Research Article
Nutritional Status of Camel Milk Consumers in Bikaner District of Rajasthan, India
Soni V1,2*, Singh G3,4 and Goyal M1
1Department of Food and Nutrition, College of Home Science, India
2Sri Jain Kanya PG Mahavidyalaya, Bidasar Bari, India
3Department of Biochemistry, College of Agriculture, SKRAU, India
4Vice Chancellor, Madhav University, Abu Road, India
*Corresponding author:
Singh G, Vice Chancellor, Madhav University, Rajasthan, India, Tel: 91-9414429766; Email:
govindsingh10@rediffmail.com
Article Information: Submission: 09/07/2021; Accepted: 10/08/2021; Published: 12/08/2021
Copyright: © 2021 Soni V, et al. This is an open access article distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
In present investigation nutritional profile of 100 camel milk consumers and 100 non camel milk consumers in the same age group (30-50yr.) residing in
similar rural area of Bikaner District of Rajasthan, India was assessed. All the subjects surveyed were interviewed on the basis of purposive sampling to find out
their nutritional status. Consumption of camel milk was found to be highest (100 percent) by the adults and elderly. All the subjects were consuming camel milk
due to its easy availability, therapeutic values and traditional household practice. Both the groups were assessed for Clinical, Dietary intake and Anthropometric
measurement. Significant gender difference was observed in camel milk intake in both the groups.
Keywords
Camel milk; Nutrition; Dietary Requirement; Milk consumers
Introduction
Camel as a livestock plays an important role in desert ecosystem
and its milk has potential contribution in human nutrition in the
hot and arid regions of the world. This milk contains all the essential
nutrients as found in other milk. Fresh and fermented camel milk
has been used in different regions in the world including India and
Russia for human consumption as well as for treatment of a series of
diseases.
Camel milk is used extensively within a variety of populations for
its proposed healing properties and disease prevention mechanisms
[1]. Some of the more common indications associated with its use
include diabetes, allergies, immune disorders, and cancer [2,3]. It
is also advocated as an alternative to cow’s milk for those who are
allergic or intolerant to cow milk proteins [4]. In the last few years,
awareness about nutritional and medicinal benefits of camel milk has
rapidly increased [5]. Consequently, the demand of the product has
also increased.
Camel has always been the symbol of India’s state of Rajasthan
and traditionally represents the lifeline of the rural population. The
camel possesses a huge productive potential. It is a multi- purpose
animal and, unlike any other domesticated animal, has been utilized
by humans for centuries for transport, traction power, milk, meat,
skin and fuel.
In India camel milk is being used since long by the camel keepers
for the preparation of traditional milk products such as local sweets
(Kheer, Ghevar), Tea, Coffee and raw or boiled milk for drinking
purpose in rural arid areas. Rajasthan is a state where due to extreme
hot environment and scarcity of water, conditions do not support the
dairy cow, hence camel milk can play a very important role in the diet
of the people living in this state.
Although various studies have been conducted on the nutritional
status of different age groups with different criteria but information
regarding the nutritional status of camel milk consumers is lacking
in the literature. People in Bikaner district also represent a definite social sector with different food habits which in turn might affect their
nutritional status. Similar may be the case for camel milk consumers.
Therefore, the aim of the study is to study the nutritional status of
milk consumers in nearby areas in Bikaner District of Rajasthan.
Materials and Methods
The present study was conducted in nearby villages of Bikaner
district of Rajasthan, selected on the basis of existing camel population.
Community was surveyed to explore consumption pattern of camel
milk and its impact on their nutritional and health status.
Accordingly, a survey was conducted on consumers of camel
milk (experimental group subjects n=100) and those who do not
consume camel milk (control group subjects n=100) but all residing
in the same village. Further the male and female subjects were equally
represented in both the groups. A structured interview schedule was
developed to collect information about different aspects of camel
milk consumption from both the groups.
