Review Article
Assessment and Management of Acute Malnutrition in Infants Under Six Months: A Systematic Review
Sirwani B*, Misra H, Shivani C and Rana R
Indian Institute of Public Health Gandhinagar, India
*Corresponding author: Sirwani B, Indian Institute of Public Health Gandhi nagar (IIPHG), Gujarat-382042, India; Email:
barkhasirwani866@gmail.com
Article Information: Submission: 29/07/2021; Accepted: 03/09/2021; Published: 07/09/2021
Copyright: © 2021 Sirwani B, et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: Acute malnutrition in infants under six months (u6m) is increasingly recognized as a serious public health concern, as the evidence from
developing countries suggests that acute malnutrition affects around 8.5 million u6m infants. Despite this, the current evidence base on the management of
acute malnutrition in under six months infants is sparse. The objectives of this paper were to present the burden and underlying risk factors associated with
acute malnutrition and synthesize current evidence on various assessment and management approaches currently in use for infants u6m.
Methods: Two electronic databases, PubMed and Cochrane Library were searched between April 2020 and May 2020. We systematically reviewed the
literature and identified 33 papers that fulfilled the inclusion and exclusion criteria. Results: One third of the identified studies (n=10, 30.3%) were secondary
data analysis. The studies were geographically diverse (LICs + LMICs), of which six were multi-country studies. The review identified that South Asian
countries bear the highest burden of acute malnutrition in u6m infants. In order to identify the u6m infants at the risk of mortality, severe underweight at 6
weeks of age could be a potential indicator (requires further evidence from different contexts). Majority of the studies identified maternal related factors to be
mainly associated with acute malnutrition in u6m infants. Among preventive interventions, one with maternal nutritional supplementation (MNS) in addition to
breastfeeding support showed promising improvement in anthropometric outcomes.
Conclusion: Health programmes, particularly in South Asia region require to focus on maternal related factors to avert and/or manage growth faltering in
u6m infants. Further research on context specific burden of acute malnutrition and identification of underlying risk factors, is urgently required for shaping new
programs and/ or for incorporating u6m in the existing malnutrition management programs.
Keywords
Assessment; Management; Acute malnutrition; Wasting; Infants under six months
Introduction
Childhood malnutrition is a global public health problem
and it is known that majority of the children become susceptible
to malnutrition during periods of vulnerability i.e., during the
intrauterine period and the early years of life [1]. Wasting (acute
malnutrition or wasting have been used interchangeably) in infants
under six months (u6m) is increasingly recognized as a serious public
health concern [2]. Evidence from developing countries reveal, an
estimated 8.5 million infants aged u6m being wasted [3], of which
nearly 4.7 million infants aged u6m being moderately wasted, and
approximately 3.8 million as severely wasted [4]. These wasted u6m
infants constitute an important proportion of all wasted children aged
less than five (< 5) years [5]. More than half of all wasted < 5 children
in the world live in southern Asia [6], and the age distribution of wasting in this region reveals that the highest prevalence is seen at
birth and most of the infants experience their first wasting episode by
three months of age [7,8].
When compared to the older children-the physiological processes,
including thermoregulation, renal and gastrointestinal functions, are
relatively immature in infants u6m [9], Infants are more susceptible
to frequent and severe infections as their immune systems are still
developing [1], they are less able to make their needs known and are
more vulnerable to the effects of poor parenting [10], diagnosing
oedema in infants might be more challenging, as most of the older
children can stand, and gravity might influence in narrowing the
location of the oedema to the limbs in the older children and also,
evidence suggests that infants u6m face higher mortality risk during
treatment of acute malnutrition [11].
There are several risk factors associated with wasting infants u6m.
Some studies have broadly categorized these risk factors into infant related,
maternal-related, and household-related factors [7,12]. Most
commonly, severe acute malnutrition in this age group is known to
occur due to suboptimal feeding practices, especially breastfeeding
practices [9,13]. As per WHO recommendations, infants u6m should
be exclusively breastfed however [14], in low-income and lower-middle
income countries (LICs and LMICs), only 37% of children
younger than 6 months of age are exclusively breastfed [15]. Studies
have shown that even exclusively breastfed infants are susceptible to
acute malnutrition [16,17].
Assessment of infants u6m is an essential step to identify acutely
malnourished infants and accordingly enroll them into nutrition
programmes. However, authors have reported that infants u6m are
often excluded from nutrition surveys and marginalized in nutrition
programmes [12]. The two anthropometric indicators commonly
used for assessing severe acute malnutrition (SAM) in children aged
6-59 months are also being considered for infants u6m [9], namely
weight-for-height z score (WHZ) and mid-upper arm circumference
(MUAC). However, in order to compute WHZ, length/ height is
required, which is especially difficult to measure in younger infants
(u6m infants) [18]. Further, there are no standards for calculating
weight-for-height (WFH) for those with length <45 cm [19].
It is challenging to manage malnutrition in u6m infants as it is
complex and multifactorial [12,19]. Thus, in 2013, for the first time
WHO guidelines on the management of SAM recognized u6m as a
special group and included a chapter dedicated to the management of
infants u6m [9]. Facility-based management of these infants include
the use of F-75 or diluted F-100 milk via a supplementary suckling
technique until exclusive breastfeeding is re-established with/without
antibiotic therapy during the stabilization phase [20]. Focusing
only on facility-based strategies might lead to increased admissions,
which might have serious implications on resources [21]. Hence,
WHO mentions community-based management approach for
uncomplicated cases/at-risk infants. Findings from a qualitative study
in Senegal showed that community-based care for uncomplicated
cases of acute malnutrition in infants u6m improved their access to
care [22].
With paucity of evidence on actual burden and associated risk
factors, also, with uncertainty in assessment and management
approaches, it is difficult to design specific programs focusing on
u6m infants. Through this review, we aim- to present the estimated
the burden of acute malnutrition in u6m infants and also explore and
synthesize evidence on various assessment and treatment approaches
used for infants u6m.
Objectives:
- To explore and synthesize evidence on various assessment
and treatment approaches used for infants u6m.
- To identify the current evidence on burden of acute
malnutrition in infants u6m.
