Research Article
To Study Knowledge, Attitude and Practices (KAP) of Mothers of Children (1-59 Months) Admitted with Severe Acute Malnutrition (SAM) Regarding Feeding and Prevention of Malnutrition
Tahilramani G1*, Meena RK2 and Mathur A3
1Nutritionist- National Health Mission, NRC - Department of Pediatrics, Hindu Rao Hospital, New Delhi, India
2Department of Pediatrics, University College of Medical Sciences >B, Dilshad Garden, New Delhi, India
3Department of Pediatrics, Hindu Rao Hospital, New Delhi, India
*Corresponding author: Tahilramani G, Nutritionist- National Health Mission, NRC - Department of Pediatrics, Hindu Rao
Hospital, New Delhi, India Email: geet.tahilramani@gmail.com
Article Information: Submission: 08/05/2021; Accepted: 10/06/2021; Published: 12/06/2021
Copyright: © 2021 Tahilramani G, et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
The first 1000 days of a child’s life are considered to be the most vital (beginning from conception to 2nd birthday) for the health, happiness & survival of
child. Knowledge of mothers has an important role in the maintenance of nutritional status of the children. Only knowledge is not sufficient but having attitude
is also important to put it into practice.
Objective: To evaluate knowledge, attitude and practices (KAP) of mothers of under-five children having Severe Acute Malnutrition (SAM) regarding
antenatal care, IYCF practices and associated preventive factors for malnutrition.
Materials and Methods: Type of study: Cross sectional descriptive study.
Study period: April 2018 to October 2018.
Study population-Mothers/primary caregiver of the children admitted at Nutrition Rehabilitation Centre (NRC) of Pediatrics department of a teaching
hospital having SAM with medical complication / no medical complication that consented for participation.
Method: Mothers/primary caregiver were interviewed on various aspects of child care using a predesigned Performa KAP were assessed related to
Antenatal care, IYCF practices, Malnutrition. These were analyzed on excel programme.
Results: Total 65 mothers/primary caregivers of children with average age 15 months and 41.5% female participated. Mothers had fair KAP about
antenatal visits required, medication required in antenatal period and place of delivery. The same applies for growth monitoring and immunization.
Knowledge and attitude regarding breast feeding are fair but practices are still very low. For complementary feeding and underlying factors for malnutrition
not only knowledge and practice is low but attitude is also poor.
Conclusion: Awareness of mothers regarding ANC, growth of child and immunization is fair and still needs to be improved to get desired levels of good practices.
We need to have a community based strong IYCF programme emphasizing on the knowledge of mothers on this important child care aspect and
counselling of mothers to improve their knowledge and practices with change of attitude.
Their stay in NRC should also be used to improve their knowledge and attitude to have better practices. This will go in a long way to prevent and treat
malnutrition which is a major threat country is facing.
Keywords
KAP; SAM; ANC; Maternal Knowledge; IYCF practicesṣ
Abbreviations
ANC: Antenatal Care; EBF: Exclusive Breast Feeding; HRH:
Hindu Rao Hospital, IYCF: Infant & Young Child Feeding;
KAP: Knowledge, Attitude & Practice; MUAC: Mid Upper Arm
Circumference; NFHS: National Family & Health Survey; NRC:
Nutrition Rehabilitation Centre; SAM: Severe Acute Malnutrition;
SAMTU: Severe Acute Malnutrition Treatment Unit; LAMA: Left
Against Medical Advice
Introduction
A Nation’s health depends on the healthy citizen. A healthy adult
emerges from a healthy child [1]. Appropriate nutrition during the
1,000-day window period, between the start of a woman’s pregnancy
and child’s second birthday, is critical to the future health, wellbeing,
and success of any child [2]. Although India has not yet overcome
the problems of poverty, under nutrition and communicable diseases,
it is increasingly facing additional challenges related to the affluence
that results from industrialization, urbanization and economic
betterment. Over the last two decades, over nutrition and obesity
have emerged as public health problems. Therefore, India at present
is facing challenge of double burden of malnutrition [3]. The effect of
malnutrition on child’s development is at multiple levels. Optimum
nutritional status is every child’s right.
