Research Article
Management of Metabolic Syndrome with Lifestyle Counseling and Supplementation with Flaxseed
Mageshwari JU1, Trueman P1, Krishnan D2 and Viswanathan V1*
1M.V.Hospital for Diabetes and Diabetes Research Centre (WHO Collaborating Centre for Research, Education and Training in
Diabetes)(IDF centre for Excellence in Diabetes care) Royapuram, India
2D V Living Sciences Pvt Ltd, Chennai, India
*Corresponding author: Viswanathan V, M.V. Hospital for Diabetes and Diabetes Research Centre (WHO Collaborating Centre
for Research, Education and Training in Diabetes)(IDF centre for Excellence in Diabetes care) Royapuram, India, Email: drvijay@mvdiabetes.com
Article Information: Submission: 01/05/2021; Accepted: 08/06/2021; Published: 10/06/2021
Copyright: © 2021 Mageshwari JU, et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly
cited.
Abstract
Background and Objectives: Flaxseed is a rich source of soluble dietary fibre, alpha- linolenic acid(ALA), and secoisolaricires inoldiglucoside (SDG)
all of which have been proven to reduce weight and lipid levels. This study was aimed to examine whether a low dose flaxseed suppresses lipid and reduces
weight.
Method: The study was an internal experimental study. Participants visiting M.V. Hospital for Diabetes in Chennai, were screened whose ages were
between 25 to 55 years. About 108 participants were recruited for the study i.e. 56 men and 44 women. All participants were on OHA and had no change in their
medication. They were divided into two groups, control and trial group with 50 and 58 participants respectively. Both groups received intense diet counselling
and asked to maintain their diet with 30mins of brisk walking daily. Trial group was counselled to include two level tablespoons of powdered flaxseed in 100
ml of water. The Study duration was for 3months.
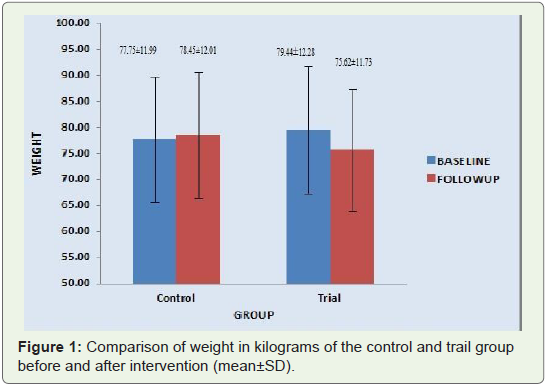
Results: The initial weight of the control and trial group was 77.75±11.99 and 79.44±12.28 respectively. The final weight of the control group was
78.45±12.01, a increase from the initial weight (p=0.005) while in the trial group there was a decrease in weight from 79.44±12.28 to 75.62±11.73. (P<0.001).
There was a significant decrease in HbA1c from 7.75 ± 0.94 to 6.76 ± 0.68. (P<0.001) and Triglycerides, LDL and Cholesterol.
Interpretation and Conclusion: These finding suggests that flaxseed supplementation helps to reduce weight and helps in glycemic control among
subjects with Type 2 Diabetes.
Keywords
ALA; Flaxseed; Glycaemic control; Low density lipid; obesity; Secoisolariciresinol diglucoside; Total cholesterol; Triglycerides
Introduction
Metabolic Syndrome (MetS) has been defined as a constellation
of metabolic abnormalities including central obesity, dyslipidaemia,
elevated blood pressure, Type 2 Diabetes and cardiovascular disease
[1]. Due to a rapid change in lifestyle i.e. diet pattern and exercise
in the last few decades, MetS has become a major challenge in India
and affects nearly 62 million and by 2030 nearly 90% of the total
population of India is likely to be affected by Diabetes. One of the
main causes of MetS is obesity. Obesity is a major health concern
and an important risk factor for Diabetes, cardiovascular disease and
cancer. According to the World Health Organization in 2014, more than 1.9 billion adults were overweight (body mass index [BMI] ≥
25 kg/ m2), and 600 million were obese (BMI ≥ 30 kg m2) [2,3]. It
is predicted that ~1.12 billion individuals will be obese by 20303.
Evidence supports the role of diet in the development of MetS4 and
obesity. The scientific advisory committee of the American Heart
Association (AHA) has published dietary recommendations for MetS
management [5]. A decreased prevalence of MetS was reported with
intensive approaches [6], i.e. very low-energy diets [7] and structured
dietary regimens, including low-fat and high-carbohydrate diets [8].
However, it is unknown whether [9] a less intensive lifestyle program
might also be effective.