- To explore and identify underlying risk factors associated
with acute malnutrition in infants u6m.Methods:
The methods for this review follow the criteria of the PRISMA
(Preferred Reporting Items for Systematic Reviews and Meta-
Analyses) statement [23].Information Source and Search Strategy:
The literature search was conducted on two electronic databases-
PubMed and Cochrane Library. At the initial stage filter for language
(English), species (Human), age (Infant: birth-23 months, Infant:
1-23 months, Newborn: birth-1 month) and publication date (2000-
2020) were applied in PubMed database. For PubMed database both
‘controlled vocabulary’ and ‘free-text’ terms were used. Similar search
terms were applied for both the databases, according to databases’
advanced search set-up. The final search strategy was run on 15th
May, 2020.Search Strategy: ((((“Infants”[Text Word] OR (“under”[All
Fields] AND “six months”[Text Word])) OR ((((“infant”[MeSH
Terms] OR “infant”[All Fields]) OR “Infants”[All Fields]) OR
“infant s”[All Fields]) AND “under 6 months”[Text Word])) OR
((((“infant”[MeSH Terms] OR “infant”[All Fields]) OR “Infants”[All
Fields]) OR “infants”[All Fields]) AND “aged 6 months”[Text Word]))
AND (((((((((((((“management”[Text Word] OR “admission”[Text
Word]) OR “admission profile”[Text Word]) OR “Discharge”[Text
Word]) OR “discharge outcome”[Text Word]) OR “outcome”[Text
Word]) OR “diagnostic criteria”[Text Word]) OR “prevalence”[Text
Word]) OR “risk factor”[Text Word]) OR “support”[Text Word])
OR “breastfeeding support”[Text Word]) OR “F-100”[Text
Word]) OR “diluted f-100”[Text Word]) OR “infant formula”[Text
Word])) AND (((((((((((“severe acute malnutrition”[Text Word]
OR “sam”[Text Word]) OR “severe malnutrition”[Text Word])
OR “acute malnutrition”[Text Word]) OR “wasting”[Text
Word]) OR “wasted”[Text Word]) OR “MUAC”[Text Word])
OR “weight for age”[Text Word]) OR “WAZ”[Text Word]) OR
“weight for height”[Text Word]) OR “WHZ”[Text Word]) OR
“Anthropometry”[Text Word]).
Study selection:
Screening: The selection of the studies was performed using two
stage selection process using explicit inclusion and exclusion criteriafirst
based on title and abstract and later based on full-text. It was
performed in EPPI-Reviewer software (version: 4.11.1.1) [24].Inclusion Criteria:
- Population: Infants u6m of age (Low birth weight infant,
preterm infants, small for gestational age were included)
- Intervention(s)/Exposure(s): risk factor, diagnostic criteria,
admission/ discharge criteria, formula feeding, F-100/ diluted
F-100, counselling of mothers of u6m infants (prenatal as
well as postnatal), postnatal interventions on mothers of u6m
infants.
- Comparator: Any
- Outcome: any of the following- Weight-for-age (WAZ),
Weight-for-height (WHZ), Mid Upper Arm Circumference
(MUAC), morbidity, mortality due to malnutrition.
- Context: Studies with a focus on LIC or LMIC, based on
World Bank classification of country on income group, 2019
(in case of multi-country study, at least one country belongs
to LIC/LMIC group) [25].
- Study design: observational, interventional and secondary
data analysis studiesExclusion Criteria: We excluded the articles that were qualitative,
systematic reviews, trial protocols, case studies, or published in
abstract form only. Articles, where the evaluation was done for congenital
abnormalities, diseases, illness, hospitalization for reason other than
malnutrition or HIV-exposed population was excluded. Articles with
prime focus on overweight/obesity or stunting (chronic malnutrition)
were also excluded.
Data Extraction:
The extracted data included characteristics of the study
population, brief description of-intervention (s)/ exposure (s),
comparator if present in the study, outcome and context.Quality Assessment:
Quality assessment was performed for all the studies except for
studies with secondary data analysis study design. Two checklists
were used- for interventional studies, quality was assessed using
‘Methods for the development of National Institute for Health
and Care Excellence (NICE) public health guidance’ [26], and
for observational studies, the quality was assessed using- ‘Quality
assessment tool for observational cohort and cross-sectional studies
and, quality assessment tool for case-control studies by National
Institute of Health, National Heart, Lung, and Blood Institute (NIH,
NHLBI)’ [27].Analysis:
The analysis is presented in the form of a narrative synthesis.
However, where the authors had stated significance of the finding, it
is presented in the results table as P-values. The evidence is presented
as- (percentage/mean/ratio/median) for the u6m population as
one group or as a comparison between the intervention group (IG)
and the control group (CG). Since this review involves a variety of
interventions/exposures, this led to a methodological heterogeneity
in the results. Thus, final results are presented under categories/
clusters, formed based on the type of intervention/exposure identified
in the included studies.Ethical Approval:
The review protocol was submitted to the ethical committee at
the Indian Institute of Public Health, Gandhinagar (IIPHG). The
protocol was assessed by research ethics committee and an exemption
was granted.Results
Study Selection:
Initial search identified 3,689 articles. Of these, 440 articles were
removed as duplicates, the remaining 3,249 records were screened in
stage-1. The screening based on title and abstract lead to exclusion
of another 3,177 records. Remaining 72 records were included in stage-2 for full text assessment. Of these, 39 were excluded based on
predetermined inclusion and exclusion criteria. Finally, 33 records
were included for analysis (Figure 1).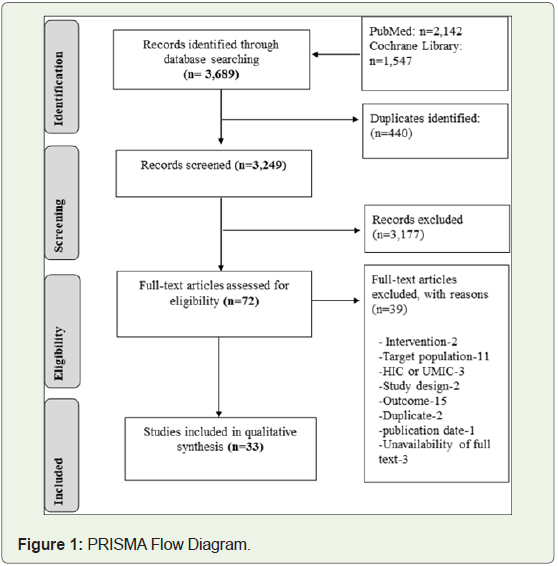
Study Characteristics:
Characteristics of the included studies are presented in Table 1.