Other information about the camel milk, like total availability
of milk, seasonal availability, reasons for consuming and not
consuming, preference for it in the family, frequency of consumption,
and types of camel milk processed products and its therapeutic value
as obtained from the experimental group i.e. camel milk consumers
was also collected. However, the control group i.e. non consumers
of camel milk were also asked for their reasons for not consuming it.
Each such aspect is dealt separately as follows.
Survey of the community:
Camel rearing community “Riakas” residing in nearby villages
like Bhamatsar, Gadhwala, Kanasar, Morkhana, Palana and Udasar
of Bikaner district were visited frequently to explore the camel milk
consumers. A list of regular camel milk consumers in the age group
of 30-50 years was prepared, since occurrence of the most of the noncommunicable
chronic diseases is common after 40 years of the age
[6]. A sample of 100 subjects of regular camel milk consumers from
the list was selected randomly [7]. Similar number of non-camel milk
consumers in the same age group residing in similar rural areas was
also identified to serve as control subjects. The experimental and
control subjects were then contacted and interviewed to explore
the consumption pattern of camel milk and their nutritional status.
Subjects’ interest and their willingness to cooperate in the study were
considered prior to their selection.Data collection
General information about the subjects:
This included information regarding their name, age, sex,
education, address, food habits, types of family, total income, activity
pattern, health status and availability of camel milk. Age of the
respondents was defined as the number of years completed by the
respondents at the time of interview. Age range of the respondents
was between 30-50 years.The type of family i.e. joint or nuclear was noted. According to
Bhushan and Sachdeva [8], a family is which consist of husband, wife
or wives and their children are called nuclear family. The children
leave the parental household as soon as they are married. A nuclear family is an autonomous unit free from the control of the elders while
joint family is viewed as a merger of several nuclear families. Thus
a small joint family may include an old man and his wife, their son,
son’s wife and their children. There are two nuclear families and the
son being a member of both families.
Occupation and Income:
Occupation is any kind of job the respondents were doing as their
earning sources and were noted for all their family members.Income was assessed as total earning in terms of money during
a specific period of time. In the present study income from other
sources like agriculture, poultry, house rent, interest etc. was also
noted. On the basis of the total family income the selected subjects
were classified into three different economic groups i.e. Lower
Income Group (LIG) having income less then Rs.12,000, Medium
Income Group (MIG) having income Rs. 12,000 to Rs.20,000 and
High Income Gruop (HIG) having income more than Rs.20,000 as
per norms given by Govt. of Rajasthan, Urban Development.
Consumption pattern of camel milk:
To gather information about consumption pattern of camel milk
following questions were asked to each of the subjects:Questions related to various methods of using camel milk and its
value addition.
a. Questions seeking answer about reason for consuming camel
milk including its therapeutic values.
b. Questions seeking information about the effect of consuming
camel milk on their health as perceived by them.
c. Question seeking information about reason for non
consumption of camel milk.
Nutritional and health status of the subjects:
Nutritional and health status of the experimental and control
subjects were assessed by Dietary intake, Anthropometric
measurement, and Clinical assessment.Dietary intake:
To find out dietary status, the food intake of all the selected
subjects of the study was assessed by following method:The food intake of the subjects was assessed by 24 hours recall
method for three consecutive days using standardized food cup set.
Raw quantity taken for cooking as well as cooked quantity prepared
especially for the subjects or for the whole family and consumed by
the subject was recorded to find out the quantum of raw food intake.
Raw and cooked amount were quantified either in terms of house
hold measures (standardized cup set) by weight or number. From this
cooked and raw amount consumed by each subject was calculated
and food adequacy was determined by using the following formula:

In this formula suggested intake is the recommended dose of daily
allowances (RDA) by ICMR. Intake of various foods consumed by the
subjects was estimated and food frequency ratio was calculated then compared with that of the balanced diet as given by ICMR (2010) for
moderate working adults.
Anthropometric measurement: It provides information on
gross body size, skeletal form or configuration and on skeletal and
soft tissue development. These measurements are non invasive,
inexpensive, universally acceptable and can reflect nutritional and
health status. Each of the subjects was assessed for the height, weight,
waist circumference and hip circumference to find out their Body
Mass Index [9] and Waist Hip Ratio [10].
