Review Article
Nutrition Management in Patients with Cirrhosis in Present COVID-19 Pandemic
Sharma P*, Kumar A and Arora A
Department of Gastroenterology and Hepatology, Sir Ganga Ram Hospital, India
*Corresponding author: Sharma P, Department of Gastroenetrology, Sir Ganga Ram Hospital, New Delhi, India; E-mail: drpraveen_sharma@yahoo.com
Article Information: Submission: 22/06/2020; Accepted: 18/07/2020; Published: 23/07/2020
Copyright: © 2020 Sharma P, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Purpose: COVID-19 pandemic has affected millions all over the world. People who are obese, elderly, with chronic kidney disease, cardio vascular disease, chronic liver disease, associated malignancy and chronic airway disease are prone to develop severe COVID-19 with increased mortality. Malnutrition is a common problem in all these co morbid illness including chronic liver disease and it is possible that malnutrition and sarcopenia add on to increased severity in these patients.
Results: Malnutrition is seen in 20-50% of patients with chronic liver disease and chronic liver disease is an independent risk factor for increased severity and mortality in patients with COVID-19 disease. Social myths about COVID-19 and intake of many herbal, Chinese and ayurvedic preparation with add on heavy metals may affect the liver function in this pandemic. Home quarantine has led to increase screen time and reduced physical activity time. This has affected many malnourished and sarcopenic patients with cirrhosis.
Conclusion: Malnutrition is common in patients with chronic liver disease and good nutrition, regular exercises and adequate supplementation with vitamins and nutrients is required in the present pandemic to improve survival.
Keywords
Malnutrition; Cirrhosis; COVID-19; Management
Introduction
Corona viruses are a family of viruses that can affect humans.
Upper respiratory tract infections are the commonest symptoms
though it can affect liver and intestine also. Majority of the infections
are mild and self limiting with symptoms of cough, fever, body ache,
anosmia and diarrhoea however severity can vary leading to severe
acute respiratory syndrome, multi organ failure and even death in few
cases [1,2].
Importance of nutrition in COVID-19 and its outcome:
Nutrition and immunity is a key determinant against various
bacterial and viral illnesses. Improving and supplementing nutrition
remains an important part of treatment regimen for acute and
chronic diseases for which a definitive etiologic treatment has not
yet been approved [3]. Adequate nutrition and enhanced immunity
may apply to the current SARS-CoV-2 (or COVID-19) pandemic as
till now we do not have definitive management protocol [4]. Patients
who are obese, hypertensive, diabetic, associated malignancy, renal
disease, cardiovascular disease, chronic respiratory disease, chronic
liver disease, old age and hypoalbuminemic patients had poor
outcome in COVID-19 [5-8]. There are no direct study evaluating
the role of nutrition per se on severity of COVID-19.However
considering together the various co morbid conditions in COVID-19,
indirect evidence supports the relevance of nutrition in present
pandemic as older age and the presence of comorbid conditions like
chronic renal and liver disease are almost invariably associated with
impaired nutritional status and sarcopenia. Similarly obesity with
associated sarcopenic obesity suggest role of nutrition in COVID-19
outcome. The presence of at least two chronic diseases in the same
individual can be defined as polymorbidity and is also characterized
by high nutritional risk. Presence of polymorbidity and addition of
inflammation and sepsis may further contribute to enhance severity
of SARS-CoV-2 infections [9,10]. Various nutritional markers like
lymphopenia and hypoalbunemia are also negative prognostic
factor in patients with COVID-19. Though serum albumin as a nutritional marker, its role in patients with inflammatory response
is a questionable importance, but low prealbumin level predicts
progression to Acute Respiratory Distress Syndrome (ARDS) may
suggest role of nutrition. These evidences support the role of nutrition
in prognosis of COVID-19 [11-13].Prevalence of malnutrition in cirrhosis:
Malnutrition is very common in patients with liver cirrhosis,
occurring in 20-50% of patients with 20% of patients with compensated
cirrhosis and more than 50% of patients with decompensated liver
disease [14]. Malnutrition spectrums include muscle mass loss
(sarcopenia) and/or protein calorie deficiencies. Sarcopenia and
malnutrition are not equivalent terms in patients with cirrhosis. Severe
