Research Article
Perioperative Artificial Enteral Nutrition in Malnourished Esophageal and Stomach Cancer Patients and its Impact on Postoperative Complications
Ramesh CS, Veerendra Kumar KV*, Arjunan R and Althaf S
Department of Surgical Oncology, Kidwai Memorial Institute of Oncology, India
Corresponding author: Veerendra Kumar KV, Department of Surgical Oncology, Kidwai Memorial Institute of Oncology, Bengaluru, India, E-mail: rameshcsagar@gmail.com
Citation: Ramesh CS, Veerendra Kumar KV, Arjunan R, Althaf S. Perioperative Artificial Enteral Nutrition in Malnourished Esophageal and Stomach Cancer Patients and its Impact on Postoperative Complications. Indian J Nutri. 2018;5(2): 190.
Copyright © 2018 Ramesh CS, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Nutrition | ISSN: 2395-2326 | Volume: 5, Issue: 2
Submission: 15/06/2018; Accepted: 16/07/2018; Published: 19/07/2018
Abstract
Introduction: The cancer is responsible for approximately 13% of all causes of death worldwide, however the death of almost 20% of cancer patients occurs as a result of malnutrition and its complications, rather than the malignancy itself. Malnutrition is common in gastrointestinal cancer patients, more so in cancer of stomach and esophagus. The causes are often complex and multi-factorial. Although it is widely accepted that malnutrition adversely affects the postoperative outcome of patients, there is little evidence that perioperative nutrition support can reduce surgical risk in malnourished cancer patients.
Materials and Methods: This prospective study was carried out from December 2016 to July 2017 at the Kidwai memorial institute of oncology Bengaluru. Within 48 h of admission, patients underwent nutritional assessment by the subjective global assessment. Perioperative nutrition was administered in the study group by enteral route only. Patients had a functioning gastrointestinal tract, and they received Enteral Nutrition (EN). Target intake of non-protein (25 kcal/kg per day) and protein (0.25 g nitrogen/kg per day) was provided using available enteral formulas. This was supplementary to standard hospital diet.
Results: Nutritional re-assessment after 15 days of intervention showed significant change in nutritional status, which was measured as gain in weight for each patient. There were significant differences in the mortality and complications between the two groups. The total length of hospitalization and postoperative stay of the control patients were significantly longer than those of the study patients.
Conclusion: In conclusion, perioperative nutrition support can decrease the incidence of postoperative complications in moderately- and severelymalnourished gastric and esophageal cancer patients. In addition, it is effective in reducing mortality. Enteral nutrition support, ALONE can be used in the management of malnourished patients undergoing gastric and esophageal surgery.
Introduction
The incidence of cancer is increasing worldwide and with it the prevalence of malnutrition, which may vary between 40 and 80% in patients with neoplasia [1,2]. The cancer is responsible for approximately 13% of all causes of death worldwide, however the death of almost 20% of cancer patients occurs as a result of malnutrition and its complications, rather than the malignancy itself [3,4].
Malnutrition is common in gastrointestinal cancer patients, more so in cancer of stomach and esophagus. The causes are often complex and multi-factorial and may be influenced by the location and type of tumor, stage of the disease, side effects of the treatment, socioeconomic status, functional performance, symptoms of nutritional impact, need for fasting and inadequate nutritional therapy, as well as medical staff awareness about the importance of nutritional status for the prognosis and quality of life of hospitalized patients [5-8].
Although it is widely accepted that malnutrition adversely affects the postoperative outcome of patients, there is little evidence that perioperative nutrition support can reduce surgical risk in malnourished cancer patients. Early retrospective studies suggested that perioperative nutrition support may effectively reduce postoperative complications [1,2]. Subsequent prospective, randomized clinical trials demonstrated that the benefits of perioperative nutrition support are limited to severely malnourished patients undergoing major surgery [3,4]. Most studies of perioperative nutritional support in patients with gastrointestinal cancer have shown that the degree of malnutrition varies considerably; unfortunately, studies in really malnourished gastrointestinal cancer patients are not available. Meanwhile, parenteral and enteral nutrition is still controversial in perioperative malnourished gastrointestinal cancer patients [5].