Malnutrition refers to deficiencies, excesses or imbalances in a
person’s intake of energy and/or nutrients. The term malnutrition
covers 2 broad groups of conditions. One is ‘under nutrition’ which
includes stunting (low height for age), wasting (low weight for height),
underweight (low weight for age) and micronutrient deficiencies or
insufficiencies (a lack of important vitamins and minerals). The other
is overweight, obesity and diet-related non communicable diseases
(such as heart disease, stroke, diabetes and cancer) [4]. Malnutrition
is a very complex phenomenon with numerous causes, manifestations
and is intergenerational. Like an iceberg, it affects the community
both directly as nutritional deficiency diseases and indirectly by
leading to high morbidity and mortality among young children [2].
Severe acute malnutrition is defined by very low weight-forheight/
length (Z- score below -3 SD of the median WHO child growth
standards), and / or a mid-upper arm circumference < 115 mm, and
/ or by the presence of nutritional edema (B/L pitting oedema ruling
out other causes of (oedema). Prevalence of SAM in India is 7.5% as
per NFSH-4 and in Delhi it is reported to be 5% [5]. The prevalence
of SAM among the admitted cases is as high as 18.5% as was reported
by Mathur et, al. [6].
Causes of acute malnutrition include inadequate food intake,
incorrect feeding practices, disease and infection or more frequently,
a combination of these factors [7]. It is not only the food insecurity
but the knowledge of mother regarding various aspects of child care
like taking care of herself during antenatal period, IYCF practices,
Family planning and immunization are very important along with
her attitude towards these and her ultimately practices.
There is a dearth of studies to assess the KAP of mothers/
caregivers of SAM children, relating to the above subjects. This
study deals with mothers of medically complicated cases which were
admitted in ward & treated in NRC of the study site.
Material and Methods
Site of Study: The present study was conducted in the Department
of Pediatrics, Hindu Rao Hospital and North DMC Medical college
of Delhi.
Study Design: Hospital based Cross Sectional study.
Duration of study: 22 April 2018 to 15 October 2018. (6-month
period).
Sample Size: The study was conducted on a sample size of
65 mothers/caregivers of children admitted with Severe Acute
Malnutrition. It was conducted in a face-to-face interview style, which
took about 20-25 minutes to complete. It included a written consent
signed by the mother / caregiver in the language understood by them.
Inclusion criteria:
Mothers/ caregiver of any child (aged 6 months to 5 year) admitted
and diagnosed with SAM as co-morbidity by any of following criteria
as per WHO and GOI guidelines [8].● Weight for Height <- 3SD
● Mid Upper Arm Circumference (MUAC) <11.5cm.
● B/L pitting pedal edema
Exclusion criteria:
1. Parents/caretaker who refused for consent.
2. LAMA before 24 hours of admission before study could be done.
3. Mothers /caregiver (2) with huge language barrier.A predesigned and pretested Performa was used and information
was collected from the participants i.e. mothers / primary care givers
of the admitted children with SAM. The questionnaire was designed to
assess the Knowledge, Attitude & Practices of participants (mothers/
caregivers) of admitted SAM cases on following subjects as according
to the literature available these points are the most vital ones for the
optimum growth & development of the child:
● Antenatal Care
● IYCF practices
● Immunization
● Malnutrition and its prevention (Table 1).