Among the included studies, one-third of the studies were secondary
data analysis (SDA) followed by seven randomized controlled trials
(RCTs) seven prospective cohort studies (PCS) [3,11,13,16,18,28-46]
(Table 1). Six studies were multi-country studies [3,11,18,30,32,36],
followed by six studies from India [16,31,35,40,47,48] and three from
each of these countries-Uganda [29,46,49], Bangladesh [38,42,43],
Pakistan [39,45,50], Kenya [28,34,51].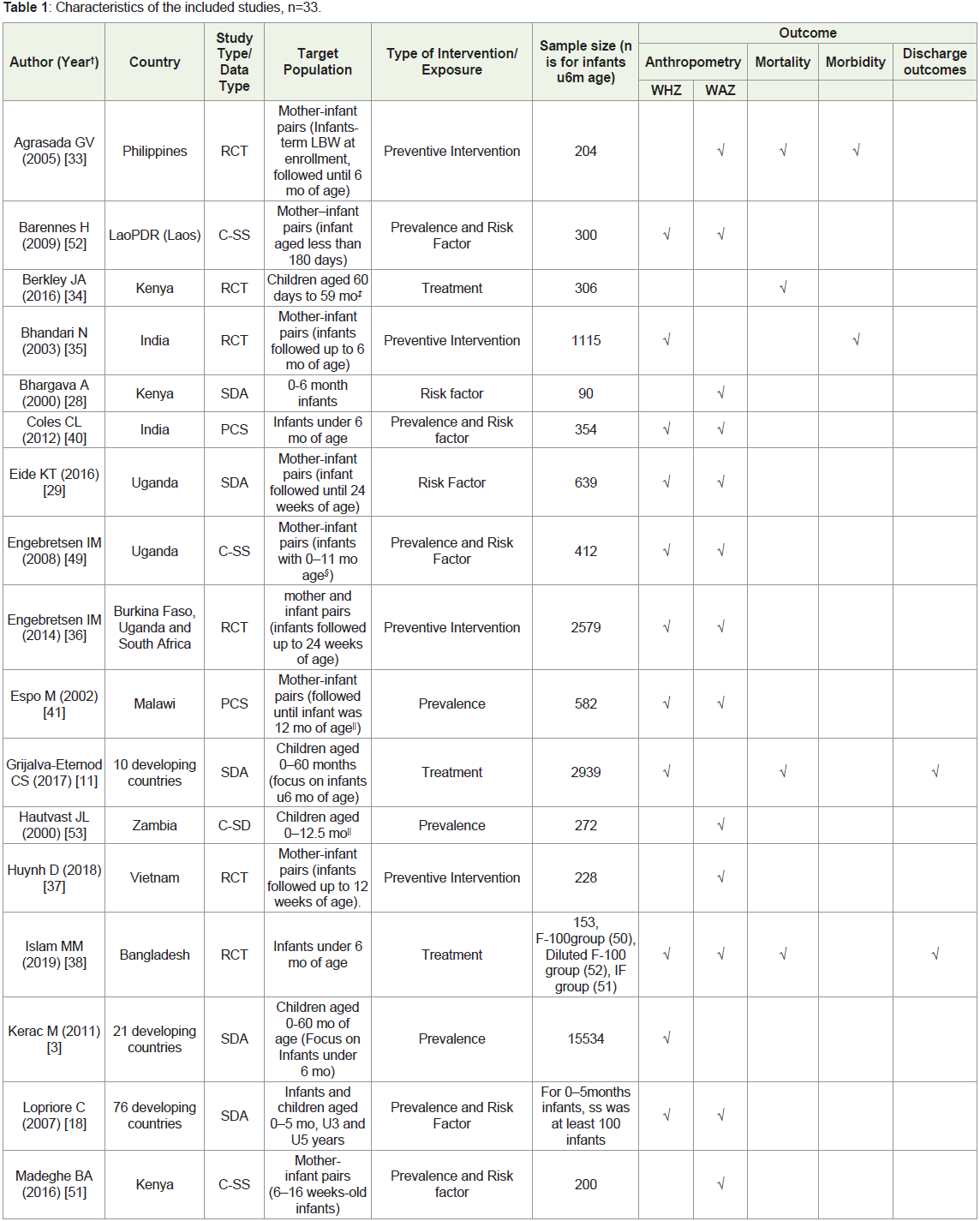
Result of Studies:
Interventions and Outcomes: Of 33 studies, 12 (36.4%) studies
observed both prevalence and risk factors, seven (21.2%) studies
focused on prevalence, six (18.1%) assessed preventive interventions,
four (12.1%) focused on treatment of wasting and three (9.1%)
assessed risk factors associated with malnutrition (Table 1). One (3%)
study focused on the assessment i.e., indicators used to assess acute
malnutrition and predicting mortality in malnourished infants.Of the total studies, anthropometry outcome was measured in 30
studies (90.9%), morbidity outcome in six studies (18.1%), mortality
was observed in six studies (18.1%) and discharge outcomes in three
studies (9.1%) (Table 1).