Clinical examination: It is an important practical method for
assessing the nutritional status of a community. This method is based
on examination for changes related to inadequate nutrition which
can be seen, felt is superficial epithelial tissues, especially the skin,
eye, hair and buccal mucosa, or in organs near the surface of body
such as the parotids and thyroid glands.
Statistical Analysis
Observations collected on the various aspects of the study have
been statistically analyzed as suggested by Gupta [7].
Results & Discussion
Information about community survey:
A community survey of 100 households associated with camel
rearing in the villages of Gadhwala, Bhamatsar, Udasar, Sainsar,
Palana, Morkhana and Kanasar in Bikaner district was carried out
to gather information about the pattern of consuming camel milk.
Similar numbers of the non-consumers of camel milk from same
villages were also surveyed.Among these villages Ghadwala village was an important study
point. Since the village harbors maximum number of the she camels as
well as the inhabitants of the village had preference for consumption
of camel milk. The village is dominated by community of Raika who
are known to rear camel either for milk or for transport purpose. The
total camel milk production in the village is about 100-120 kg per day.
Following aspects were dealt with while conducting the survey:
General information about the subjects:
The general information of the subjects of control and
experimental groups about their age, sex, type of family and family
income was collected (Table 1).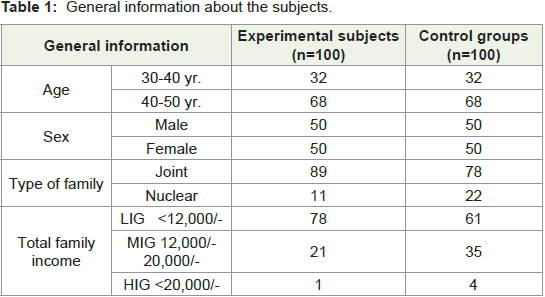
The selected subjects were aging between 30-50 years. Perusal
of data reveals that the majority of cases (68 percent) who consume
camel milk belonged to age group 41-50 years, followed by 31-40
years (32 percent). Same age groups of the non-consumers (control
group) were also surveyed. The results illustrate that the camel
milk is preferred by old aged persons as compared to their younger
counterparts.
Specific information about consumption of camel milk:
Each such aspect about camel milk consumption is dealt
separately as follows.Availability of camel milk: The information about the total
availability of camel and camel milk was obtained from the
respondents of the identified village (Gadhwala).
Perusal of data reveals that the total number of camels available
in the studied villages was 316 of which she camels were only 185.
Further analysis of data reveals that only 80 she camels were in the
lactation state in the villages and an average yield of camel milk per
day per camel was 6 litres.
Seasonal availability of camel milk: Information about the
seasonal availability of camel milk was gathered and is presented in
Figure 1.
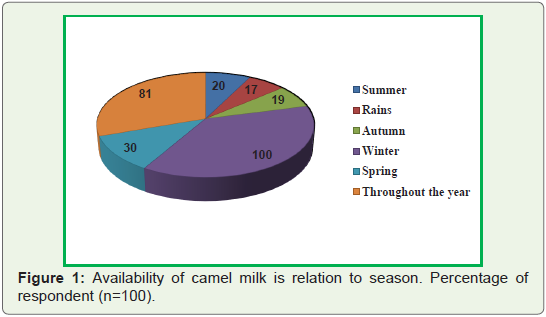
The seasonal availability of milk from her camel seems to be
controlled by the availability of feed and fodder and its seasonal
nature of breeding [13].
Reasons for consuming camel milk: While inquiring about
reasons for consuming camel milk, all of the subjects reported
about its therapeutic values, traditional/ household practice, easy
availability and its good taste. The other factors favoring camel milk
consumption included its high nutritive value (70 percent) and low
cost (68 percent) (Figure 2).