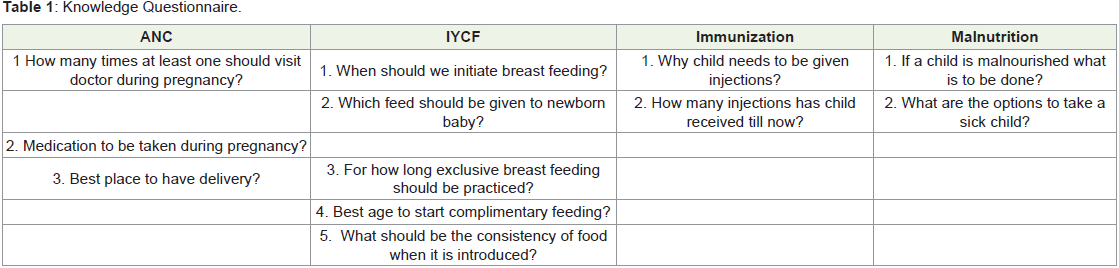
Each section had three to four questions related to the topic. Each
question was framed in three different ways to get the information
about their knowledge, attitude and what they have practiced and /or
practicing. For all the respondents not doing appropriate practice, we
tried to find reason as well.
All the data was stored & analyzed in Microsoft excel; Summations
& percentages used for descriptive analysis & interpretation of the
collected data. For categorization of scores to assess the KAP, out of
the entire mother’s cohort (Table 2):

Results
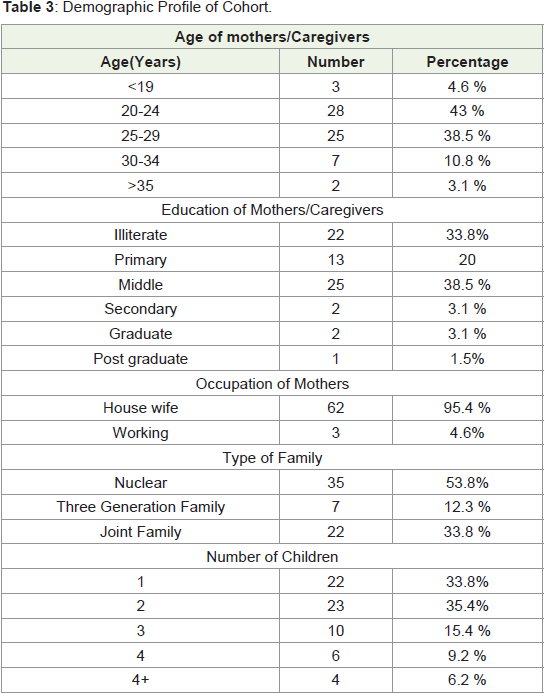
Total 65 mothers / caregivers agreed to participate in the study.
97% (n=63) of respondents were mothers while 3% (n=2) participants
were primary caregiver. The average age of child in the group was 15
months with 41.5% (n=27) were females.
In the cohort 41.5% had monthly income Rs 6431 to 10718 and
36.8% had above 10718. 4 had above Rs 21438.
In 95.4% (n=62) cases had toilet facilities whereas 4.6% (n =3)
responders had to defecate in open areas (Table 3) and (Table 4).
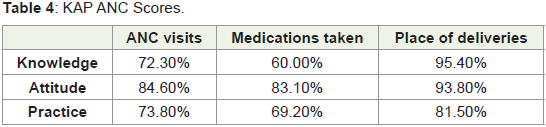
The first segment of the questionnaire dealt with the Antenatal
care.
72 .3% had knowledge that there should be 4 or more visits
and 73.8% actually did so many visits. Attitude was even in higher
percentage of mothers (84.6%) for antenatal visits so if knowledge
is improved by group and one to one counselling ANC visits can be
improved.
Reasons for having less than 4 visits in those 17 cases on top
were, they did not get enough time 4 cases, with other reasons family
pressure (3) & facility far off in 2 cases. 7 cases did not have any
specific reason.
There were approximately 83.1% felt that there should be need for
taking medications during pregnancy understanding that there must
be need to take them but only 60.0% had requisite knowledge and
69.2% completed the medications. Rest did not take medications as
recommended as they or family was not convinced topped the reason
in 20 defaulters and 6 could not specify the reasons.