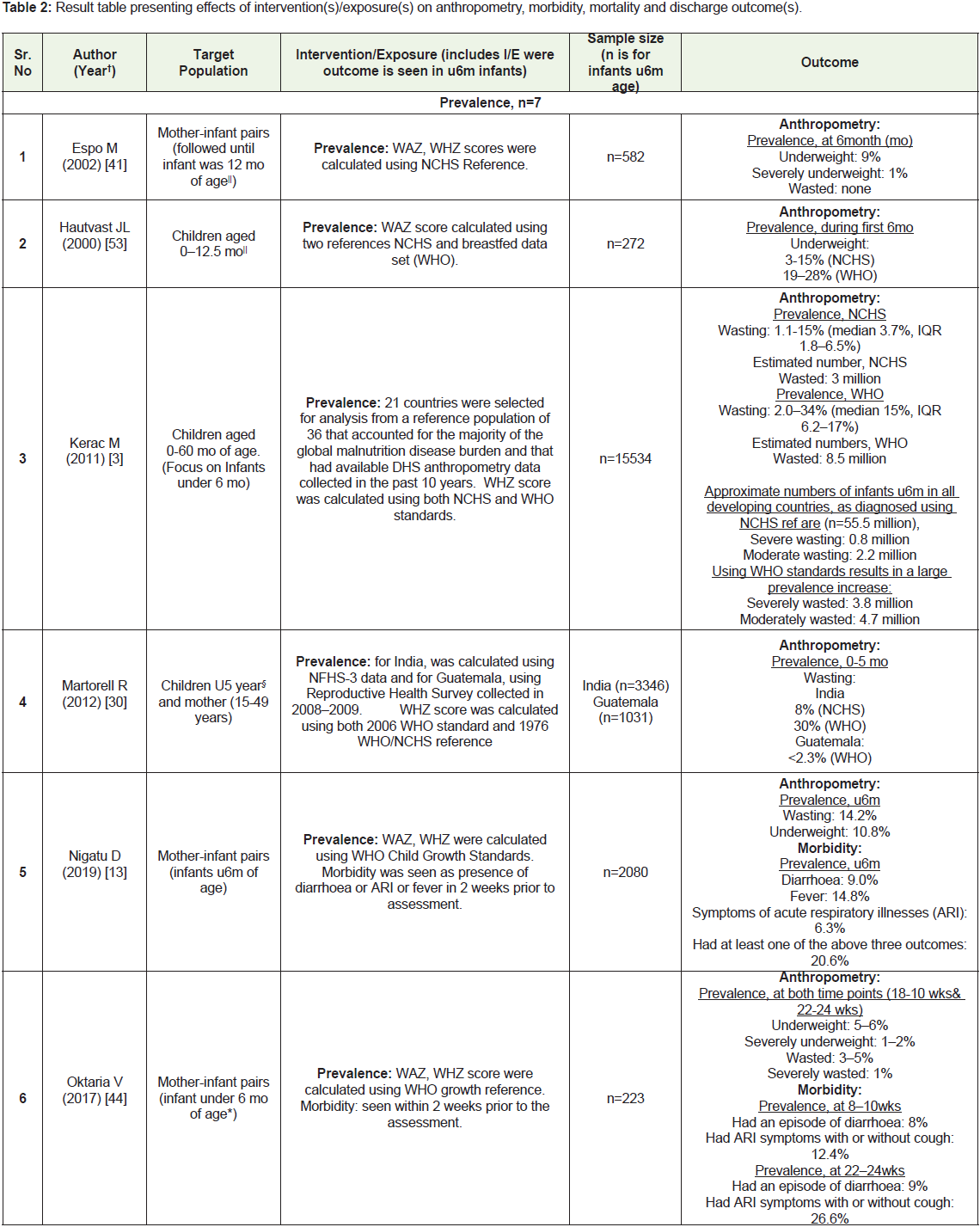
Effect of Interventions on Specific Outcomes: Anthropometry Outcomes: Of total 30 studies reporting outcomes on anthropometry,
26 reported WAZ and 21 reported WHZ. Of these, 12 focused on
both prevalence and risk factors, seven focused on prevalence, six
on preventive interventions and two on treatment aspect of acute
malnutrition in u6m infants (Table 2).
Effect of intervention/Exposure on outcome (for details of each
study refer Table 2).
Prevalence (WHZ): Of the total 21 studies reporting WHZ, 15
studies presented prevalence of wasting in infants u6m. Of these,
11 considered prevalence based on WHO growth standards, two considered prevalence based on National Center for Health Statistics
(NCHS) growth standards, while two studies compared prevalence
based on both the standards. Prevalence of wasting was measured at
different ages/ time points in different studies, however, all the studies
measured prevalence among infants ≤ 6 months.
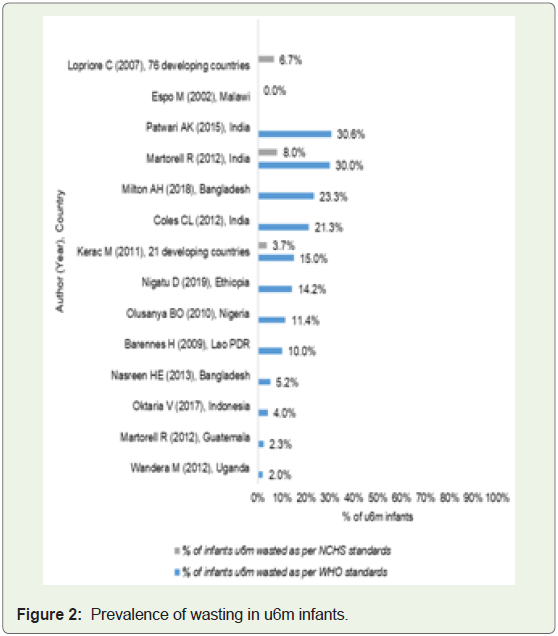
Figure 2 presents prevalence reported as per WHO/ NCHS
growth standards in the studies, except one study that reported mean
WHZ score [49], Which is not presented in this figure. As per WHO
growth standards, highest prevalence of wasting was observed in
an India based study- 30.6% infants u6m reported as wasted [16].
Lowest prevalence was reported as 2% in Uganda [46]. As per NCHS
standards, highest prevalence was reported as 6.7% by a multicountry
study [18]. Lowest prevalence was reported as 0% in Malawi
[41] (Figure 2). While severe wasting was reported by Nigeria based
case-control study- among all the cases of 0-3 months infants with
undernutrition, 22.9% (0-3 mo) infants were reported to be severely
wasted [55].
