Research Article
A Study to Understand Pattern of Weight Gain among Undernourished Children Admitted to Nutritional Rehabilitation Centre in a Tertiary Health Care Setting- A Retrospective Study
Karn M1*, Angolkar M1, Herekar V2, Adhikari H1, Sharma R1 and Karn A3
1Department of Public Health, J.N. Medical College, India
3Department of Paediatrics, J.N. Medical College, India
3MPH, Chitwan Medical College, Nepal
*Corresponding author: Mukesh Karn, MPH, Department of Public Health, J.N. Medical College, KAHER, Belagavi, Karnataka, India Email: m.mukace@gmail.com
Article Information: Submission: 02/04/2020; Accepted: 08/09/2020; Published: 12/09/2020
Copyright: © 2020 Karn M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: Malnutrition in developing countries causes 45% of deaths among under-five children according to WHO health statistics 2016. India is one among the many developing countries where child malnutrition is a major problem and severe. India is home to more than one-third of the world’s undernourished children.
Objective: The aim of the study was to understand pattern of weight gain among undernourished children admitted to nutritional rehabilitation centre in a
tertiary health care setting.
Methodology: A retrospective study was conducted using records from Nutritional Rehabilitation Centre ward. This study has been taken up to analyse data of last three years to determine its impact on weight gain pattern. 320 children aged between 1-60 months were recruited and their records were analyzed. Demographic information was collected by telephonic interview. SPSS 20.0 and WHO Anthro software was used to analyze the data.
Results: Majority (75.3%) children were severe acute malnourished. 58% of children were male of which 40% were below the age of one. Mean (SD) duration of stay in the nutritional rehabilitation centre was 8.9 (4.9) days. There was a statistically significant (p<0.05) difference between mean weight at admission and mean weight at discharge, socioeconomic status and clinical impression.
Conclusion: NRC had a good impact on weight gain among admitted children. The weight gain was statistically significant. Though stay at NRC has
shown improvement in the weight gain, but during the time of discharge most of the children are still undernourished due to shorter duration of stay at NRC.
Keywords
Severe acute malnutrition; Nutritional Rehabilitation Centre; Under five; India
Introduction
Adequate nutrition in early years of childhood is an essential element for ensuring healthy growth, a strong immune system, proper organ formation and function, leading to neurological and cognitive development. A well nourished population is a base on which the economic growth and human development of the community rests. Malnutrition can be defined as a pathological condition, which occurs due to the deficient assimilation of the components of the nutrient complex. It manifests in varying degrees of severity and diverse clinical manifestations [1]. A child can be said to be suffering from Severe Acute Malnutrition (SAM) if his/her weight for height is less than -3SD (as recommended by the WHO) and/or if they suffer from visible severe wasting and/or oedema of both feet (excluding other causes of oedema), and if their mid arm circumference less than
11.5 cm (in infant more than 6 months of age) [2]. According to the National Family Health Survey 4, cases of stunted and underweight children have decreased by 10% and 6.8% respectively in the last ten years, among under five children in India. Wasting, however, has increased by 1.2% and severe wasting (SAM) by 1.1% in the same duration of time [3].
In the state of Karnataka NFHS-4, has shown that the prevalence
of wasting has increased by 8.5% and severe wasting by 3.8% in the
last decade [4]. The district of Belgaum has a very high prevalence of
wasting with 33.1% and severe wasting with 18%, which are much
more than the national and state data [5]. The increasing number
of children being affected of severe wasting should lead a serious
concern to be taken for the improvement of nutritional status among
the children so that they can lead a normal life without any forms of
malnutrition.
Under NRHM4, many Indian states have established Nutritional
Rehabilitation Centres (NRCs) that provides integrated facilities
of initial treatment at the health facility and after that community
follow ups. With the support of UNICEF, GOI further started, the
NRCs under Bal Shakti Yojna with objective of bringing down the
prevalence of SAM <1% [6,7]. Although lately, 966 of NRC’s have
been established in private and public settings in India, however their
impact in correcting the problem needs to be studied. In KLE’s Dr.
Prabhakar Kore Charitable Hospital, the NRC unit was established in
2013. This study has been taken up to analyse data of last three years
to determine its impact on weight gain pattern.
Materials and Methods
The present retrospective study was carried out amongst 320
children’s data who were admitted in NRC aged between 1 to 60
months. The necessary data required for the study was obtained as
primary and secondary. Accordingly, secondary data was collected
from patient’s case sheets, weight at admission, weight at discharge,
height, number of days of hospital stay etc as required. Primary data
was collected by telephonic interview with the parents for collecting
the socio-demographic information. Data from February 2014 to Dec
2016 was taken into account. Duration of the study was 10 months
from February 2016 to November 2016.
Sample size: Complete enumeration. Record of 320 participants
was analysed out of total record of 380 patients. If the children weight
for height z scores were below -3 SD then they were considered as
SAM and if the weight for height of children lies between -3 SD to -2
SD then they were considered as MAM according to WHO standards.
Record of all haemodynamically stable children of age 1 to 60
months were included. Incomplete record and children with severe
multiple congenital anomalies were excluded from the study. A Pilot
study was conducted on record of 35 participants before starting the
actual study to check validity and reliability of study tool.
Ethical consideration: Before conducting the present study,
written permission was obtained from Medical Director, KLE’s Dr.