The aim of this study was to evaluate the efficacy of optimal perioperative enteral nutrition support in reducing complications and mortality in malnourished esophageal and stomach cancer patients.
Materials and Methods
This prospective study was carried out from December 2016 to July 2017 at the Kidwai memorial institute of oncology Bengaluru.
Inclusion criteria
Exclusion criteria
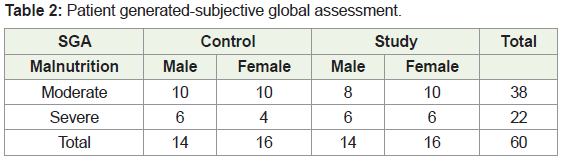
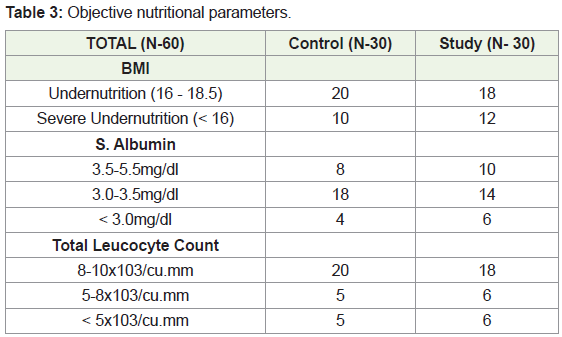
Within 48 h of admission, patients underwent nutritional assessment by the Subjective Global Assessment (SGA) performed with a standardized questionnaire including the patient’s history (weight loss, changes in dietary intake, gastrointestinal symptoms, and functional capacity), physical examination (muscle, subcutaneous fat, ankle edema, ascites) and the clinician’s overall judgment of the patient’s status (normal/ SGA-A, moderately malnourished /SGA-B or severely malnourished/ SGA-C). Objective value of weight, height, BMI, serum albumin and total leucocyte count were recorded. On the basis of these data, the patients were classified as well-nourished, moderately- malnourished or severely -malnourished. A total of 60 moderately malnourished and severely malnourished gastrointestinal cancer patients were included in this study.
After stratified for age, sex and tumor localization (gastric, esophageal), patients were divided into study group (n = 30, 14 women, 16 men) and control group (n = 30, 14 women, 16 men). The mean ages were 52 years (range 34-68 years) and 50 years (range 35-67 years) in the study group and control group, respectively.
Perioperative nutrition was administered in the study group by enteral route only. Patients had a functioning gastrointestinal tract, and they received Enteral Nutrition (EN).
EN was given to all 30 patients in whom GI function was adequate and administered through via a nasogastric tube or a feeding jejunostomy catheter. Target intake of non-protein (25 kcal/kg per day) and protein (0.25 g nitrogen/kg per day) was provided using commercially available enteral formulas. The initial rate of delivery was 40-60 mL/h, increasing stepwise to full intake for 48 h according to patient tolerance. Nutritional support was started 15-20 days before surgery. Nutritional status assessed once again at 15th day of starting nutritional intervention. Intervention started after 48 hrs of surgery, and continued for more than a week after surgery. This was supplementary to standard hospital diet.
Patients in the control group (n = 30) were given a standard hospital oral diet before surgery and a hypocaloric parenteral solution (1600 kcal non-protein and 60 g amino acid) in the postoperative period until gastrointestinal function recovered completely.
