Research Article
Nutrition Assessment Using Serum Albumin and Change in Weight in Cancer Patients and Its Correlation with Post Operative Outcome
Subbiah S*, Gopu G, Hussain SA and Arulmurugan R
Department of Surgical Oncology, Government Royapettah Hospital, Kilpauk Medical College, India
Corresponding author: Subbiah S, Department of Surgical Oncology, Government Royapettah Hospital, Kilpauk Medical College, Chennai-600014, India, E-mail: subbaihshanmugam67@gmail.com
Citation: Subbiah S, Gopu G, Hussain SA, Arulmurugan R. Nutrition Assessment Using Serum Albumin and Change in Weight in Cancer Patients and Its Correlation with Post Operative Outcome. Indian J Nutri. 2019;6(1): 196.
Copyright © 2019 Subbiah S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Nutrition | ISSN: 2395-2326 | Volume: 6, Issue: 1
Submission: 11/01/2019; Accepted: 13/02/2019; Published: 16/02/2019
Abstract
Background: The Government hospitals in India cater to patients in low socioeconomic group. These patients due to a combination of factors are basically presumed to be nutritionally deprived. The fact that the level of nutrition and post operative healing is well documented by accepted protocols.
The government hospitals provide stay and diet to these patients free of cost. The stay of these patients before surgery is on an average around 10 days. During this period the length of stay with rest and nutritional improvement with concomitant impact on wound healing can be analysed.
Nutrition in cancer patients can be assessed using various methods. Serum albumin and prealbumin are widely used. Serum albumin co-relates with post operative morbidity and mortality of the patient.
Objectives: To compare the pre operative BMI, serum albumin levels with post operative levels and its impact on wound healing. To assess the nutritional supplementation in the hospital in a 10 day preoperative period.
Methods: One fifty nine cancer patients (Head and neck, gastrointestinal and gynec) admitted for surgery in our institute from October 2016 - December 2017 were evaluated pre operatively with serum albumin and BMI on admission. Serum albumin and BMI of the patient were repeated before surgery. All patients were provided with diet supplement as permissible in Government hospital. After evaluation patient underwent surgery. After surgery, serum albumin levels on first and fifth post operative day were noted. Post operative complications were noted and analysed.
Results: Of the 159 patients, 32 (20%) patients had serum albumin level less than 3.5g/dl. Age (avg = 52) (p = 0.21 for age > 70 vs. < 70 yrs) and sex (p = 0.12) had no significant difference in albumin levels of the patient. Body mass index less than 17.5 (p = 0.03), grade 3 (p = 0.005) post operative complications were associated with decreased albumin levels. Weight loss during hospital stay was associated with decreasing albumin levels (p = 0.001) and significant grade 3 complication (p = 0.037). Change in albumin levels did not correlate with grade of complications. More the duration of stay in hospital, more number of patients gained weight which correlates with decreased grade 3 complication. In oral cavity cancers, trismus and ankyloglossia had significant difference in albumin levels and post operative complications.
Conclusion: Albumin though not a specific marker for nutritional assessment, it is widely used because of availability and cost effectiveness. To conclude, serum albumin levels >= 3.5gm/dl at admission and increase in weight during hospital stay of more than 10 days is associated with decreased post operative complications.
Keywords:
Nutrition assessment; Albumin
Introduction
Nutrition is an important factor in postoperative wound healing. Reliable markers for nutrition are necessary to assess the nutritional status. This helps in identifying patients prone for post operative complications. These patients can be supplemented with nutritional support before and after surgery to reduce complications related to wound healing.
An extensive and diverse set of methods are available for assessing nutritional status in cancer patients. Each has its strengths and weaknesses. Among the most commonly employed are: (i) anthropometric measurements, e.g. weight change, arm muscle circumference, and triceps skinfold thickness; (ii) quantitative biochemical assays, e.g. serum albumin, transferrin, and nitrogen balance studies; (iii) Subjective Global Assessment (SGA) based on medical history and physical examination; Patient-Generated SGA (PG-SGA) adapted from the SGA specifically for cancer patients [1,2]. Many other nutritional parameters, including the Prognostic Nutritional Index, the Nutritional Risk Index, the Nutritional Screening Tool have also been used to attempt to risk stratify patients [2]. The utility of these nutritional screening tools has been evaluated by their ability to predict relevant clinical outcomes, such as complications, treatment response, survival, hospital Length of Stay (LOS), and higher costs of health care.