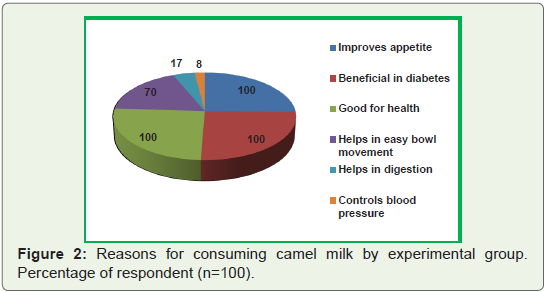
All the respondents (100 percent) reported that camel milk is
useful in improving the appetite, helps in maintaining good health
and useful in diabetes. Majority of the respondents (70 percent) were
of the opinion that camel milk helps in the bowl movement but only 17 percent and 8 percent of them reported that camel milk is useful
in digestion and control of blood pressure, respectively. Yet 5 percent
also were of opinion that it is beneficial in preventing liver diseases.
The result clearly reveals that as per consumer’s belief camel milk
bears good therapeutic value.
Therapeutic value of camel milk as perceived by the subjects: During the survey the respondents were also asked about their
knowledge about therapeutic value of camel milk. The data thus
generated is presented in Figure 3.
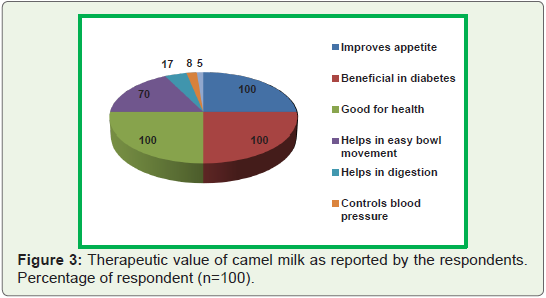
According to data, all the respondents (100 percent) reported that
camel milk is useful in improving the appetite, helps in maintaining
good health and useful in diabetes. Majority of the respondents
(70 percent) were of the opinion that camel milk helps in the bowl
movement but only 17 percent and 8 percent of them reported that
camel milk is useful in digestion and control of blood pressure,
respectively. Yet 5 percent also were of opinion that it is beneficial
in preventing liver diseases. The result clearly reveals that as per
consumer’s belief camel milk bears good therapeutic value.
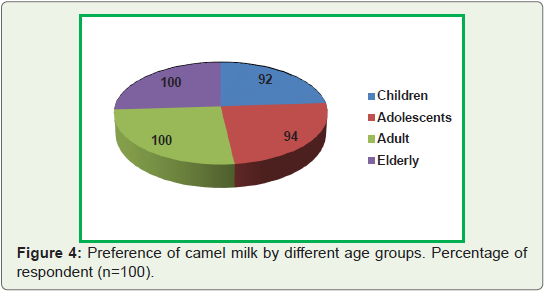
Preference for camel milk in the family: The subjects were
interviewed about their preference for camel milk in their families.
Highest consumption of camel milk was found among adults and
elderly (100 percent) followed by adolescent (94 percent) and children
(92 percent).
It was evident from the present study that adults and elderly
members of the community preferred to take camel milk as compared
to their younger counterparts (Figure 4). This may be because of their
traditional practice of consuming camel milk and secondly they might
be aware of the therapeutic value of the camel milk. Osman [14] has conducted study on utilization of camel milk by milk consumers
in Sudan and observed that the majority of owners consumed the
produced milk, while few of them sold the produced milk and took
the milk for calves.
Frequency of consumption of camel milk: The subjects of study
group were interviewed for the frequency of consumption of camel
milk. All the camel milk consumers reported that they consume
camel milk daily in its fresh form i.e. without boiling although the
preference depended on their age groups.
Forms of using camel milk: The form of using camel milk and its
types of processed products being utilized in diet of the subjects were
surveyed. All the households studied were found to be utilizing camel
milk either in the form of fresh milk or in processed form or both.
It has been observed that the camel milk was found to be processed
for preparing various products viz tea (100 percent of subjects), kheer
(100 percent of the subjects) and raabri (100 percent of the subjects).
None of the household utilized camel milk in the form of khoa, curd,
ice cream and paneer or other forms of value added products.