Flaxseed is a complex food containing high amounts of PUFA,
mainly α-linolenic acid (ALA), an (n-3) fatty acid, as well as soluble
fiber, lignan precursors, and other substances that may have health
benefits [4]. Flaxseed contains 22% ALA and contains high levels of
soluble dietary fibre [9-11]. Harper et al [12] found that ALA from
flaxseed (3 g/day) tends to increase the concentrations of the large,
less atherogenic LDL1 and LDL2 sub- fractions. The smaller diameter
and more dense LDL particles have a greater proclivity for oxidation
and an enhanced ability to penetrate the intima compared with the
larger, less dense LDL particles.
Many studies have reported a loss of weight due to the presence
of soluble fiber which helps in the control of hunger and intake [13].
A two arm internal experimental study was conducted to study
the effect of flaxseed supplementation as an adjunct intervention
to lifestyle counselling. Additionally, the BMI, triglycerides levels,
total cholesterol levels, HbA1c values, as well as the fasting and post
prandial blood sugars were evaluated.
Aim of the Study The aim of the study was to examine whether
flaxseed supplementation in the diet reduces weight and brings about
glycemic control and improves Lipid profile among subjects with
Type2 Diabetes Mellitus.
Methods
Study Design The present study was an internal experimental
study. Participants with metabolic syndrome, i.e. central obesity,
dyslipidemia, and Type 2 Diabetes Mellitus visiting a tertiary care
Centre M.V. Hospital for Diabetes and Prof. M. Viswanathan
Diabetes Research Centre in the department of Diet and Nutrition in
Chennai, South India were screened whose ages were between 25 to
55 years and those meeting the following parameters were included
in the trial i.e. fasting blood glucose above 120 mg/dl, and BMI above
25. The study was for a period of three months from January 2019
to May 2019. Exclusion criteria were clinically diagnosed renal, liver,
heart, endocrine disturbances mental diseases or digestive problems
and those already taking flaxseeds and nuts.
A total of 300 individuals visiting the center were screened and
108 participants were recruited for the study (58 men and 50 women).
All participants were on OHA and did not change their medication
during the trial period.
The Study protocol was approved by the institution’s ethical
committee. The registration no. was IEC/N-014/11/2018.
Lifestyle counselling included the two main components of diet
and exercise.
All participants received intensive diet counselling by a Senior
Dietitian and were provided with guidance on diet. They were asked
to follow their diet, with the following instructions such as limited
consumption of red meat (twice a month), normal salt intake, with
normal fruit (1 to 2 servings per day) and vegetable consumption (3
to 4 servings per day)
Participants were divided into two groups i.e. both groups received
lifestyle counselling which included 30 minutes of brisk walking
and their regular diet pattern. The participants in the trial group were requested to take two level standard measuring tablespoons of
flaxseed powder in 100 ml of water and have it in the morning before
breakfast. The participants were called once a week telephonically to
ensure dietary adherence as well as adherence to the study protocol.
Baseline Measurements:
The age group of the participants was between 25 to 55 years.
Based on the baseline survey 108 participants (36%) met the criteria
of selection. At baseline a dietary recall was taken to evaluate their
normal dietary habits, medication details and activity pattern.Standardized protocols were used to collect anthropometric
measurements. Body weight and height were measured in light
clothing without any shoes to the nearest 0.1kg and 0.1cm respectively.
BMI was calculated as kg/m2 .
Participants were requested to fast overnight and fasting and post
prandial samples were collected. Serum samples were analysed on the
same day. All examinations and sample collections were repeated at
the completion of the 3 month intervention period.
Serum glucose fasting and post-prandial values were measured
enzymatically on an automatic analyser (BS-400mindray). HDL was
measured using immuno inhibition, cholesterol and Triglyceride
using enzymatic method and LDL direct measurement (BS-
400mindray).
Haemoglobin A1C (HbA1c) was quantified using immuno turbi
metric method (cobas 311).
Statistical Analysis:
Statistical analysis was performed using IBM SPSS version
2.0. Statistical analysis was done for baseline data using t-test for
independent samples. Frequency, percentage was done by Fisher’s exact test. A comparison was performed between initial and final
evaluation with paired t- test.Result
A total of 108 participants were divided into two groups 50 in the
control group and 58 in the trial group. The study period was for 3
months from Jan 2019 to May 2019 Eight participants dropped out
due to lack of interest to continue the study in the trial group.