Protein is one of the important substances in the process of wound healing. Serum albumin provides a simple method of evaluating visceral protein levels. Malnutrition and inflammation suppress albumin synthesis. In an adult the normal range of serum albumin is defined as 3.5-5.0g/dl and levels < 3.5g/dl is called hypoalbuminemia. Serum albumin helps in assessing protein status in the surgical patient. Albumin measurement lacks sensitivity because its level can be altered in various diseases and may not always reflect current nutritional status, due to its long half life (20 days). Nonetheless serum albumin level has been validated as an excellent predictor of postoperative infectious and wound complications.
Other markers of nutrition assessment are serum pre-albumin, transferrin, retinol binding protein. These are acute phase proteins, a situation that would alter specificity for diagnosis of visceral protein malnutrition. Pre albumin and retinol binding protein are better tools for evaluating short term effects of nutritional changes because of their rapid turnover i.e. short half life. Serum transferrin, prealbumin and retinol binding protein levels are not routinely measured due to higher cost compared with serum albumin. Hence we use serum albumin in our study for assessing nutritional status of the patient.
Materials and Methods
A prospective study of 159 cancer patients (Head and neck, gastrointestinal and gynec) admitted in our institute from October 2016 - December 2017 were evaluated pre operatively with serum albumin and weight with BMI on admission. Ethical committee clearance was obtained for the study and there were no ethical issues for this study. All patients were given protein rich diet. Supplemental high protein diet was provided to the patients who had low albumin levels at admission. Serum albumin and BMI of the patient were evaluated before surgery. Pre operative Ryles tube feeding was given to patients who could not take adequate feeds orally. After evaluation patient underwent surgery.
After surgery, serum albumin status on first and fifth postoperative day were noted. Postoperative complications were noted and analysed using Clavien-Dindo classification.
SPSS software was used for statistical analysis with p <= 0.05 as the significance level.
Results
Of the 159 patients there were 97 males and 62 females (ratio 1.5:1). The average age of the group was 52.3 years (range 24 - 83 years).
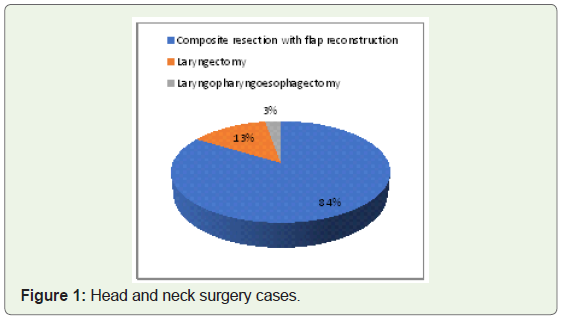
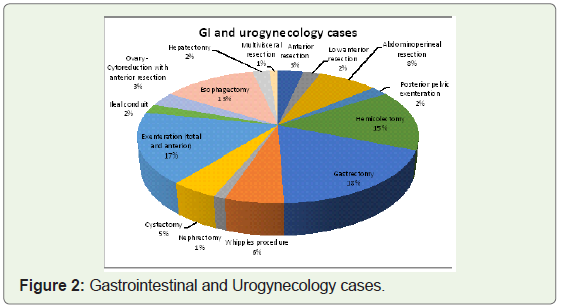
The disease characteristics are in Figure 1 and Figure 2.
Of the 159 patients, 32 (20%) patients had albumin less than 3.5g/dl. Age [< 70 vs. >= 70 yrs] (p = 0.21) and sex (p = 0.12) had no significant difference in albumin levels of the patient. There were 119 patients (75%) with body mass index of more than 17.5 and 40 patients (25%) with less than 17.5, comparing this with albumin levels BMI less than 17.5 was significantly associated with low albumin levels (3.5gm/dl) (p = 0.03) (Table 1).
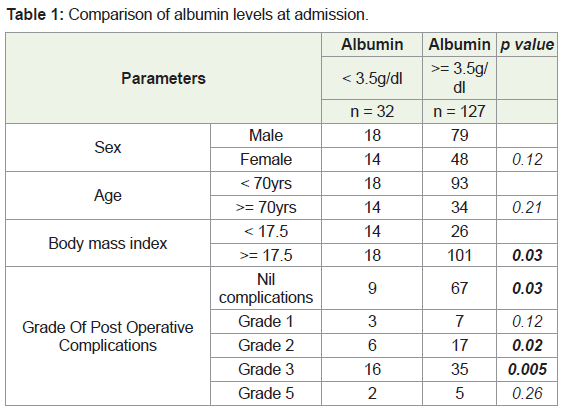
Post operative complications were analysed. Serum albumin levels less than 3.5gm/dl was associated with increased post operative complications. Of the 159 patients 76 patients had no complications and albumin levels more than 3.5gm/dl was associated with decreased complication rates [67 vs. 9] (p = 0.03). Grade 2 and 3 complications were seen in 23 patients and 51 patients respectively. Low albumin levels were significantly associated with increased grade 2 [6 vs. 17] (p = 0.02) and grade 3 complications [16 vs. 35] (p = 0.005). There was no significant association with grade 5 complications and low albumin levels. Five patients died during the same admission due to post operative complications [enterocutaneous fistula (n = 2), secondary hemorrhage (n = 2), neck wound dehiscence and carotid blowout (n = 1)].