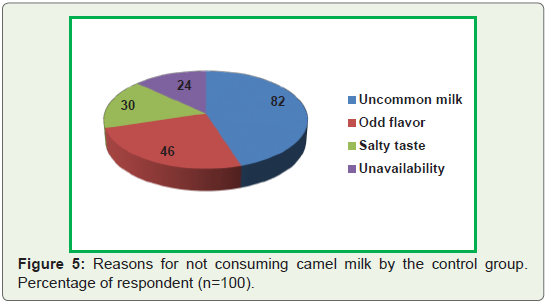
Reasons for not consuming camel milk: The respondents of
control group who do not consume camel milk were interviewed
for the reasons of their non consumption. “Uncommonness of
camel milk” was the reason reported by majority of the (82 percent)
respondents. This was followed by “odd flavor” which was reported
by 46 percent of the subjects. The other reasons like “salty taste” and
“unavailability” was reported by 30 percent and 24 percent of the
respondents, respectively (Figure 5).
Assessment of nutritional status of the subjects:
Nutritional status refers to the health of an individual as it
is affected by the intake and utilization of nutrients [15]. Thus
nutritional status of the subjects was evaluated by assessing their
dietary, anthropometric and clinical status.Dietary assessment: The food habits of the subjects was evaluated
and it was found that irrespective of age and sex, all respondents from
experimental and control groups were vegetarian.
However, besides economic status, the type of menu incorporated
for the day’s meal was depended upon individuals like and dislike,
food habits, food availability and family food pattern.
Nutrition is the most vital component of life that is to be taken
care of by all individuals to maintain their body structure and energy
levels for day to day activities. During adult age, balanced amount of
nutrients are needed to support the development as well as to meet
the balanced basal metabolic rate [16].
The dietary adequacy of the subjects under present study was
assessed by calculating the amount of various foods and compared
with balanced diet suggested by ICMR [17,18]. The relevant results
are presented in Table 2&3.

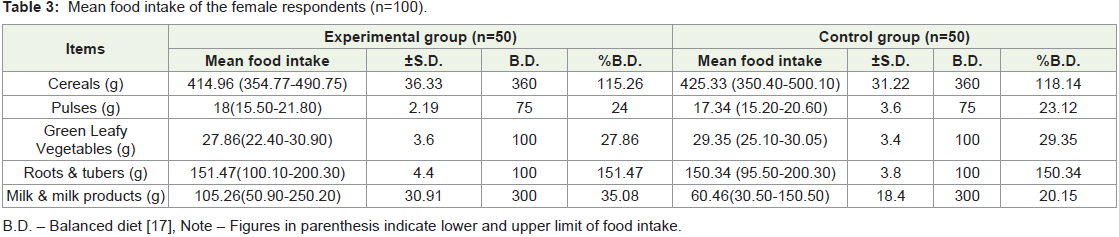
Among male and female subjects, mean cereal intake of
experimental group as well as control group was significantly higher
than the balanced diet recommended by ICMR [17] while in pulses
it was noted to be lower in both experimental and control groups as
compared to balanced diet recommended by ICMR [18] in male and
female subjects. All subjects were not fulfilling the requirement of
recommended value for pulses in their diets.
Mean intake of green leafy vegetable was apparently very low
by the male and female subjects of both the groups as compared
to the value suggested in balanced diet. The lower intake of green
leafy vegetable by the subjects of present study in Thar area may be
due to unavailability, food preferences and unawareness about its
importance. Similar finding were noted by Paul and Purushothman
[19] while conducting study on dietary intake of LIG subjects under
their study.
In the present study potato, onion and radish were the most
commonly consumed roots and tubers in the form of vegetables and
salad by the subjects in both the groups.
Another group covers liquid milk, milk powder, fermented
products like curd, butter milk etc. Milk has a unique place in any
balanced diet particularly in a vegetarian diet to provide good quality
protein, sufficient calcium and riboflavin, which are difficult to obtain
in adequate quantities solely from plant foods [17]. According to
Ostman et al [20] milk and milk products tend to lower post prandial
glucose level and fermented milk and milk products are more
beneficial in maintaining blood glucose level.