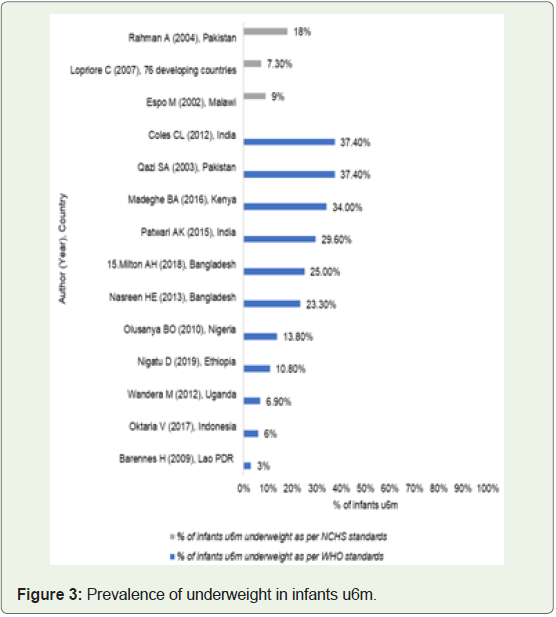
Prevalence (WAZ): Of the total studies, 17 had reported
underweight prevalence. Of which, 13 studies measured prevalence
of underweight based on WHO growth standards, three studies
measured underweight based on NCHS standards and one study
reported prevalence based on both the standards. Prevalence of
underweight was measured at different ages/time points in different
studies, however, all the studies measured prevalence among infants
≤ 6 months of all the studies reporting underweight prevalence, a
Zambia based study reported prevalence in the form of range (19-
28% as per WHO standards and 3-15% as per NCHS) and another
Uganda based cross-sectional study reported mean WAZ score
(-0.41) [49,53]. Results of remaining 14 studies are shown in Figure 3 - as per WHO standards, highest prevalence of underweight was
observed in two studies, one was India based study and another
was Pakistan based study [40,50]. A case-control study conducted
in Nigeria reported very high prevalence (%) of severe underweight
among cases of 0-3 months infants with undernutrition(55)Risk
factors (WAZ / WHZ) (for details of each study refer Table 2): Of
the total 15 studies focused on risk factors, 13 studies reported factors
associated with WAZ/ underweight and nine studies reported factors
associated with WHZ/ wasting in infants u6m. Various risk factors identified from these studies are presented below:
• Maternal BMI: Two studies reported maternal BMI [18,28]
as a significant factor correlated (Spearman rank correlation coefficient, r=0.78) [26] /associated with underweight/ WHZ in infants u6m (P< 0.05) [28].
• Maternal depression: Three studies reported maternal depression as a factor associated with infant’s underweight.
Two studies found significant association of maternal
depression with underweight in infants u6m [45,51].
Rahman et al. (OR 3.5; 95% CI: 1.5-8.6; P<0.01) [45], and
Madeghe et al. (adjusted odds ratio- AOR 5.79; 95% CI: 2.14
–15.62; P = 0.001) [51], however one study focused on both
prenatal as well as postnatal depression and other study
reported only postpartum depression [45,51]. On the other
hand, Nasreen et al. found non-significant association of
maternal depressive symptoms (during pregnancy and 2-3
mo postpartum) with infant’s underweight at 2-3 mo [43].
Place of Delivery: Two studies (Nigeria-based) found a place
of delivery as a factor significantly associated with underweight or
wasting in infants u6m [54,55]. Of these two studies, one was a
case-control, which found that infants delivered at residential homes
compared with the public hospitals had almost threefold odds of
being severely underweight (AOR 2.98; 95% CI: 1.51–5.88; P= 0.002)
or severely wasted (AOR 2.90; 95% CI: 1.32–6.37; P = 0.008), when
controlled for potential confounders [55]. The other study which
was cross-sectional in nature reported infants born out of hospital
had higher odds of being underweight (OR 1.27; 95% CI: 1.08, 1.49;
P=0.004) or wasted (OR 1.44; 95% CI: 1.20, 1.73; P<0.001) compared
to those born at hospitals [54].
Socioeconomic Status: Three studies observed association
of indicators related to socioeconomic status of the family with
underweight or wasting in infants u6m [29,45,50]. The Uganda
based study performed secondary data analysis to see socioeconomic
distribution of underweight or wasting, and found that prevalence
of underweight (at 24 wks: concentration index -0.226, at 12 wks:
concentration index -0.301) or wasting (at 24 wks: concentration
index -0.253, at 12 wks: concentration index -0.213) was significantly
concentrated among poor [29]. Another study from Pakistan,
reported family income as a factor associated with underweight and
found that higher proportion of infants from low income families
were underweight when compared to infants in moderate income
families (OR 1.15, 95% CI: 1.03-1.29, P = 0.017) [50]. Rahman et
al found relative poverty as a factor significantly associated with
underweight (OR 2.3; 95% CI: 1.1-5.2; P< 0.05) in infants u6m [45].
Other Factors:
Maternal Factors: Maternal haemoglobin concentration and
mother’s education status were significantly and positively associated
with underweight. Mother’s periodontal health was significantly
associated with infant’s WHZ. Factors like maternal autonomy
[28,54,46,47], mother’s childbearing age and having multiple
pregnancies were significantly associated with underweight or
wasting in infants u6m. While, association of restricted maternal
diets, during postpartum period with infant’s underweight or wasting
was found to be negative, but insignificant [52,54].Infant Related Factors: An India based study found that
nasopharyngeal carriage of streptococcus Pneumococci (spn) in
infants (at 2 mo) was significantly associated with WAZ score but
not with WHZ (at 6 mo) [40]. Another study reported that infant’s
gender (i.e. when compare to female, male infants had higher odds of
being underweight- OR 1.31, 95% CI 1.21, 1.54, P=0.001 or wasted- OR 1.26, 95% CI 1.05, 1.50, P=0.011, adjusting for covariates) and
this association was found to be significant, however history of
hyperbilirubinemia was associated with underweight only [54]. Two
studies observed infant’s morbidity status as a risk factor [28,45].
Of these, one study reported that ≥ 5 diarrhoeal episodes per year
was significantly associated with underweight [45], while the other
reported no significant association of infant’s morbidity index with
underweight [28].