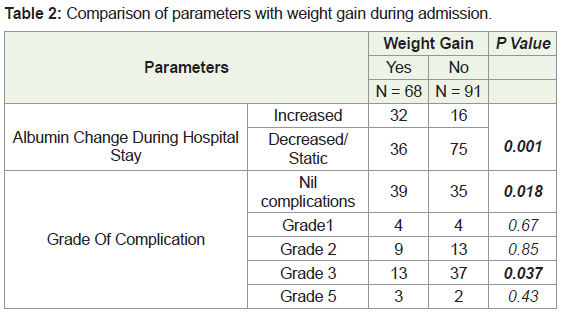
Sixty eight patients (43%) gained weight during their hospital stay before surgery. Weight gain of more than 0.5 kg during hospital stay was associated with significant increase in albumin levels (p = 0.001) and significant decreased post operative (grade 3) complication (p = 0.037) (Table 2).
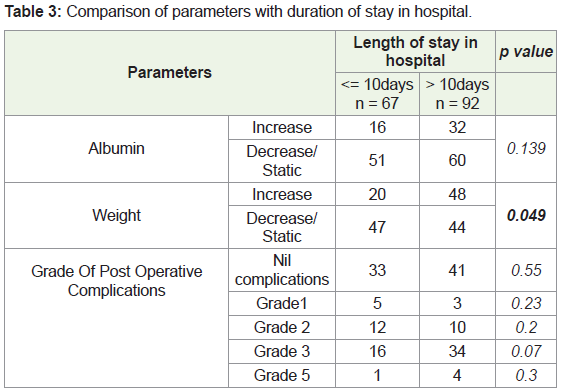
Of the 159 patients, 92 patients had their hospital stay more than 10 days for pre operative evaluation. Of the 92 patients, 48 (52%) had weight gain of more than 0.5kg (p = 0.049) and there was decrease in post operative complication who gained weight but was not statistically significant (p = 0.07) (Table 3).
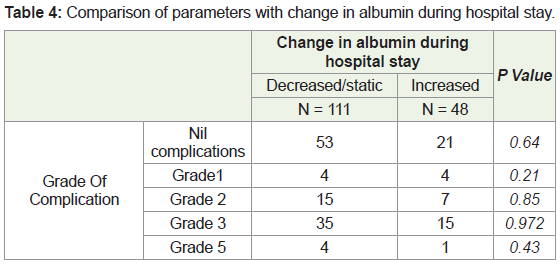
Forty eight patients (30%) showed increase in albumin levels and 111 patients (70%) had decreased or static albumin levels after admission in hospital. Change in albumin levels does not correlate with grade of complications (p = 0.25) (Table 4).
Of the 74 head and neck cancer patients 26 patients (35%) underwent post radiation salvage surgery showed statistically significant increased grade 3 and 5 complications (p = 0.005) when compared to primary head and neck surgeries. In oral cavity cancer patients (n = 62), 29 (46%) had trismus and 15 (24%) had ankyloglossia and were associated with decreased albumin levels and increased complications but not statistically significant (p = 0.21 and p = 0.11 respectively).
Discussion
In this study 32 (20%) patients had low serum albumin level (3.5gm/dl) on admission Low Body Mass Index (< 17.5 kg/m2) (25%) was associated with decreased serum albumin levels. A study by Schiesser M, et al. found a nutritional risk prevalence of 14.3% in surgical patients, and malnourished patients were three times more likely to experience complications and required significantly longer hospital stays than nourished patients [4]. Gupta D, et al. concluded that correcting malnutrition may decrease the length of stay in hospital in the post operative period and perhaps even lower the rate of hospital readmissions in this population [5].
In our study age and sex of the patient had no association with pre operative albumin levels. Schiesser M, et al. found that complications were strongly associated with disease severity and nutritional status, but not with age > 70 years [4].