Institutional deliveries were in 81.5% cases only though 93.8%
were convinced that it should be in health facility. Among those who
had home deliveries 66.8% could not reach hospital on time.
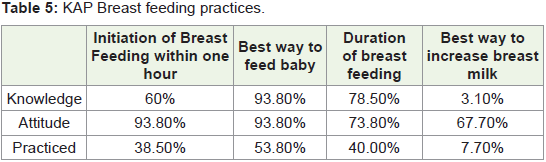
In the second set of questions information was gathered on IYCF
practices. The data showed that timely initiation of breast feeding is
only in 38.5% cases despite 60% had the knowledge that initiation
should be done within one hour and very high percentage convinced
and have attitude for early initiation.
In this cohort of 40 mothers who could not initiate breast feeding
within one hour 37.5% reason was that baby was not with mother and
47.5% could not respond /specify any reason for delayed initiation.
A mother have the knowledge that breastfeeding is best for the
babies and wants to do that also still only 53.8% could breastfeed the
babies exclusively for required period. Top most reason for switching
to mixed feed was not enough breast milk.
63.3% mothers had introduced top milk for this reason. Very high
percentage 23.3% could not give any specific reason.
78.5% had good knowledge of duration for which exclusive breast
feeding is to be given, 73.8% had attitude for it as well but only 40%
practiced it. The reason for knowledge and attitude not converting
into practice was not enough milk in 48.7% and very high percentage
out of these 39 cases 41% there could not attribute to any specific
reason.
Questions related to the best way to increase breast milk were
asked too but only one responded that it can be increased by only two
gave importance to sucking by the baby to increase milk supply. 29.2%
had no idea and 55.4% feels only mothers’ diet helpful .67.7% feels
that breast milk supply can be increased. Only 5 mothers consulted
the doctors to increase for not enough milk (Table 5).
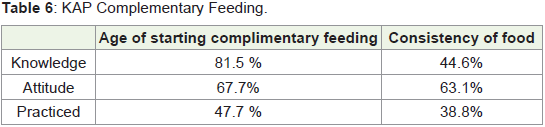
The next segment of the questionnaire dealt with the
complementary feeding. The data shows that only 81.5% had the
knowledge regarding the age of starting complementary feeding &
67.7% had the attitude for the same. But only 47.7% practiced it.
41.1% had no specific reason for not starting.
Only 44.6% have knowledge that consistency of food is important
and still lower 38.8% gives food of right consistency.35.4 have given
thin food most of the time and rest have not taken care of consistency
any time. Mostly (30 out of 43) had no specific reason for giving food
of not right consistency (Table 6) and (Table 7).
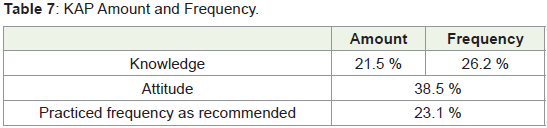
Knowledge regarding amount to be given and how frequently
is very poor. Only 21.5% had knowledge about the quantity and
only 26. 2% about how frequently child needs to be feed. There is
lack of attitude also. Only 38.5% responded that they will try or were
confident that child will take. Only 23.1% were giving as frequently
as required. Main reasons specified were that they were not aware
that child needs to be given so much in 26% cases and equally felt
that child will not be able take this much. A big percentage of them
42% could not specify any reason. None of the mother said that they are not giving this much amount and frequently due to financial
constraint and except one none gave the reason as constraint of time.