After surgery, patients were monitored daily for postoperative complications including septicemia, intra-abdominal abscess, wound infection, wound dehiscence, fistula formation, urinary tract infection, pneumonia, respiratory insufficiency and phlebitis. Rigid objective criteria were established defining each complication to avoid subjective bias. A diagnosis of septicemia was based on a positive blood culture, hypotension and hypoperfusion. An intra-abdominal abscess was defined as an intra-abdominal purulent collection requiring operative drainage. Fistulae were radiographically documented. A diagnosis of urinary tract infection required a quantitative culture of greater than 100 000 organisms. Pneumonia was documented by an abnormal chest x-ray, positive sputum culture, and treatment with antibiotics. The presence of a wound infection was defined by culture and operative or spontaneous drainage of purulent materials. A wound dehiscence required operative re-closure of the wound. The occurrence and cause of death during hospitalization and the length of hospitalization were recorded.
Statistical Analysis
Data were analyzed after submitting to a master chart. For normally distributed data, a paired Student’s t test was used for statistical analysis. P ≤ 0.05 was considered statistically significant. Data were expressed as mean ± SE.
Results
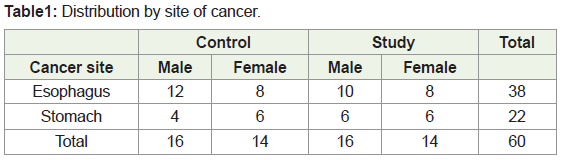
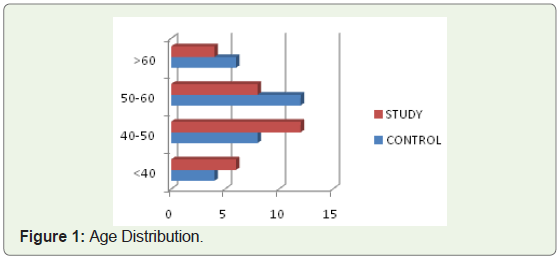
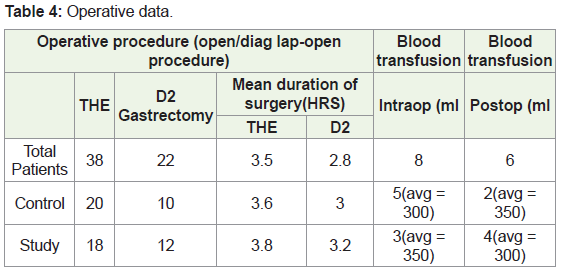
A total of 60 malnourished patients gave their consent to participate in the study. 60 were assigned at random to study group (n = 30, 14-women, 16-men) and control group (n = 30, 14-women, 16-men). Patient demographics and preoperative parameters of the two groups are presented in Table 1-3. There were no significant differences in mean age, sex distribution and nutrition status between the two groups (Figure 1). Operative data are listed in Table 4. The mean length of the surgical procedure and the volume of intraoperative blood transfusions were similar in two groups. The volume of postoperative blood transfusions was larger in control group. However, none of these differences was statistically significant.
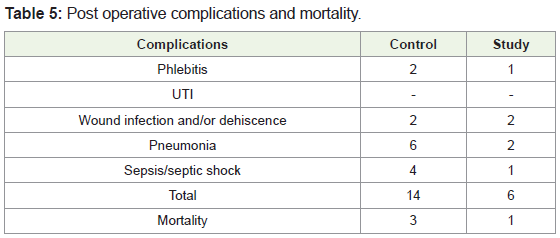
The number of postoperative complications per study group is shown in Table 5.
Preop and pre-interventional nutritional status of patients
Nutritional re-assessment after 15 days of intervention showed significant change in nutritional status, which was measured as gain in weight for each patient. Weight gain due to peripheral edema secondary to hypoalbuminemia not considered as weight gain.
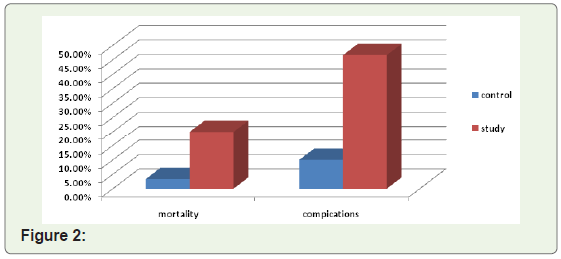
Complications occurred in 6 patients in the study group, and 1 patient died due to major complication. Complications occurred in 14 patients of the control group, and 3 patients died of major complications. There were significant differences in the mortality and complications between the two groups (3.33% vs. 9.99%, P = 0.003 for mortality; 19.98% vs. 46.62%, P = 0.002 for complications).