malnutrition are associated with a higher rate of complications such
as more infections with increase severity, Hepatic Encephalopathy
(HE) both overt and covert, ascites, increased pretransplant waiting
list mortality, increased post transplant intensive care stay and post
transplant infections [15-18]. Various screening tools like Subjective
Global Assessment (SGA), royal free hospital nutrition prioritising
tool (RFHNPT) are used for rapid screening of malnutrition followed
by detailed assessment by methods of nutritional status (total
lymphocyte count, mid arm muscle circumference, mid arm muscular
area, tricep skin fold thickness, subscapular skinfold thickness, BMI
and handgrip measurement and Computed Tomographic (CT)
image analysis at the L3 vertebra [14].Liver disease a risk factor of severe COVID-19:
Liver involvement as suggested by impaired liver enzymes is seen in more than one third to half of patients with COVID-19. Majority of the studies had only 3-8% of the patients with pre existing liver disease and increased severity of COVID-19 in these patients has not yet been fully evaluated [2,5-7]. Singh et al. which included 250 patients with chronic liver disease [CLD, 42% Metabolic Fatty Liver
Disease (MAFLD) and n=50 with cirrhosis] [19]. These patients had associated co-morbidities like hypertension (68%), diabetes mellitus (48%), chronic kidney disease (CKD, 32%), chronic respiratory disease (40%) and congestive heart failure (CHF, 24%). Relative Risk (RR) of mortality in cirrhosis was (RR, 4.6) and in CLD (RR 3.0) compared to non CLD patients. In a large study by Moon et al. 103 patients with cirrhosis and 49 with non-cirrhotic CLD were enrolled and deaths occurred in 12.2% of CLD without cirrhosis [20], 24% CTP-A cirrhosis, 43% CTP-B cirrhosis, and 63.0% CTP-C cirrhosis. These studies had shown that underlying pre-existing liver disease is a risk factor for increased severity of COVID-19 and these patients should be looked upon by trained hepatologist and Internist.Patients who have MAFLD (Metabolic Fatty Liver Disease) and
chronic liver disease (fatty liver) are also prone to develop severe
COVID-19 as MAFLD shares common risk factors (hypertension,
obesity, dyslipedemia) with severity of COVID-19 [21].
Management of Nutrition in chronic liver disease in COVID-19 pandemic:
Majority of chronic liver disease patients which includes both
compensated and decompensated liver disease have poor nutrition.
Cirrhosis itself is a risk factor for severe COVID-19 so these patients
should be monitored very carefully in the present pandemic.Social myths/practises about diet in the present COVID-19
pandemic: Though majority of the people know that best strategy for
prevention of COVID-19 is self quarantine at home and maintaining
social distance and wearing mask outside home. Many local practises
also prevails in society which varies from country to country and
includes intake of some homemade remedies like kadha which
is a mixtures of Indian black pepper, ginger, resins, cardamom,
cinnamon and honey with warm water and to consume it three or
four times a day. Avoid high calories diet and take bland diet which
contains less fat and protein to avoid extra work on liver during this
pandemic. Some people are using Chinese herbs, ayurvedic herbs
with added heavy metals to boost the immunity [22-24]. There is no
scientific basis for these and how much they affect liver is also not
known. Avoiding good nutritious diet which is rich in proteins like
meat, fish and other animal products like milk and milk products is
affecting patient with cirrhosis who are already protein and calorie
malnourished.
WHO has given its guidelines in the present pandemic and advised
for proper nutrition and hydration which are vital in the present
pandemic. WHO advised to eat a variety of fresh and unprocessed
foods every day to get the vitamins, minerals, dietary fibre, protein and
antioxidants which our body require to boost up immune response.
Drink enough water which includes 8-10 cups of water. Avoid sugar,
fat and salt to significantly lower risk of overweight, obesity, heart
disease, stroke, diabetes and certain types of cancer. These guidelines
are followed by majority of people including patients with cirrhosis
and decompensated cirrhosis. Though majority of the guidelines
are good but for people who had chronic kidney disease, chronic
decompensated liver disease and chronic heart disease with failure
need special precaution as are already fluid overloaded and excess
water intake may worsen there problem [25].
Common principles to be followed while dealing with chronic
liver disease patients in present pandemic.