Change in albumin levels during pre operative hospital stay was not associated with post operative complications. This may be due to posture-related effects (supine, sitting, standing) on serum albumin levels which is related to the alterations in hydrostatic and oncotic pressures with changes in body positions. This can lead to falsely elevated or diminished levels of albumin [3]. Another possibility is the longer half life of serum albumin which may not be reflected in alteration in albumin levels. Weight gain during hospital stay was associated with decreased complications. Other studies found an increased risk of complications in patients with recent weight loss.
Longer the length of stay in hospital in the preoperative period, more number of patients gained weight and less complications were noted. This is due to the fact that most of the patients referred to our institute from far areas of our state belonging to low socio economic status were provided with hospital based high protein diet. Also many patients who could not take adequate feeds orally were provided with feeding through Ryle’s tube, feeding jejunostomy tube, albumin supplementation (as 20% human albumin or fresh frozen plasma).
Isenring E, et al. showed that nutritional interventions significantly improve individual nutritional status [6].
To determine objective prevalence of malnutrition it is important to obtain nutritional status of every patient, which should include detailed personal history, prior medication, physical, anthropometrical and biochemical parameters [7].
The findings of this study reinforce the importance of assessing the nutritional status right after admission. These also indicate the need for developing and implementing protocols for nutritional screening, care, and monitoring during stay at the hospital. These protocols would enable the proposition of intervention strategies to improving patients’ clinical outcomes.
The limitation of the study is that albumin is not as sensitive as other markers but because of its cost effectiveness, we assessed nutrition status based on serum albumin levels. One study found that using serum albumin levels < 3.5g/dL as the sole parameter for malnutrition would have low specificity for identifying nutritional status in the functionally impaired elderly [8].
Other limitation is that the major sample population consisted of people from low economic background. Therefore, the long pre operative period of stay in hospital improved patient’s weight and nutritional status thereby reducing the complications. Hence futuristic studies should aim at conducting similar studies at private hospitals as well or in the people of sound economic status so that a concrete inference can be derived.
Conclusion
Albumin though not a specific marker for nutritional assessment, it is widely used because of availability and cost effectiveness. About one fourth of the patients admitted in our hospital were malnourished with low albumin levels. Normal albumin levels (> 3.5gm/dl) at admission and increase in weight of more than 0.5kg during hospital stay were associated with decreased post operative complications. Preoperative nutritional support after admission in hospital with protein rich diet will decrease post operative complications. Hence it is necessary to supplement protein rich diet for cancer patients in all government institutions during the pre operative hospital stay in order to reduce the post operative complications and overall health care cost by decreasing length of stay in post operative period.
References
- Gorman RC, Buzby GP (1997) Perioperative nutritional interventions. In: Shikora SA, Blackburn GL (eds.). Nutritional support: theory and therapeutics. New York: International Thomson Publishing pp: 91-112.
- Putwatana P, Reodecha P, Sirapo-ngam Y, Lertsithichai P, Sumboonnanonda K (2005) Nutrition screening tools and the prediction of postoperative infectious and wound complications: comparison of methods in presence of risk adjustment. Nutrition 21: 691-697.
- Hyltoft Petersen P, Felding P, Hørder M, Tryding N (1980) Effects of posture on concentrations of serum proteins in healthy adults. Dependence on the molecular size of proteins. Scand J Clin Lab Invest 40: 623-628.
- Schiesser M, Müller S, Kirchhoff P, Breitenstein S, Schäfer M, et al. (2008) Assessment of a novel screening score for nutritional risk in predicting complications in gastro-intestinal surgery. Clin Nutr 27: 565-570.
- Gupta D, Vashi PG, Lammersfeld CA, Braun DP (2011) Role of nutritional status in predicting the length of stay in cancer: A systematic review of the epidemiological literature. Ann Nutr Metab 59: 96-106.
- Isenring E (2013) Nutrition intervention improves nutritional status and quality of life outcomes in patients undergoing radiotherapy.
- Laviano A, Megiud RA, Meguid MM (2008) Nutrition support. In: DeVita VT, Lawrence TS, Rosenberg SA (eds.) DeVita, Hellman, and Rosenberg’s Cancer: Principles and practice of oncology. Lippincott Williams and Wilkins 2.
- Kuzuya M, Izawa S, Enoki H, Okada K, Iguchi A (2007) Is serum albumin a good marker for malnutrition in the physically impaired elderly? Clin Nutr 26: 84-90.