A vast difference occurred in milk intake at two levels. Firstly a
clear gender difference is visible in the milk intake by both the groups.
Since, the female subjects of control and experimental groups were
consuming only 60.46 ml to 105.26 ml of milk per day as compared
to their male counterparts who were having 100.6ml to 250.62 ml of
milk each day. Moreover at the time of survey it was also observed
that most of the milk consumed by the female subject was in the form
of tea and buttermilk.
Similarly the difference in milk intake was also observed when it
was compared between males of both the groups. The male subjects
of experimental group were consuming quite good amount of milk
(250.62ml/day) than that of the males belonging to control group
(100.6ml/ day). This must be due to ready to use availability of camel
milk in their houses for experimental group. It was also reported by
camel breeders that camel milk available with them is not allowed
to be sold in the market as per their religion. This might have led to
higher consumption of camel milk within their family. The interest
for camel rearing and production is increasing strongly for the last
20 years in many countries, including Western countries where the
camel is newly implemented. As example, the implementation of
camel dairy farms in Netherland, Italy, USA or even in Australia
testifies the growing enthusiasm for the camel products, especially
milk [21].
Immaterial of gender and types of group overall view of food
intake indicates that the diets of all the subjects was grossly lacking
in important food groups like pulses, green leafy vegetables and
milk. Whereas, energy and carbohydrate rich foods like cereals were
found to be consumed in more than the required amounts. Gopalan
et al [22] have reported that in rural areas, a normal adult person
consumes 446 g cereals/millets, 32 g pulses, 10 g green leafy vegetable,
48 g other vegetables, 70 g milk, 11 g fish and such foods etc.
Anthropometric assessment: Anthropometric measurement is
an important method assessing the nutritional status of the subjects
as these measurements are partially dependent upon nutrient intake.
Therefore, in present study weight, height, waist circumference and
hip circumference of all subjects were measured and then Body Mass
Index (BMI) as well as Waist Hip Ratio (WHR) of the subjects was
assessed using pertinent standards as mentioned in methodology.
Height
During present study the mean height of male and female subjects
of control and experimental groups was measured to be 176.34 cm
and 176.32 cm, 158.68 cm and 158.60 cm, ,respectively and the values
were in tune with the reference values of Indian man (173 cm) and
woman (161 cm) given by ICMR [17]. The difference between the
height of control and experimental subjects of both the genders was
found to be non significant.
In contrast to the present results, Banerjee et al [23] reported
evidence of lower weight (79-95 percent) and height (81-97 percent)
than the given standards in their investigations on male and female
subjects of various age groups.
Weight
Body weight is most widely used and the simplest reproducible
anthropometric measurement for the evaluation of nutritional status of the subjects. It indicates the body mass and is a composite of all
body constituents like water, minerals, fat, protein, bone etc. for
screening short term malnutrition at a high level of specificity, weight
for height is superior to weight for ages [24]. Difference in the weight
measurement of both the categories of control and experimental
groups between male and female subjects were found to be non
significant. It may also be perceived from the table that weight of all
the subjects was approximately near to the reference values. It must
be due to their moderately active life style as well as almost balanced
energy intake.