Household Factors: A Bangladesh based longitudinal study
observed association of household (HH) arsenic exposure on infant’s
underweight or wasting, but found it to be insignificant [42]. Another
study reported, living in rented accommodation vs owned was
associated with a lower risk of infant being underweight (OR 0.64;
95% CI: 0.45, 0.90; P=0.011) or wasted (OR 0.45; 95% CI: 0.31, 0.65;
P<0.001) [54].
Preventive Intervention (WAZ): All the six studies with focus on
preventive intervention reported anthropometric outcomes. Of these,
five studies reported WAZ/ underweight [33,36,37,39,48] (for details
of each study refer Table 2). Of these five studies, two were communitybased
studies, where counseling on EBF was given through home
visits. However, one study had peer counselors selected from the
same village [36], while the other one had two intervention groups
with breastfeeding (BF) counselors or childcare (CC) counselors
[33]. At end of the trial both the studies found only small changes
in WAZ scores of IG vs CG, which were non-significant [33,36]. A
prospective cohort assessment was conducted in India to evaluate
a program that in addition to government services, involved age
specific recommendation of BF and CF in the intervention arm. The
results showed that the proportion of underweight in IG (37.2%) was
lower than CG (44.4%), but this difference was insignificant [48]. On
other hand, Vietnam based RCT in conjunction with a breastfeeding
support program also used maternal nutritional supplementation
(MNS) in the intervention arm and at the end of the trial, trends for
WAZ score development over time (birth to 12 weeks postpartum,
estimate 0.16; 95% CI: -0.03, 0.36, P=0.0636) were significantly higher
in the intervention group [37]. Only one study had the intervention
focused on mothers with depression, which involved home-based
cognitive behavior therapy sessions in the intervention arm, at the
end of the trial differences in infant’s WAZ score (adjusted mean
difference - 0.02; 95% CI: −0.18 to 0.14, P=0.76) was non-significant
[39].
Preventive Intervention (WHZ): Of six studies, only two
reported WHZ/wasting [35,36]. Both the studies had communitybased
counselling of EBF as intervention. Of the two, an India based
study found that prevalence of wasting in IG vs CG was 3% vs 3%
and for LBW infants it was 3% vs 5%, with this difference being nonsignificant
[35]. The other study was a multi-country trial, which
showed the differences in wasting prevalence ratios between two
groups were small and non-significant in Burkina Faso and South
Africa, while in Uganda prevalence of wasting in IG vs CG was 7.56%
vs 3.16%, and was significant [36].
Treatment (WAZ / WHZ): Of the four studies focusing on
treatment aspect, only two had reported anthropometry outcomes
[11,38]. First was a study on the dietary management in the rehabilitation phase of SAM in infants u6m, which described three
interventions F-100, diluted F-100 (F-100D), and Infant Formula
(IF). Positive impacts on WAZ scores and WLZ scores in all the three
groups were reported at the end of the trial, but significance of these
changes was not reported [38]. However, duration of recovery was
reported to be significantly better with F-100D (median duration in
days: F-100 vs Diluted F-100 -1.9, 95% CI -3.9 to 0.2, P=0.07; F-100
vs IF: - 3.3, 95% CI -5.7 to -0.9, P=0.008; Diluted F-100 vs IF: -1.4,
95% CI - 3.8 to 1.1, P=0.26) [38]. The other study was on inpatient
therapeutic care program for acute malnutrition, which reported
85.0% infants u6m being wasted at admission, of which 14.5% were
moderately wasted and 70.6% were severely wasted and mean WHZ
score for infants u6m was -3.89 [11].
Morbidity outcome(s): Of total six studies reporting morbidity
outcomes, three were prevalence studies [13,44], Two studies
focused on preventive intervention [33,35], and one study focused on
treatment component of acute malnutrition/ wasting in infants u6m
[31] (Table 1).
Effect of intervention/Exposure on outcome (for details of each
study refer Table 2).
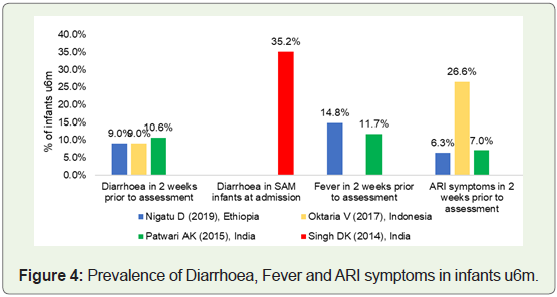
Prevalence: Three studies that reported morbidity prevalence in
infants u6m are shown in Figure 4. Highest prevalence of diarrhea was
reported by India based SDA [16], while highest prevalence of fever
was reported by a SDA performed in Ethiopia and highest prevalence
of ARI symptoms was reported by a study conducted in Indonesia
[13,,44].
Preventive intervention: Both the studies assessed community-based
counseling on EBF as an intervention and no specific intervention
was provided to the control group. One was Philippines based RCT that reported IG2: childcare group and CG: control groups had
higher rates of diarrhea (IG2=28.3% and CG=30.5%) than the IG1:
breastfeeding counselled group (IG1=15%) [33]. The other study was
India based RCT, which reported prevalence of diarrhea at 6 months
in IG vs CG was (25% vs 28%), i.e., significantly lower in intervention
group (P=0.04) [35].
Treatment: One study observed admission profile of infants
u6m with SAM admitted in Nutrition rehabilitation center (NRC) in
India, and reported- at admission most common symptom that the
infants presented with, was acute diarrhoea [31] (Figure 4).
Mortality outcome(s): Of the six studies reporting mortality
outcome, four focused on treatment [11,31,34,38]. Among remaining
two, one was based on preventive intervention [33], and other on
assessment aspect [32] (Table 1).
Effect of intervention/Exposure on outcome (for details of each
study refer Table 2).
