Research Article
Cost of Enteral Formulae Feed in Critically Ill Patients in a Tertiary Care Centre: An Observational Study from India
Sanjith S* Apoorv T and Nikita shah
Department of Critical care, Raheja-Fortis, India
*Corresponding author: Sanjith S, Department of Critical care, Raheja-Fortis, Mumbai, India, Tel: 00919004479549; E-mail: docsanjith@rediffmail.com
Article Information: Submission: 03/12/2019; Accepted: 30/12/2019; Published: 31/12/2019
Copyright: © 2019 Sanjith S, et al. This is an open access article distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction: Specialized enteral feeding provided by the use of scientific formula feeds are considered costly and cost is very important factor in Indian
ICU. The aim of this study is to evaluate the cost of enteral formulae feeding in critically ill patients in a tertiary care center and to correlate the cost to the
severity of illness and LOS of patients in ICU.
Methodology: An Observational study was performed on2748 patients admitted in ICU of S.L Raheja Hospital over a period of 3 years who were completely
fed over formula feeds which was determined by iNutrimon Software. The feeding data were extracted from the patient file record and were analyzed.
Result: Overall results indicated that the average cost of scientific feeding formulae was 749 INR (10.77 U.S.Dollars)/day. Average LOS for the entire
population during the study period was 4.84 days. If the LOS was greater than 5 days the cost of formulae feeding was 325 INR (4.67 U.S.Dollars)/day and if
LOS was less than or equal to 5 days the cost was 826 INR (11.88 U.S.Dollars/day.
Conclusion: Lesser the number of days the patient stays in the ICU more is the cost of scientific formula feeding. Howsoever the cost of feeding per day
is much lesser than the cost of many others like antibiotics in the ICU.
Keywords
Enteral nutrition; iNutrimon software; Intensive care unit; Formula feeding; Length of stay; APACHE2; Cost of feed
Abbreviations
APACHE: Acute Physiology and Chronic Health Evaluation;
ASPEN: American Society of Parenteral and Enteral Nutrition; EN:
Enteral Nutrition; GI: Gastro Intestinal; ICU: Intensive Care Unit;
LOS: Length of Stay
Introduction
The benefits of enteral nutrition is very well known such as
reduced incidence of pneumonia and intra-abdominal infections
by reinforcing gut immunocompetence with their direct effect in
promoting MALT (Mucosa Associated Lymphoid Tissue) thus
producing IgA antibodies, reduced cost by reducing length of stay,
lesser chances of infection (associated with parenteral nutrition) and
avoidance of central line associated complications [1,2]. In India
and many other Asian countries, specialized enteral feeding can be
provided by the use of blenderised kitchen feeds or reconstituted
powder based supplemental nutrition also called as scientific formula
feeds. Other countries like the United states and European countries
have premixed liquid based formula feeding which are generally
ready to hang. Scientific feeding formulae have got some advantages
over blenderised kitchen diets which include minimization of feed
contamination [3], consistency in amount and supply of nutrients,
prevention of viscosity related blockage of feeding tubes etc. [4,5].
In an earlier observational intensive care unit study, among the 20
intensive care units studied in a city of Mumbai in India only around
50 % of patients were being fed by scientific formula feeds [6]. This
could be due to many reasons which include untrained staff, lack of
dietitians, physicians belief of non-superiority of scientific feeding
formulae, fear of diarrhea, lack of awareness and above all cost.
As per a systematic review conducted by Pritchard, a wide
variation in costs was reported, ranging from 7.8 U.S Dollars per day
of Enteral Nutrition (EN) in adults to charges of 46 U.S.Dollars per
day for pediatric ICU patients [7]. Another study done in medical
and trauma patients in a single centre reported around US$ 245 per
7 days, or US$ 35 per day [8]. Cost is a very crucial factor when it
comes to Indian Intensive Care Units since most of the payments are
out of pocket and less than 10 % of the entire population are covered
by medical insurance as per National Family Health Survey-4 for
national health insurance [9].
However to the best of our knowledge there is no such study
conducted in India that has evaluated the cost of scientific feeding
formula in intensive care patients. Hence this observational study
was carried out in a tertiary care intensive care unit which provides
nutrition by specialized formula feed to 100% of its patients when
indicated as per screening criteria with the aim of evaluating the cost
of enteral formulae feeding. Secondly we also studied the relation of
severity of illness (APACHE 2) and the Length of Stay (LOS) to the
cost of scientific enteral feeding.
Materials and Method
A retrospective observational study was performed over
consecutive 2748 patients admitted to Intensive Care Unit of SL
Raheja Hospital, Mahim, Mumbai, and Maharashtra over period of
3 years from September 2015 to September 2018 after prior approval
from ethics committee of the hospital. All of them were included
provided they fell into the at risk criteria as suggested by either NRS-
2002 or the Nutric score (without the Interleukin-6). All the selected
patients were provided with complete powder based formula feeds
that was reconstituted under laminar airflow with drinking water.
In case of re-admission, only the first admission was considered.
Patients were transitioned to kitchen feeds only on the day that the
patients were getting shifted out from the intensive care unit.