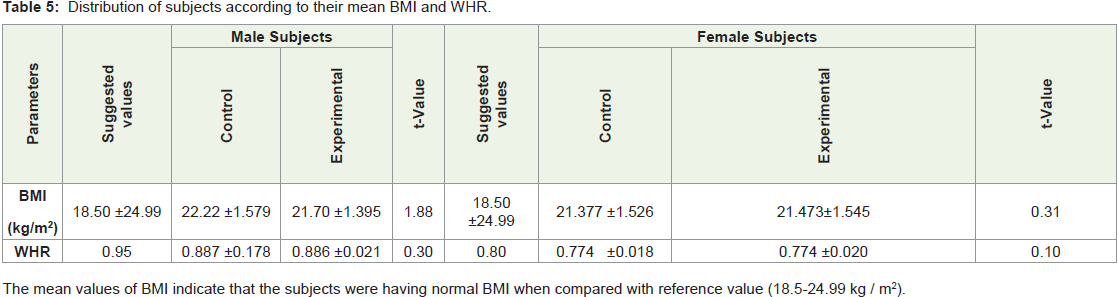
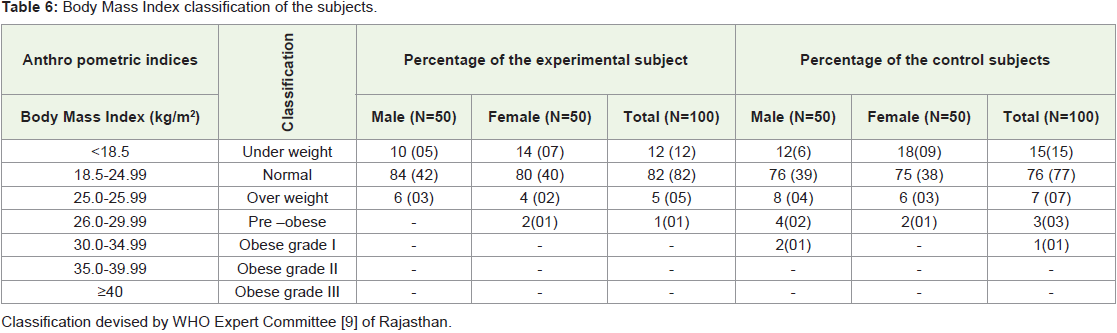
Body Mass Index (BMI):
BMI provides a reasonable indication of the nutritional status of
adults. The BMI has good correlation with fatness. It may be used as
an indicator of chronic energy deficiency as well as obesity [25].None of the subjects were found to be in obese grade III and II
categories. Similar evidence of BMI was observed by [26,27] during
their investigations on adult male and female subjects. It is important
to note that majority of the subjects (77- 83 percent) in both the
groups were belonging to normal BMI category. This must be due to
their better intake of energy and protein rich foods in their diet.
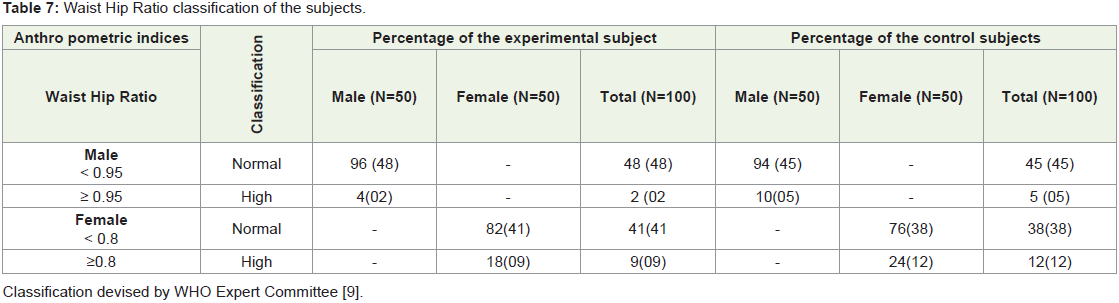
Waist Hip Ratio (WHR):
The distribution of excess adipose tissue profoundly affects its role
as a risk factor for Cardio Vascular Disease (CVD). Specially, excess
of truncal and intra-abdominal fat (central obesity) have important
adverse influence on lipid levels, blood pressure, glucose tolerance
and is in fact risk factor for coronary disease [28,29].The mean WHR of the male subjects belonging to control and
experimental category was noted to be 0.887 and 0.886, respectively
(Table 5,6). Similarly the values were noted to be 0.774 for their female
counterparts against 0.80 as reference value. The difference between the male and the female subjects of both the categories was found to
be non significant. The data regarding WHR measurement of all the
subjects also indicate that they had slightly lower mean WHR when
compared with the reference values. Agarwal et al, [30] also have
reported approximately similar WHR values (0.85 and 0.88) for male
and female rural adults of Rajasthan.