Malnutrition:
Mother’s have very poor knowledge regarding the causes
associated with malnutrition & they do not do anything special to
prevent malnutrition in the child without having any specific reason
for this. A big number had no idea about the causes of malnutrition
that 20 out of 65 i.e. 30.7%. 23% of the respondents know that both
feeding and underlying disease /repeated infections are the causes
of malnutrition. Feeding alone was felt as a cause of malnutrition by
29.2% and 15.3% attributed it only to infections. The mothers admit
in 37% cases that they did not do anything to prevent malnutrition
in this child. 63.1% had no reason for not taking special efforts to
prevent malnutrition.Immunization:
Results of immunization were quite positive with 87.6% having
knowledge about importance of immunization & 80% immunization
is updated and another 14% had partially immunized this child
(Figure 1).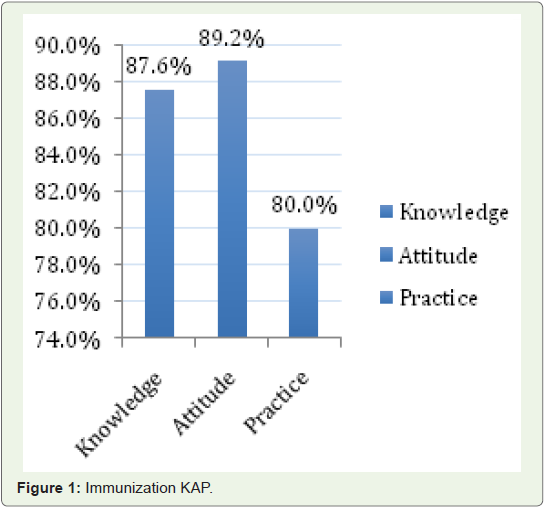
Discussion
In the current study we found that the knowledge of the mothers
/ primary caregiver for antenatal care including visits and place of
delivery is fair. Out of 65 participants 73.8% had 4 or more antenatal
visits which are much more than the national average of 51.2% as per
NFHS- 4 data. Similar findings are there about the rate of institutional
deliveries, which is 81.5% compared to the 84.4% and 78.9% for Delhi
and national average respectively as per NFHS -4 [5].
In a recently published study from Ethiopia including 350
participants, the rates of antenatal visits and institutional deliveries
were 85.5% and 72.6% respectively [9].
During the period of pregnancy, a healthy and balanced diet
with an adequate intake of essential nutrients is important not only
for foetal development and birth outcome, but also for the mother’s
health.
Adequate calcium intake during pregnancy is of major importance
for the health of both mother and fetus. It was reported by Willemse
et, al. that calcium supplements were used by 64.8% of women [10].
Along with calcium supplements, Iron supplements are particularly
important for pregnant women who have anaemia. Demuth et, al.
reported that 65% of pregnant ladies consumed recommended iron
supplements [11].
In our study it was reported that only 50% were taking Iron Folic
Acid and Calcium tablets while7.6% (n=5) consumed only iron.
According to NFHS-4, 49.9% of pregnant females in Delhi consume
Iron & FA supplements while only 8.7% at the national level [5].
In this study 68.7% of respondents had completed the medication
course. Our data shows that if counselling is done to increase the
knowledge it will convert to practices as their attitude is positive in
much higher percentages.
The early initiation of breast feeding is the key factor for the
successful exclusive breast feeding. It plays a very vital role in
continuation & sustenance of breast feeding & practicing EBF for 6
months, which forms the basis of healthy development of the baby
by providing adequate amount of required nutrition, prevention of
the malnutrition state and development of bonding between mother
& baby.
Age appropriate and adequate feeding practices are the main
contributors to reducing morbidities and mortalities in under-five
children [12]. According to the WHO rating on early initiation of
breastfeeding; 0–29% is considered poor, 30–49% as fair, 50–89% as
good and 90–100% as very good [13].
In our study only 38.5% respondents practiced timely initiation of
breast feeding even though 50.7% had knowledge of it and 78.4% had
attitude. This shows that Knowledge and attitude both are there but
still practices are very low. According to NFHS- 4 the timely initiation
of breast-feeding rate is 29.1% in Delhi, whereas the national figures
are 41.6%. The study done by Manohar et, al. in Tirupati in India
about the factors responsible for delayed breastfeeding [14], They
had found that 60% of mothers knew that breastfeeding should be
initiated as early as possible after birth and increasing the knowledge
of patients will be beneficial for increasing breastfeeding rate further
along with change in health facility policies as they had found the
separation of mother and baby as the commonest reason for delayed
initiation.