All the patients received powder based specialized formula
feeds that were determined by computer generated sophisticated
algorithm called as the iNutrimon Software [10]. The iNutrimon
selected the type of formula feed (among all available formulae in the
hospital which included Nestle, Abbott, and Fresenius). The energy
and protein requirements were determined as per simple predictive
equations as per ASPEN guidelines (total calories at 25 kcal/kg and
protein at 1.5 g/kg). The software algorithm showed products or
at times combinations of two different formula feeds based on the
following criteria in descending order.
1. Best protein match for the water prescribed and that suggested
by the formula
2. Best calorie match for the water prescribed and that suggested
by the formula
The software suggested the number of scoops to be given with the
recommended volume for that particular feed and it also took into
account the fluid balance and requirement of the patient.
As per protocol the ICU uses continuous feeding with feeding
pumps. In the study, the cost of bags was not included in the data.
Also, at times patients were also given scientific feeding formulae orally inorder to “top up” the inadequacy in kitchen based oral diets.
When patient had started consuming at least 70 % of kitchen diet
orally scientific feeding formula were discontinued. This usually
coincided with the last day of stay in the Intensive care unit.
The feeding data were extracted from the patient file record from
the Medical Record Departments. The average feed was calculated by
sum total of the total number of scoops supplied per admission during
the overall length of stay in ICU divided by the number of scoops
supplied per tin of formula feed to know the number of tins utilized
per patient. Data so obtained were analyzed to get the relationship of
average length of stay to average cost of feed per day per patient.
The APACHE 2 score and length of intensive care unit stay of
all selected patients were noted by the date of first entry in nutrition
planner software considered as date of admission and date of
discharge from or death in ICU. In order to obtain the relationship
between the cost of feeding, length of stay and severity of illness,
the patients were distributed into 4 subgroups based on APACHE 2
scoring system - 3 to 10, 11 to 20, 21 to 30 and more than 31 and the
data were analyzed accordingly.
Results
Following Observations were drawn from this study:
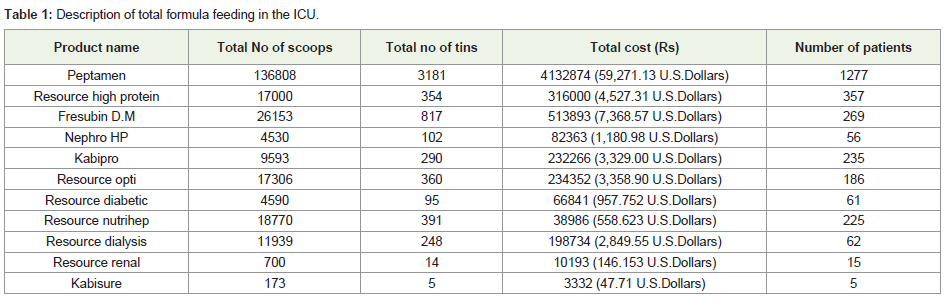
The inutrimon software probably selected Peptamen (Nestle)
(among all the available products as shown in Table 1) often probably
in view of specific nutritional requirement for ICU patients which
included conservative fluid management, high proteins and moderate
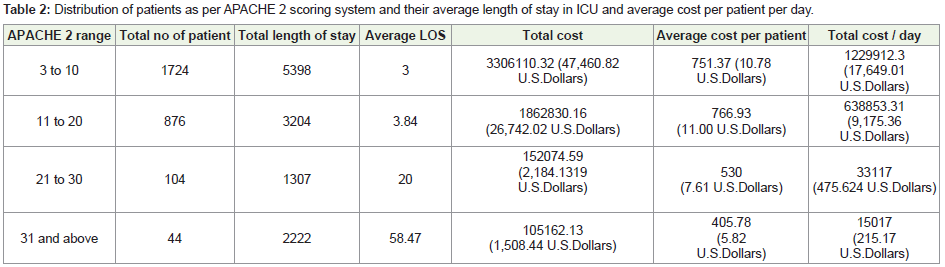
calories.Average length of stay was lesser in patients with APACHE 2
scores between 3 to 10 and 11 to 20 i.e., 3 and 3.84 respectively however
the cost of feed per day per patient 751 INR (10.8 U.S.Dollars) and
766.93 INR (11.03 U.S.Dollars) respectively. Whereas average LOS
was 20 days and 58 days for subgroups with APACHE 2 scores in the
range of 21 to 30 and 31 and above respectively. However average cost
per patient was 530 INR (7.62 U.S Dollars) per day and 405 INR (5.82
U.S.Dollars) per day for patients with APACHE 2 scores in the range
of 21 to 30 and 31 and above respectively (Table 2).
On comparison between the groups Average LOS was found to
be higher in patients in subgroups with apache scores more than 20
when compared with the subgroups with apache scores less than 20.
Also, the cost of formulae feed for patients with higher apache score
was found to be significantly lower than patients with lesser apache
scores.
Overall results indicated that the average cost of scientific feeding
formulae was 749 INR/day (10.77 U.S.Dollars) with average length of
stay for the entire population during the study period from September
1st 2015 to September 1st 2018 was 4.84 days.