The total perioperative and postoperative median length of hospitalization was 8 days in the study group and 12 days in the control group, respectively. The total length of hospitalization and postoperative stay of the control patients were significantly longer than those of the study patients.
This study represents a small mono-institutional clinical trial to explore the role of perioperative nutrition support in moderately- and severely-malnourished gastrointestinal cancer patients. In these patients nutritional support was started 15-20 days before surgery and continued for more than a week after surgery. Nutrition was given by enteral route only. Postoperative complications were defined by rigid objective criteria to avoid subjective bias. This prospective study demonstrated that adequate perioperative nutritional support could effectively reduce the incidence of postoperative complications in moderately- and severelymalnourished gastrointestinal cancer patients. In perioperative nutrition support patients, there was a two-fold reduction in complications (P = 0.012) and a three-fold reduction in death (P = 0.003) (Figure 2). The most dramatic decrease was noted in major septic complications (14.9% vs. 27.9%, P = 0.011) such as pneumonia and wound infection. In addition, the mortality was statistically lower in artificial nutrition support group than in the control group (2.1% vs. 6.0%, P = 0.003). As a consequence of the lower infection rate, the length of hospital stay of the study group was shorter. These results indicate that malnutrition has a negative impact on postoperative outcomes, which may be efficiently controlled by a perioperative nutrition support that is adequate in quality, quantity, and duration.
Discussion
In this mono-institutional small study we observed nutritional re-assessment after 15 days of intervention showed significant change in nutritional status, which was measured as gain in weight for each patient. There were significant differences in the mortality and complications between the two groups. The total length of hospitalization and postoperative stay of the control patients were significantly longer than those of the study patients.
Malnutrition in hospitalized patients is a critical issue associated with a significant increase in morbidity and mortality. Recent surveys have demonstrated that 30 - 50% of hospitalized patients have a certain degree of malnutrition [6,7]. Malnutrition is closely associated with increased morbidity and mortality after major gastrointestinal surgery, especially oncological surgery. Perioperative nutrition support can restore many of biochemical and immunologic abnormalities in malnourished or normal state. However, it is difficult to demonstrate that perioperative nutrition support can significantly reduce surgical complications except in the most severely malnourished patients [8]. Early retrospective studies from 1970s to 1980s suggested that perioperative nutrition support can reduce surgical complications. Subsequent prospective, randomized trials demonstrated that the benefits of perioperative nutrition support are limited to severely malnourished patients undergoing major surgery [3,4]. Most studies of perioperative nutritional support in patients with gastrointestinal cancer have shown that the complication rate decreases from 56% in the control arm to 34% in the nutrition arm, with no deaths in the latter group [4,9]. Because nutrition support can only ameliorate but not reverse the catabolic response to trauma, it may effectively improve nutritional state and reduce postoperative complications when started preoperatively [10].
Perioperative nutritional support can be administered by PN or EN or their combination. PN has the advantage of easy administration and essentially immediate provision of optimal nitrogen and caloric requirements once the central venous access is established. A major concern with PN in hospitalized patients is the increased risk of septic complications related to immune dysfunction after PN. Unlike PN, EN is not associated with increased infectious complications. In fact, enteral feeding can maintain structural and functional integrity of the gastrointestinal tract and reduce septic complications in critically ill patients. The major disadvantages of EN support are the time delay when attempting to provide complete nutrition by the enteral route and the inability of patients with postoperative abdominal complications to tolerate enteral feeding. Early postoperative EN has fewer septic complications compared to early postoperative PN [11,12]. Unfortunately, studies in really malnourished cancer patients are not available. Excessive energy intake may result in hyperglycaemia and lead to increased septic complications and mortality [13,14]. In the present study, the prescribed target intake for EN patients was (25 kcal /kg per d and 0.25 g N/kg per d). In the present study, the route of feeding was dictated by ensuring adequate intestinal function, and simple NG tube feeding was sufficient. The results of this study are in accord with the recent studies [15,16].