Baseline Characteristics: The age range was 25 to 55 years with
the mean age of the control group was 50.92±7.74 and that of the trial
group 50.88±8.17. Forty eight percent (n=24) and 64 % (n=32) were
men in the control and trial group respectively. After randomization,
the group appeared fairly balanced with respect to BMI and
medication uses.
Dietary adherence was 92.59% (8 participants dropped out of
the study). At the end of the 3 month period total energy intake
decreased from the baseline calories 1528±252 to 1464±124 for the
control group (p =0.012) and calories of trial group from 1533±155
to 1400±124 at the end of the 3 month trial period which was highly
significant in the trial group (p < 0.001). The percent of energy from
carbohydrate and fat significantly decreased in both groups (Table 1).

There was a 7.2% decrease in the intake of carbohydrate in the
control group while the decrease in the intake of trial group was
12.5%.
The decrease in fat intake was 6.8% and 11.06% in the control and
trial group respectively.
The participants of the trial group had a highly significant level of
weight loss from 79.44±12.28 to 75.62±11.73 (p < 0.001). The control
group did not show the same loss in weight but there was a slight
increase in weight (p=0.005) (Figure 1).
The trend was reflected in the BMI values also. The initial BMI
of the control group was 30.53±3.88 and that of the trial group was 30.67±4.00. The BMI after the intervention period of three
months was 30.79±3.85 and 29±3.83 of the control and trial group respectively. The decrease in BMI was highly significant in the trial
group (p<0.001) While the control group did not show any change in
their BMI (p=0.043).
Table 2 shows the comparative fasting and post prandial
blood sugars of both the control and trial groups. The values show
a decrease in both the fasting and post prandial blood sugar levels
after intervention with flaxseed which was statistically significant
(p<0.001).

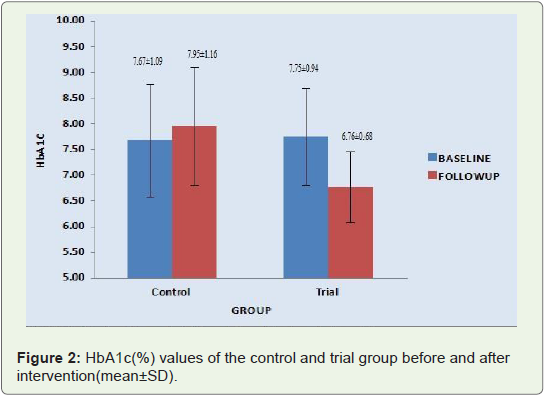
The reduction in blood glucose values resulted in a decrease of the HbA1c values in the trial group as shown in Figure 2. The HbA1c
values significantly reduced from 7.75±0.94 to 6.76±0.68 in the trial
group (p<0.001).
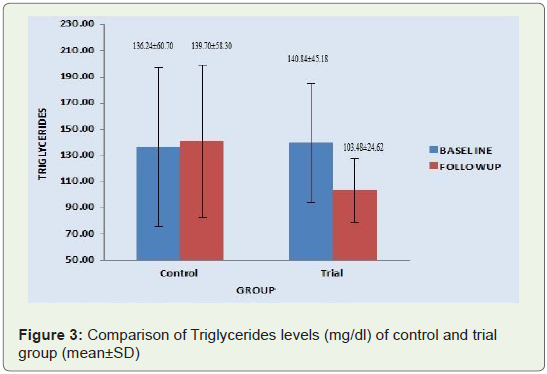
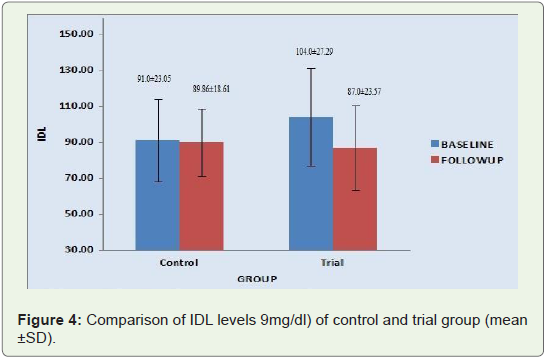
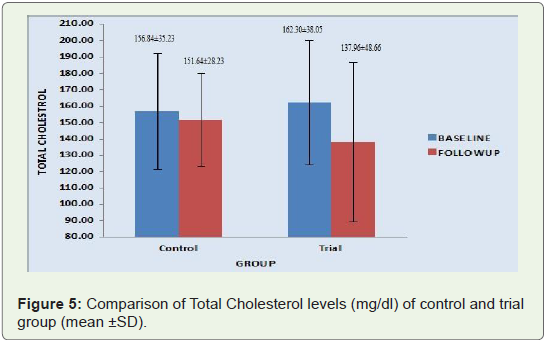
A similar reduction in the triglyceride, LDL and total cholesterol
levels were seen in the trial group after intervention. There was a
lowering of TG, LDL and total cholesterol by 26%, 16% and 24%
respectively which was highly significant (p value of 0.000) in all three
cases.