Treatment: Among the four studies, two studies were SDA
[11,31], one was India based study, that analysed data to see discharge
outcomes of 108 infants with SAM admitted in NRC and reported
death of 3 infants [31]. Other study was based on data from 10 countries
and reported death of (4.60%) infants u6m before discharge, also
infants u6m were found to have a greater risk of mortality (risk ratio
1.30, P< 0.01) during treatment, when compared to older children
[11]. Mortality in IG vs CG was reported by two RCTs [34,38]. One
RCT with intervention- daily co-trimoxazole prophylaxis given to
children without HIV being treated for complicated SAM, reported
(21.62% vs 27.21%) 2-5 months old infant deaths in IG vs CG [34].
Other study, compared three diets for dietary management in the
rehabilitation phase of SAM in infants u6m- Group1: F-100, Group2:
F100D and Group3: IF, and death at the end of trial was reported in
F-100 group only (2%) [38].
Assessment: A multi-country study, determined the sensitivity
and specificity of nutritional status indicators for predicting death
during infancy and reported that- at 6 weeks of age, underweight or
wasting in India was associated with an increased risk of death before
6 months of age, while no indicator was a good predictor of mortality
at 6 months age in Ghana or Peru [32].
Discharge outcome(s): Of the four studies that focused on
treatment, three reported discharge outcomes [11,31,38]. A study
with three IGs (F-100 vs F-100D vs IF) reported duration of recovery i.e., infants who received F-100 recovered more quickly than infants
who received infant formula (P = 0.016) but not more quickly than
infants who received diluted F-100 (P =0.09) [38]. Another study
reported percentage of infants admitted in NRC that were cured i.e.,
69.4%, while percentage of infants u6m non-recovered were 26.8%
[31]. Of those cured, 42.6% were cured using supplementary suckling
technique (SST), 30.6% cured using F-100D and 26.6% cured with
correction of positioning and attachment only [31]. The study based
on SDA of datasets on inpatient therapeutic care programme for acute
malnutrition from 10 countries reported- 75.7% infants as recovered,
while 10.2% as non-recovered [11] (refer Table 2 for details).
Discussion
Summary of Evidence:
The review included 33 studies that were focused on different
aspects related to acute malnutrition in u6m infants. These studies had
varied methodology and were from different countries belonging to
LICs or LMICs [25]. Majority (n=22) of the included studies focused
on prevalence and risk factors associated with acute malnutrition.
However, the target population was diverse in these studies, with
some having sole focus on u6m infants while others incorporating
sub group analysis for this age group.Only one study focusing on assessment of u6m infants with acute
malnutrition met the inclusion criteria. The study reported that, to
identify infants at higher risk of mortality at 6 months age, severe
underweight at 6 weeks age (i.e., age of routine immunization)
could be considered as better indicator when compared to low WLZ
score [32]. Similar findings were reported by Lelijveld N et al., in a
review of methods to detect cases of severely malnourished infants
u6m, the author rated WFA, MUAC as indicators over WLZ, for
acute malnutrition and associated mortality in infants u6m [56]. The
probable explanation for this could be the fact the WLZ has poor
predictive value or low sensitivity to predict infant’s death and many
WLZ values are incalculable using current WHO growth standards
[56,57,58]. WHO’s current recommendations for u6m infants
adopted the same criteria used for older children (i.e., use of WLZ
for identifying mortality risk), however these recommendations were
made in absence of quality evidence and recently emerging evidence
has reported WLZ as poor indicator for u6m infants [9].
Four studies focusing on the treatment aspect were identified in
this review [11,31,34,38]. The included studies found that u6m infants
had a higher risk of mortality during treatment compared to the
older children. However, u6m infants showed less default rate than
the older children at discharge [11,34]. The higher vulnerability of
these u6m infants could be one of the reasons explaining their higher
mortality rate, when compared to older children (6- 59 months age).
In the study by Singh et al., majority of the inpatient infants were
treated by simple interventions like- counselling, SST, correction
of breast positioning and attachment [31]. These findings suggest
that simple interventions could be easily incorporated in outpatient
programs and a considerable case load of u6m could be managed in
community itself, reserving the inpatient admissions for complicated
cases (cases with oedema and danger signs).
For inpatient management of u6m infants with SAM, WHO
guidelines based on earlier evidence stated F-100 to be unsafe for
u6m infants with SAM, owing to high renal solute load and risk of
hypernatraemic dehydration [9]. However, recent evidence from a
study conducted by Islam et al., suggested that for infants who are
gaining weight rapidly in a hospital environment with well-controlled
preparation of feeds, F-100 is safe and that there is no need to prepare
an alternative type of feed for infants u6m [38]. These contrasting
findings highlight the need of further research in this field to generate
concrete evidence.
The review also explored postnatal/ postpartum interventions
that prevent growth faltering in u6m infants. Studies (n=4) mainly
involved community-based promotion of breastfeeding practices
as the intervention [33,35,36,48]. These interventions successfully
improved breastfeeding practices in the intervention group and
two studies, reported significantly less diarrhea prevalence in IG
[33,35]. However, this improvement was not translated to infant’s
anthropometric outcomes at 6 months. This review observed
outcomes at 6 months only. Thus, it is possible that improvement in
anthropometry might have occurred, when follow up was carried out
at later ages.
A study by Huynh et al, incorporated MNS in the intervention, in
conjugation with BF support. This intervention reported significant
trends for higher WAZ score development over time (birth to 12
weeks postpartum) in the infants of IG [37]. This finding explains the
importance of incorporating mother’s nutritional component in the
interventions addressing the prevention of growth faltering in u6m
infants.
Another study that offered cognitive behavioral therapy
(counseling sessions) for mothers with depression presented no
significant differences in underweight prevalence between IG vs CG,
but other significant benefits of this intervention were reported [39].
Risk factors associated with acute malnutrition in u6m infants
were reported by (n=15) studies in this review. The factors that were
reported as significant were grouped into three categories- maternal
related, infant related and HH/ sociodemographic related. Majority
of the studies reported maternal related factors. Factors like maternal
autonomy, mother’s childbearing age, place of delivery, and parity
were significantly associated with either underweight or wasting.
While, maternal BMI, mother’s mental health (depression), maternal
education, maternal hemoglobin concentration were factors
significantly associated with infant’s underweight/WAZ score. On the
other hand, mother’s periodontal health (low CPI score) was found
as a significant risk factor associated with infant wasting/WHZ score.