It was also found that if the length of stay was greater than 5 days
then cost of formulae feeding was 325 INR (4.67 U.S.Dollars) /day
and if length of stay was less than or equal to 5 days the cost was
826 INR (11.88 U.S Dollars) /day (cost of feeding becomes more than
double if length of stay goes beyond 5 days - Table 3)

Discussion
Nutrition given early and by the enteral route is well established
in the ICU. In modern critical care, the paradigm shift from
‘blenderized kitchen feeds’ to the ‘formulae feed nutrition’ has now
a lucrative response in terms of health of critically ill patients aiding
in their faster recovery and lesser duration of stay in ICU. Choosing
the right enteral feeding formula at the right time have number of
positive implications. Early enteral nutrition reduces the risk of
infection in critically ill patients improves gut immunity and gut
function administered to post-operative patients of GI malignancies
as they can be subelemental [11-14], offers minimal or no feed
contamination as compared to blenderized kitchen feeds [15], lesser
chances of intolerance due to permissible osmolarity, early weaning
off from mechanical ventilator supports reduces the length of stay in
ICU and is cheaper than parenteral nutrition [16,17].
Cost factor plays a crucial role in a developing country like
India where less than 10% of the population is covered under health
insurance schemes, most people have to pay for the cost of treatment
and feeding from their pockets. So, the cost of formula feeds becomes
imperative here. The question to answer for which this study was
taken up was, whether early initiation of formula feed would affect
the length of stay in ICU and will it affect the cost of treatment to
critically ill?
In our study, all of the patients were completely fed over
formula feeds which was determined by a sophisticated computer
generated algorithm by “ inutrimon” software that selects the most
appropriate scientific feeding formula after taking into account the
anthropometry, present illness of the patient, his/her comorbities and
his/her severity of illness.
The results of the present study showed that the average cost
of scientific feeding formulae was 749 INR (10.77 U.S.Dollars)/
day with average length of stay for the entire population during the
study period from September 1st 2015 to September 1st 2018 was
4.84 days. It was also found that cost of feeding becomes more than
double if length of stay goes beyond 5 days. This correlation that we
found in our observational study has been established in the past by
Noseworthy TW [18].
It was established that, average length of stay was lesser in patients
with APACHE 2 scores between 3 to 10 and 11 to 20 i.e 3 and 3.84
respectively and the cost of feed per day per patient 751 INR (10.8
U.S Dollars)and 766.93 INR (11.03 U.S.Dollars) respectively. This
probably may be because of -
a) These patient tolerated feeds better
b) We were able to feed them early in the admission as they
probably did not need resuscitation
c) They probably were unable to finish the formula feed tin
supplied in the said days of stay in the ICU and hence the per day cost
(in the ICU) increased.
Whereas average LOS was 20 days and 58 days for subgroups with
apache scores in the range of 21 to 30 and 31 and above respectively.
However average cost per patient was 530 INR (7.62 U.S.Dollars)-per
day and 405 INR (5.8 U.S Dollars) per day for patients with apache
scores in the range of 21 to 30 and 31 and above respectively. This can
be attributed to -
a) These patients were fed less probably because the initial 48
hours would have gone without feeding in order to ensure reasonable
hemodynamic stability.
b) These patient would have had higher intolerance and hence
received lesser feeding
c) Many of these patients were ventilated and monitored via
indirect calorimeter and the measured calories required were found
to be much lesser
d) There were many episodes of iatrogenic underfeeding like visits
to CT scans and procedures etc where feeding was held resulting in
lesser consumption of feed and hence tins and hence cost.
As in our study average length of stay was lesser in patients with
APACHE 2 scores between 3 to 20 which can be supported by some
previous studies one among them is by SA Naved which stated that
there is an inverse relationship between the high APACHE II score
and the length of stay [18]. If the APACHE II score increased beyond
20 in our study the length of stay also increased accordingly which is
in accordance to studies by A Agarwal and SJ Theresa [18,19].
As to the best of our knowledge there is no such study taken up in
india till date which directly estimated the cost of scientific formula
feed, therefore this study could play a pivotal role by supporting
the facts that early initiation of feeding will result in lesser overall
cost of treatment and will benefit the patient above and better than
blenderized kitchen feeds.
Some of The Limitations Of This Study Are
1. This is a single centre observational study where the feed
prescription and monitoring is computer driven and hence probably
very tightly controlled with respect to achieving target goals of
calories and protein.
2. The authors ICU also used continuous feeding via feeding pump.
This may not be the cases in other ICU’s. Hence the generalizability to
all ICUs in INDIA may not be justified.
Concluding Remarks
This is probably the first Indian data on the cost of complete
scientific feeding formulae in the ICU. It does appear that lesser
the number of days the patient stays in the ICU more is the cost of
scientific formula feeding. However the cost of feeding per day is
much lesser than the cost of many others like antibiotics in the ICU.
References
Citation
Sanjith S, Apoorv T, Shah N. Cost of Enteral Formulae Feed in Critically Ill Patients in a Tertiary Care Centre: An Observational Study from India. Indian J Nutri. 2019;6(3): 207.