Conclusion
In conclusion, perioperative nutrition support can decrease the incidence of postoperative complications in moderately- and severelymalnourished gastric and esophageal cancer patients. In addition, it is effective in reducing mortality. Enteral nutrition support, ALONE can be used in the management of malnourished patients undergoing gastric and esophageal surgery. Enteral nutrition has advantage of low cost, ease of administration and low septic complications compared to parenteral nutrition, and suited for patients with low BMI, low socioeconomic status.
References
- Von Meyenfeldt MF, Meijerink WJ, Rouflart MM, Builmaassen MT, Soeters PB (1992) Perioperative nutritional support: a randomised clinical trial. Clin Nutr 11: 180-186.
- Meguid MM, Curtas MS, Meguid V, Campos AC (1988) Effects of pre-operative TPN on surgical risk--preliminary status report. Br J Clin Pract Suppl 63: 53-58.
- Neumayer LA, Smout RJ, Horn HG, Horn SD (2001) Early and sufficient feeding reduces length of stay and charges in surgical patients. J Surg Res 95: 73-77.
- Bozzetti F, Gavazzi C, Miceli R, Rossi N, Mariani L, et al. (2000) Perioperative total parenteral nutrition in malnourished, gastrointestinal cancer patients: a randomized, clinical trial. JPEN J Parenter Enteral Nutr 24: 7-14.
- Bozzetti F (2002) Perioperative nutrition of patients with gastrointestinal cancer. Br J Surg 89: 1201-1202.
- Edington J, Boorman J, Durrant ER, Perkins A, Giffin CV, et al. (2000) Prevalence of malnutrition on admission to four hospitals in England. The Malnutrition Prevalence Group. Clin Nutr 19: 191-195.
- Waitzberg DL, Caiaffa WT, Correia MI (2001) Hospital malnutrition: the Brazilian national survey (IBRANUTRI): a study of 4000 patients. Nutrition 17: 573-580.
- McClave SA, Snider HL, Spain DA (1999) Preoperative issues in clinical nutrition. Chest 115: 64S-70S.
- Bozzetti F, Braga M, Gianotti L, Gavazzi C, Mariani L (2001) Postoperative enteral versus parenteral nutrition in malnourished patients with gastrointestinal cancer: a randomised multicentre trial. Lancet 358: 1487-1492.
- Hulsewé KW, Meijerink WJ, Soeters PB, von Meyenfeldt MF (1997) Assessment of outcome of perioperative nutritional interventions. Nutrition 13: 996-998.
- Moore FA, Feliciano DV, Andrassy RJ, McArdle AH, Booth FV, et al. (1992) Early enteral feeding, compared with parenteral, reduces postoperative septic complications. The results of a meta-analysis. Ann Surg 216: 172-183.
- Ashley C, Howard L (2000) Evidence base for specialized nutrition support. Nutr Rev 58: 282-289.
- McCowen KC, Friel C, Sternberg J, Chan S, Forse RA, et al. (2000) Hypocaloric total parenteral nutrition: effectiveness in prevention of hyperglycemia and infectious complications--a randomized clinical trial. Crit Care Med 28: 3606-3611.
- van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, et al. (2001) Intensive insulin therapy in critically ill patients. N Engl J Med 345: 1359-1367.
- Woodcock NP, Zeigler D, Palmer MD, Buckley P, Mitchell CJ, et al. (2001) Enteral versus parenteral nutrition: a pragmatic study. Nutrition 17: 1-12.
- Chung A (2002) Perioperative nutrition support. Nutrition 18: 207-208.