Assessment of malnutrition: All patients with cirrhosis,
malnutrition assessment should be done. Common easy methods
include measurement of body mass index with corrected body
weight, assessment of Child’s status, SGA and RFH-NPT should be
assessed in all patients. These are simple methods and questionnaire
based assessment of malnutrition and can be easily calculated by a
physician or his supporting staff without taking much time. These can
also be calculated on a telephonic discussion if patient do not want to
come to clinic/hospital during present pandemic. Patients with BMI
less than 18.5 kg/m2, Child’s Pugh class C and SGA score of mild and
severe malnutrition and RFH-NPT score more than 1 are the patients
that should be screened in detail and corrective measures to be taken
to improve nutrition [14]. Preserving nutritional status and treating
malnutrition is also important to reduce complications in patients
with cirrhosis at nutritional risk who might incur in COVID-19 in
the future.
Though there are no direct study evaluating the role of malnutrition
in non cirrhotic or cirrhotic patients and severity of COVID-19.
However in a previous study in influenza infections, increased
mortality predictors includes type of virus (OR 7.1), malnutrition
(OR 25.0), hospital-acquired infection (OR 12.2) and respiratory insufficiency (OR 125.8) [26]. Subjects with malnutrition should try
to optimize their nutritional status, ideally by diet counseling from
an experienced dietician with sound knowledge of diet in patients
with liver disease (preferably through video conferencing to prevent
contact). Obesity, chronic liver disease and old age patients are
risk factors of severe COVID-19 so obesity does not preclude these
patients for nutrition assessment. Dietician should regularly follow
these patients for adherence to dietary plan and reassess the nutrition
status of these patients.
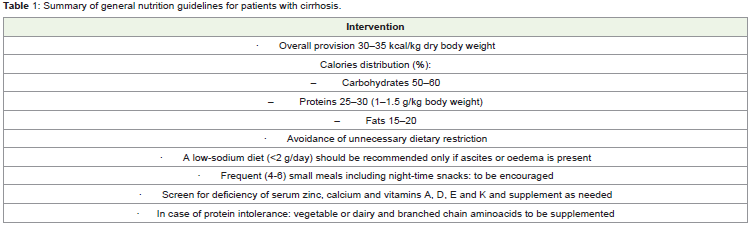
Total calories/protein/carbohydrate and fat intake:
Majority of patients with cirrhosis are malnourished and hence
even at home for self quarantine and not doing enough work out/
exercise does not mean taking fewer calories. Patient should continue
to follow the guidelines of ESPEN as before the COVID-19 pandemic
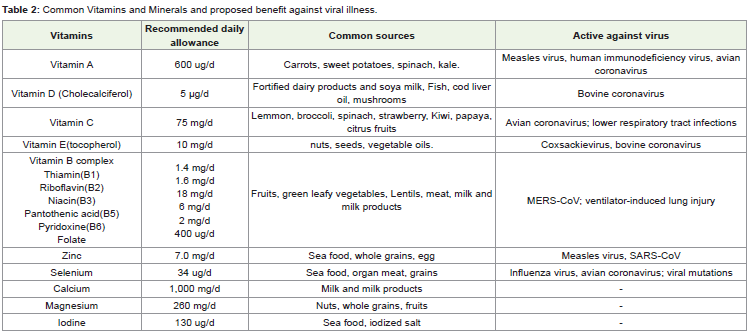
[27] (Table-1). Patient with cirrhosis should continue with daily
multivitamin supplement (Table 2). Routine testing for vitamin
deficiency or their level should not be monitored in every patients of
cirrhosis as is not cost effective and not available routinely.As most patients will remain at home adequate intake of Vitamin
D should be encouraged in all. Vitamin D is a well-known regulator
of innate immunity. Vitamin D deficiency has been associated
with a number of viral and bacterial diseases including influenza,
Human Immunodeficiency Virus (HIV), hepatitis and mycobacterial
infection. Vitamin D role in bovine corona has been seen [28-31].
Vitamin A has been defined as “anti-infective” vitamin since many of
the body’s defences against infection depend on its adequate supply.
In an animal study it was found that the effect of infection with
Infectious Bronchitis Virus (IBV), which is a kind of corona viruses,
was more pronounced in animals fed a diet marginally deficient in
vitamin A than in those fed on an adequate vitamin A diet. Adequate
supplementation with Vitamin A is advised for all patients with
cirrhosis [32].