Prabhakar Kore Charitable Hospital, Belagavi. Ethical clearance for
this study was obtained from the Institutional Ethics Committee of the J.N. Medical College, Belagavi. Verbal consent was obtained from
parents before data collection via telephonic interview.
Data analyses:
Data entry and analyses were done by using both WHO Anthro
software version 3.2.2 and SPSS 20.0. The nutritional survey option
in WHO Anthro software version 3.2.2 (WHO, Geneva, Switzerland)
for assessing growth and development was used to calculate weightfor-
height z-scores on the basis of WHO standards.Frequency, percentage, mean and standard deviation were
calculated. Non parametric test was used to see the difference between
two means. Level of significance was considered at p<0.05.
Results
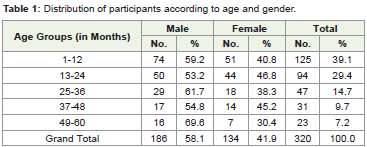
Table 1 showed that out of 320 participants, 186 (58.1%) were
male and 134 (41.9%) were female. With regard to age distribution it
was observed maximum number, 125 (39.1%) participant were found
in 1-12 months age group, where male children were 74 (59.2%) and
51 (40.8%) were female children (Table 2).
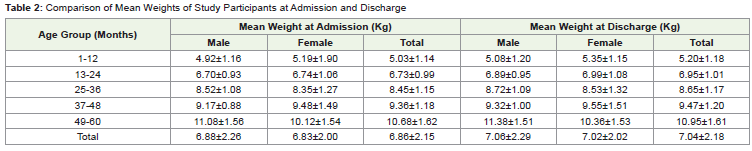
There is an increament on weight among children at NRC. Overall
mean weight at admission was 6.86 ± 2.15 kg. For males, it was 6.88 ±
2.26 kg and for females, it was 6.83±2.00 kg. The overall mean weight
at discharge was 7.04 ± 2.18 kg. For males, it was 7.06 ± 2.29 kg and
for females, it was 7.02 ± 2.02 kg. Clinically, at the time of admission
the mean (SD) weight was 6.86 ± 2.15 kg which increased to 7.04 ±
2.18 kg. Statistically, the weight gain was analysed by Wilcoxon Rank
test and it was found that the weight gain was statistically significant
(p=0.000). When it was analysed for gender and mean weight at
admission and discharge, statistical significance was found at p=0.01.
Table 3 shows that, there was statistical significance found
between the no. of days at hospital stay and the mean weight gain.
This says that the weight increased as the duration of stay in the
hospital increased.
Discussion
A study conducted in Belagavi city showed that 36.7% of
participants belonged to age group of 13-24 months [8]. In a study
conducted in Waynad district of Kerala city showed that more than
30% of the participant were of less than 2 years of age [10]. A similar
finding was reported by a study conducted in Bhopal, where majority
42.1% were in the age group of 13–24 months [11].
In the present study, mean ± SD weight at admission and
discharge were 6.86 ± 2.15 kg and 7.04 ± 2.18 kg. The mean weight
gain was 0.18kg. There is difference in mean weight at admission and mean weight at discharge, and the difference is statistically significant
(p<0.05). A simialr finding was reported by a study conducted in
Nellore. A statistically significant difference was found between mean
weight at admission and mean weight at discharge for all children
(p<0.001) [13]. A study conducted in Madhya Pradesh also had the
similar finding as our study. A statistically significant difference was
observed between the mean weight at discharge and the mean weight
at admission for the study group (t=14.552, P<0.001) [14]. In contrast,
another study also conducted in Madhya Pradesh reported that no
significant difference was found between mean weight at admission
and mean weight at discharge for participants (p>0.05) [15]. A study
conducted in Ghana at four day NRC care also reported a significant
increase in weight for age for the admitted children [16].

In the present study, the mean (SD) number of days of hospital
stay was found to be 8.99(4.94) days. In a study conducted in
Allahabad city, the findings regarding to length of stay at hospital was
12(6.8) days [17]. In a study conducted in UP, the mean (SD) length
of hospital was 13.2(5.6) days [18]. A similar result to that of UP was
found in a study conducted in Madhya Pradesh where, average (SD)
duration of stay was 13.51(2.73) days. A similar finding to these was
seen in a study conducted in Baroda city, where mean duration of
hospital stay was 15.6 days.
Conclusion
A statistically significant weight gain was observed among SAM
children treated at NRC, as analyzed by comparing the weight at
admission and discharge. The length of stay at NRC was found
statistically significant with weight gain at discharge. NRC has a
good impact on improving nutritional status of undernourished
children. Though stay at NRC has shown improvement in the
weight gain, but during the time of discharge most of the children
are still undernourished due to shorter duration of stay at NRC.
Lower socioeconomic status is also significantly associated with
malnutrition which is primarily because of inability of guardian to
resume work and because of that they have to compromise their daily
wages which in turn makes them to get their children discharge from
hospital much earlier than recommended period of stay.
References
Citation
Karn M, Angolkar M, Herekar V, Adhikari H, Sharma R, et al. A Study to Understand Pattern of Weight Gain among Undernourished Children Admitted to Nutritional Rehabilitation Centre in a Tertiary Health Care Setting- A Retrospective Study. Indian J Nutri. 2020;7(2): 216.