The same trend was not observed in the control group. There was
a decrease in the total cholesterol level in the control group which was
not significant as can be seen in Figures 3,4 and Figure 5.
However the HDL values of both the control and trial group did
not change after intervention as seen in Table 3

Discussion
In the present study two level standard measuring tablespoons of
powdered flaxseed was given to the participants of the trial group to
be taken in water early morning before breakfast.
Kristensen et al 14 (2013) in their study reported that addition of
2 g/MJ of flaxseed dietary fiber (from isolated mucilage) to a mixed
meal decreased lipid response. They have also reported that subjective
measures of appetite to point toward increased satiety after a flaxseed
meal. Other literature also reports a similar finding when given a
viscous dietary fiber source like flaxseed [15-17]. They also observed
an inhibitory effect of flaxseed dietary fiber on the hunger-signalling
hormone ghrelin which was observed throughout the test day [14].
The results of this study were also substantiated by a systematic
review and meta analysis of RCT [13]. This analysis reported that
participants ingesting flaxseed products had lower body weight, BMI
and waist circumference after intervention than controls. Research
has shown that this reduction in weight was due to the presence of
lignans primarily secoisolaric resinol diglucoside (SDG) [18,19].
The significant decrease in body weight and BMI following
supplementation with flaxseed can also be explained by the subsequent
increase in circulating ALA. ALA is converted to eicosapentaenoic
acid (EPA, 20:5,n=3) and docosahexaenoic acid (DHA, 22:6,n=3) in
the body [20]. The anti-obesity effects of EPA and DHA have been
well documented [21-23].
It is a known fact that obesity is associated with abnormal postprandial
lipid patterns [24]. Reductions in triglyceride concentrations
have been observed in individuals consuming dietary fibers from
other foods like pea fiber [25], oat bran [26], wheat [27] etc.
Other studies have reported that there was a lowering of both
total cholesterol and LDL cholesterol by 12 and 15% respectively in
7 days [28]. It has also been reported in this study [28] that 5 g of
dietary fiber from flaxseed for one week significantly increased fecal
excretion of fat and reduced total and LDL cholesterol.
Purified lignans in the form of SDG have been shown to reduce
visceral fat in mice [29]. The authors 29 have reported that the
high content of SDG may contribute to the overall effect of flaxseed
through a reduction of mRNA levels of sterol regulatory element binding proteins that are involved in triacyl glycerol synthesis. It is
also suggested that SDG may also be useful in regulating adiponectin
levels and can prevent or reduce obesity through increased fat
oxidation in skeletal muscle [29]. The current study found that two
level standard measuring tablespoons of powdered. Flax seed per
day reduced fasting and post prandial blood glucose levels with a
corresponding significant reduction of HbA1c levels.
Hutchins et al (2013) [30] have reported in their study that a daily
low dose of flaxseed supplementation decreased insulin resistance
in overweight and obese, glucose intolerant people. Fasting insulin
values also significantly reduced with daily consumption of 13 g of
ground flaxseed.
Kristensen et al [14] have reported a decreased insulin response
after supplementation with flaxseed which may indicate that flaxseed
dietary fiber reduced the rate of glucose uptake leading to a decreased
demand for insulin to match the rate of glucose uptake in peripheral
tissue.
Limitations of the Study
The sample for the present study comprised of only 108 people
with diabetes visiting the MV Hospital. This sample is only a very
small proportion of the entire population of diabetics. Therefore,
research studies with much larger sample size would be required to
ensure appropriate generalization of the findings of the study.
Conclusion
Two level standard measuring tablespoons of powdered flaxseed
was supplemented in the diet to the trial group showed reduced
weight and BMI. There was a lowering of the LDL, total cholesterol
and triglyceride values. However there was no significant difference
in the HDL levels. The present findings should be regarded as proof
of the efficacy of flaxseed to reduce weight and maintain lipid profile
and control HbA1c values.
Acknowledgement
The authors wish to thank Prof. M. Viswanathan Diabetes
Research Centre for the funding to carry out this work.
References
Citation
Mageshwari JU, Trueman P, Krishnan D, Viswanathan V. Management of Metabolic Syndrome with Lifestyle Counseling and Supplementation with Flaxseed. Indian J Nutri. 2021;8(3): 232.