Role of vitamin C to lower incidence of lower respiratory infection has been seen in few studies. The COVID‐19 had been reported to cause lower respiratory tract infection, so supplementation with vitamin C could be one of the effective choices for the treatment of COVID‐19 [33-35]. Selenium deficiency also increases influenza virus infection so supplementation will help in all patients [36]. Zinc
has an important role in immune cells of both the innate and adaptive immune system and its deficiency may results in dysfunction of both humoral and cell‐mediated immunity. In addition, the combination of zinc and pyrithione at low concentrations inhibits the replication of SARS Coronavirus (SARS‐CoV) [37-38]. Zinc supplementation also decreases the hepatic encephalopathy in cirrhosis patients [39]. Therefore, zinc supplement may have protective effect in COVID‐19
and should be supplemented in all patients with cirrhosis [40] (Table 2).
Physical exercises while remaining quarantine:
Best preventive measure to reduce infectious risk is to remain
quarantine at home and is endorsed all over the world [40]. However,
prolonged home stay may lead to increased sedentary life and its
associated problems. More and more people including patients with
cirrhosis are spending time in lying down and watching television
and mobile phones. Increase in screen time had led to lower physical
activity time. Prolonged sedentary behaviour in patients with
cirrhosis who are sarcopenic can lead to worsening of their muscle
strength. Reduced aerobic exercises can also alter immune system
and make them prone to develop secondary infections [41]. Many
people have underlying diabetes and obesity related problems and
sedentary lifestyle affects glycemic control and associated problems
of increased susceptibility to secondary infections.In the developed and developing countries majority of people are
living in a small apartment with little free space. Patient with cirrhosis
can continue exercise at home even open space is a constraint using
various safe, simple, and easily implementable exercises tools. These
easy steps will also avoid the airborne coronavirus and maintain
fitness levels in these patients. Exercises that can be easily done at
home include strengthening exercises, stretching exercises, or a
combination of these along with some aerobic exercises if space
allows. Common example of home exercises include stand-to-sit and
sit-to-stand using a chair and from the floor, chair squats, and situps
and push ups if possible. Even walking in home and climbing
stairs with support, playing with kids or pets for 20 minutes, dancing
at home or traditional yoga should be considered since they require
no equipment, little space, and can be practiced at any time. Various
health programmes on television, internet and mobile apps are some
other ways to keep your health in a good shape. Regular exercise
improves your muscle and improves appetite and general well being. Limited outdoor activities such as garden walk or light outdoor
games like table tennis and badminton can be tried. Every day >20-30
min or every second day > 40-60 minutes exercise is recommended
to maintain mental and physical health, muscle mass and thus energy
expenditure [42].
Patients who have decompensated cirrhosis and ascites should
also do exercises which may include walking in the home for 15-
20 minutes, playing with kids/pets or some sort of stretching or
strengthening exercises during this pandemic. Daily monitor of
weight is also important to keep watch on amount of ascites. Excessive
amount of water should be avoided and these patients must ask or
inform their treating physician if taking any alternative/off label
medicines.
Conclusion
Majority of patient with cirrhosis are malnourished and its
severity increases with increase in Child’s Pugh status. Cirrhosis
patients either compensated or decompensated and patients with
MAFLD are also prone to develop severe COVID-19.In the present
pandemic best preventive strategy to COVID-19 is to stay home and
keep proper social distancing and wearing face mask. However staying
at home has increased screen time compared to physical activity time
in all persons including patients with cirrhosis. Prolonged screen
time can worsen the already prevalent sarcopenia in patients with
cirrhosis. Social myths about diet and cultural practises while staying
home also add to nutrition problem in patients with cirrhosis. Taking
herbal, Chinese, ayurvedic treatment with add on heavy metals to
improve immunity can lead to worsening of liver status in these
patients. All patients with cirrhosis should have a screening test for
malnutrition which can be done either by doctor or his paramedical
staff or dietician even on video conferencing. Patient who found to be
malnourished should be screened by trained dietician on telephone or
preferably on video conference and corrective measures to be taken.
All patients should get supplements with multivitamins on regular
basis as regular exercises which can be done even at home should be
enforced in all patients.
References
25. WHO (2020) Food and nutrition tips during self-quarantine: what to choose
and how to eat healthily.
Citation
Sharma P, Kumar A, Arora A. Nutrition Management in Patients with Cirrhosis in Present COVID-19 Pandemic. Indian J Nutri. 2020;7(2): 215.