A systematic review by G.J. Carlson et al., reported similar
findings in terms of, positive association between maternal autonomy
and child’s nutritional indicators in developing countries [59]. This
review considered broad age group of children (0-60 months age) as
target population, however there were studies that incorporated u6m
infants as well.
The review also identified many infant-related risk factors,
like infant’s gender and chronological age, which were found to be
significant risk factors associated with both underweight or wasting. While, nasopharyngeal carriage of pneumococci (spn) in infants at
2 mo age, history of hyperbilirubinemia, ≥5 diarrhoeal episodes per
year, were the risk factors significantly associated with underweight/
WAZ score. In addition, acute malnutrition in u6m infants was more
concentrated among poor and low-income families.
Some factors that were reported as non-significant by the authors
were- HH arsenic exposure, maternal restricted diets in pospartim
period, number of siblings, maternal and infant’s morbidity index,
and others. However for HH arsenic exposure, author reported no
association of HH arsenic exposure with underweight or wasting but
found association with stunting, indicating a chronic long term effect
of HH arsenic exposure [42].
This review also identified burden of acute malnutrition in u6m
infants. Studies reporting the prevalence of wasting and underweight
were from three regions according to World Bank classification, i.e.,
South Asia, Sub-Saharan Africa, and East Asia & Pacific [25]. The
highest prevalence of both wasting and underweight as per WHO
growth standards was found in the South Asia region. With 30.6%
and 30.0%, two India based studies reported the highest wasting
prevalence followed by Bangladesh with 23.3% [16,30,42], with both
the countries falling in a critical situation as per WHO cut-off values
for public health significance. Similar findings were reported in a oneday
consultation organized by UNICEF on wasting in South Asia,
which reported that more than one in three children in India have
wasting (WHZ <-2 SD) during the first three months after birth [8].
When looking at underweight prevalence found in this review, as per
WHO cut-offs, very high underweight prevalence was reported from
both India and Pakistan (37.4%), followed by Kenya (34%), and high
prevalence was reported from Bangladesh based study (23% to 25%).
Limitations and Strengths of the study:
The findings of this review should be interpreted with the
following limitations. For screening based on title & abstract, studies
where age group was not mentioned or had a broader age group (<1,
<2, <5 years or <11, <23 months, etc.), inclusion for full-text screening
was considered if sub-group analysis was mentioned in the abstract
or based on the reviewer’s judgment. During the initial search some
filters were applied in the search strategy, this could have led to a
bias in the total number of records found initially. Due to the broad
scope of this review, there was considerable heterogeneity in the
interventions and outcomes. A large number of studies were included
based on the full text; hence details of individual studies could not
be discussed. A qualitative tool was used for quality appraisal, which
could have led to reviewer bias. Another limitation is that the review
did not look at the interventions given to mothers prenatally, and
likewise, interventions that had seen outcome at the age beyond 6
months were not considered in the review.In spite of these limitations, this review also has some
considerable strength. To our knowledge, this is the first review that
presents burden and risk factors of acute malnutrition in u6m infants
along with the preventive interventions, assessment, and treatment
approaches used for u6m infants with acute malnutrition in LICs and
LMICs.
Implications for Practice and Research:
The review identified high burden of acute malnutrition in u6m
infants in LICs and LMICs which recognizes an urgent need to plan
programs and invest resources for management of acute malnutrition
in u6m. The review also identified various risk factors associated
with acute malnutrition in u6m and knowledge about these factors
would help in planning the strategies to prevent growth faltering in
infants of this age group. Evidence from this review could be helpful
in strategizing community-based support of breastfeeding mothers
as a treatment option for uncomplicated cases (without oedema and
danger signs) of malnutrition in infants u6m.Routine immunization visits shortly after birth could be utilized
as an effective platform for anthropometric assessment of u6m
infants to identify wasted infants at a higher risk of death and thus
targeted interventions could be planned accordingly. In addition, as
mother’s mental health is found to impact infant’s health, training of
community/ frontline health workers could be considered for early
screening and identification of depression symptoms in mothers.
Detecting and treating maternal depression and child malnutrition
simultaneously could be an effective approach and programs can
integrate a psychosocial component into existing maternal and child
health interventions.
Research Gaps Identified in the Study:
Of all the 33 included studies, only 17 studies had prime focus
on u6m infants, while rest were studies that had a component of
sub-group analysis in u6m infants. Majority of the studies that
reported prevalence and risk factors had SDA as study design. Thus,
considerable gap was observed in context specific primary studies
with a focus on u6m infants.The number of studies that measured the impact of preventive
interventions on anthropometry and morbidity outcome was
very limited, as most of the studies focus only on measuring the
improvement in breastfeeding practices.
The review also found that the number of studies focusing on
assessment and treatment aspect were very limited. In future studies
presenting evidence on the feasibility and accuracy of using MUAC
to identifyu6m infants at higher risk of mortality is required. Also,
research to identify effective choice of therapeutic milk for infants
u6m and follow-up of malnourished non-breastfed infants.
Studies exploring psychosocial support activities to manage
depression in pregnant and lactating women and its effects on
improving infant’s nutritional status, require urgent consideration.
Conclusion
The review systematically synthesized evidence on burden, risk
factors, different preventive interventions in practice, assessment and
treatment strategies to manage acute malnutrition in infants u6m
from LICs and LMICs. Burden of acute malnutrition in u6m infants
in LICs and LMICs is very high, especially in South Asia region. Risk
factors identified in the review were mainly maternal related and
MNS component along with BF support is identified as an effective
strategy to prevent growth faltering in u6m infants. The review also
identified that there is paucity in current evidence on assessment and
management of acute malnutrition in u6m infants.
In addition, further research on context specific burden of acute
malnutrition and identification of underlying risk factors, can help
shaping new programs and/ or in incorporating u6m in existing
malnutrition management strategies.
Acknowledgements
We would like to acknowledge the team of Eppi Reviewer and
EndNote for their support.
References
Citation
Sirwani B, Misra H, Shivani C, Rana R. Assessment and Management of Acute Malnutrition in Infants Under Six Months: A Systematic Review. Indian J Nutri. 2021;8(3): 240.