When subjects were classified according to their categories of
WHR (Table 7,8) it indicates that majority of the subjects were falling
in normal category but few of them had high waist hip ratio.
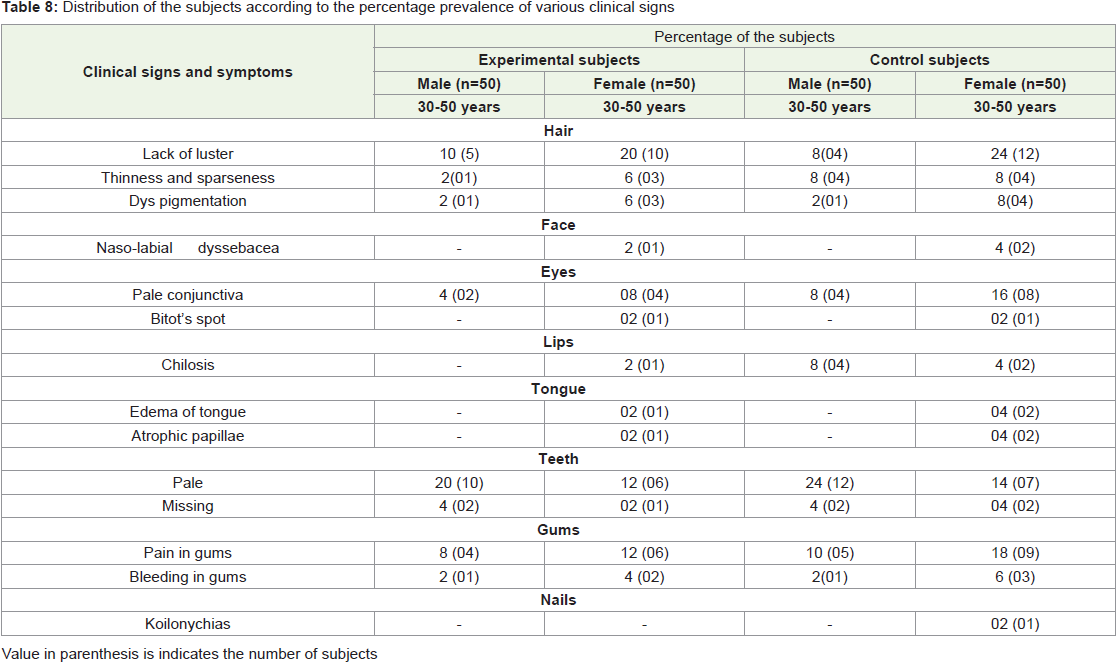
Clinical examination of the subjects
Clinical examination is an important method of assessing the
nutritional status of community. In this, the subjects were examined
for change in the appearance related to inadequate nutrition. The
clinical signs observed were interpreted as the schedule suggested by
Jelliffe [11].
No significant difference was observed of clinical signs in both
the groups under study compared with earlier drought survey of
Jodhpur district, it was observed that prevalence of various signs
related to protein calorie malnutrition, prevalence of anemia, vitamin
A, vitamin C deficiency and B complex deficiency was observed to be
also higher in that area [31].
In summary, nutritional profile of milk consumers and non
camel milk consumers was assessed in present investigation. Most of
the subjects were from joint family. Average yield of camel milk per
day was found to be 6 liter. Consumption of camel milk was found to
be highest by the adults and elderly. All the subjects were consuming
camel milk due to its easy availability, therapeutic values and
traditional household practice. Finding of food intake it was noted
that pulses, green leafy vegetables and milk and milk products were
inadequately consumed by all the subjects, whereas consumption of
cereals, roots and tubers were noted to be in adequate when compared
with suggested intake given by ICMR [18].
References
Citation
Soni V, Singh G, Goyal M. Nutritional Status of Camel Milk Consumers in Bikaner District of Rajasthan, India. Indian J Nutri. 2021;8(3): 238.