combs GF, McClung JP, Combs GF, McClung JP (2017) Vitamin B12. In: The Vitamins. Elsevier 431-452.
Citation
Rawat S, Nagpal J, Jain T. Role of Vitamin B12 in Autistic Spectrum and Attention Deficit Hyperactivity Disorders: A Scoping Review. Indian J Nutri. 2021;8(3): 243.