In a study done by Fadare et, al. in Nigeria 76.1% respondents
practiced exclusive breast feeding [15]. Whereas, in a study done
by Dukuzumuremyi et, al. in East Africa only 55.9% respondents
actually practiced EBF in spite of the fact that 84.4% were aware of
EBF and its importance [16]. While the rates for India are 54.9% as
reported in NFHS-4.
This points to the fact that for improving breast feeding practices
not only improving knowledge will be helpful but supporting the
mother in other ways also.
Above 93% had knowledge & attitude for breastfeeding but only
53% were practicing exclusive breastfeeding. Not enough milk tops
the list of reasons for not practicing exclusive breastfeeding, found
in 67.1% of the mothers. Practically mothers do not have knowledge
that milk can be increased by correct positioning and attachment.
Practices of exclusive breast feeding and duration of breast feeding is
low despite knowledge and attitude in higher percentage.
Mothers have poor knowledge and practices about age of
starting and consistency of complementary feeding. The data for
India by NFHS suggests that only 8.7% children get age appropriate
complementary feeds while it was 34.3% in a study done by Zeleke et,
al. in Ethiopia [9]. Practically they have no idea about quantity and
frequency of feeding and leading to poor practices. As per national
data on complementary feeding complementary is started for 42.7%
at age of 6 months along with mothers giving breast milk.
Globally immunization of infants and young children against
various kinds of serious infectious diseases is among the most
successful and cost-effective interventions in preventative health care
[17].
Results of immunization in our study were very encouraging,
87.6% respondents had knowledge about it and 80% actually
practiced it. In a study done by Verulava et, al. 97% respondents had a
positive attitude towards immunization, whereas in our study 89.2%
respondents were quite positive with regards to vaccination As per
NFHS 4 [18], 62% of children below 2 years receive age appropriate
vaccinations while a study done in Bijapur by Angadi et, al. reported
the immunization rates to be 34.8% [19]. A study by Thiru kumar
& Kavin prasad in Chennai reported about 90% of parents have the
positive attitude towards immunization and 73% of parents have
good knowledge about Immunization [20].
Conclusion
Knowledge of mothers/ caregivers is better regarding antenatal
care and immunization than feeding of infant and malnutrition
causes and prevention. Their knowledge regarding the infant feeding
is poor especially regarding the components of complementary
feeding when to start, quality and quantity and thickness of food.
Knowledge and attitude of mothers need to improve by group and /or
individual counselling. Stay in the NRC should be utilized to improve
their knowledge and attitude on infant feeding. IYCF Centre facilities
need improve to support, mothers having Breast–feeding difficulties.
Acknowledgements
We acknowledge the medical officers, resident doctors especially
Dr. Mohit and nursing staff working in the paediatric wards & NRC
- HRH for their contribution to the implementation of the program
and special thanks to Ms Ritha Biju & Ms Mini Mehta (staff nurses –
paediatrics) for approximately 100% anthropometry & coordinating
records management and data entry for the purpose of this analysis.
Contributors:
Dr Alka Mathur, In charge NRC & Dr Rajesh Kumar Meena
contributed to conceptualizing the study and patient care.
Dr Alka Mathur and Ms Geetanjali Tahilramani contributed to programme implementation.
Dr Alka Mathur and Ms Geetanjali Tahilramani led data
analysis, interpretation and wrote manuscript.
All the authors reviewed and approved the final manuscript.Disclaimer
The views expressed in this paper are those of the authors and do
not necessarily reflect the official position of the institutions they are
affiliated with.
References
Citation
Tahilramani G, Meena RK, Mathur A. To Study Knowledge, Attitude and Practices (KAP) of Mothers of Children (1-59 Months) Admitted with Severe Acute Malnutrition (SAM) Regarding Feeding and Prevention of Malnutrition. Indian J Nutri. 2021;8(3): 233.