Research Article
The Effects of the Nutrient Deficiency in Oral Cavity Manifestation in Population of AL-Najaf City In-Vivo Study
Ibrahim SA1* and Hameed SA2
1Department of Prosthodontics, University of Kufa, Iraq
2Department of Oral Pathology, University of Kufa, Iraq
Corresponding author: Ibrahim SA, College of Dentistry, Assistant Professor Department of Basic sciences &Department of Prosthodontics, University of Kufa, Iraq, E-mail: drsanaaibraheem@yahoo.com
Citation: Ibrahim SA, Hameed SA. The Effects of the Nutrient Deficiency in Oral Cavity Manifestation in Population of AL-Najaf City In-Vivo Study. Indian J Nutri. 2018;5(1): 183.
Copyright © 2018 Ibrahim SA, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Nutrition | ISSN: 2395-2326 | Volume: 5, Issue: 1
Submission: 19/01/2018; Accepted: 05/03/2018; Published: 09/03/2018
Abstract
Aim: Clinical manifestations of nutrient deficiencies can have a significant impact on the function of the oral cavity. There are sever relationship between nutrition and oral health, which is multifaceted. Nutrient deficiency may result in oral symptomatology. Nutrition has both local and systemic impacts on the oral cavity. There are many factors effected the nutrient as age, sex, and pregnancy. Functional properties of the oral cavity include taste, salivation, mastication, and swallowing food.
Material and method: The study was carried out on 120 cases from hospitals and special clinics during period from October 2016 to May 2017 in Al-Najaf city. All patients had been involved in this study from both sexes, (90 females and 30 males, and 30 males control, 30 females control), females divided in pregnant women 50, the ages between 15-38 years and non-pregnant women 40, and the ages between 12-65 years.
Result and discussion: The results of this study showed that the people in the Najaf city they do have we founded there are many factors that affected the nutrient and then affected the oral manifestation later. The mouth is frequently the mirror of the body involved in conditions that affect the skin or other multi organ diseases. In many instances, oral involvement precedes the appearance of other symptoms or lesions at other locations.
Conclusion: Dentists and health professionals must recognize the manifestations of these deficiencies consider their causes and provide early treatment to prevent further compromise in nutrition status and to promote optimal nutrition, oral and overall health.
Keywords:
Nutrition; Manifestations; Vitamins; Nutrient deficiencies; Symptoms; Dental caries; Periodontal diseases; Hypogeusia; Angular stomatitis; Diabetes mellitus
Introduction
Nutritional science investigates the metabolic and physiological responses of the body to diet. These compounds provide that needs both energy and essential molecules for growth and maintenance.
Nutrients are the constituents of food necessary to sustain the normal functions of the body. The sequences of biochemical steps through which substances in living things change from one form to another. With advances in the fields of molecular biology, biochemistry, and genetics, the study of nutrition is increasingly concerned with metabolism and metabolic pathways. The human body contains chemical compounds, such as water, carbohydrates (sugar, starch, and fiber), amino acids (in proteins), fatty acids (in lipids), and nucleic acids (DNA and RNA). These compounds in turn consist of elements such as carbon, hydrogen, oxygen, nitrogen, phosphorus, calcium, iron, zinc, magnesium, manganese, and so on. All of these chemical compounds and elements occur in various forms and combinations (e.g. hormones, vitamins, phospholipids, and hydroxyapatite). Factors that influence the amount of a nutrient required to meet the needs
1- Age: the nutrients vary from infancy to adulthood. For example, adults required about 0.8g of protein per kg of body, whereas infants need over 2 g per kg.
2- Sex: for men are approximately 20% greater than those for women.
3- Other factors: for most nutrients are increased about 20-30% above normal in pregnant and lactation women. Patients with injury or illness also show increased requirements for some nutrients.
The relationship between nutrition and oral health is multifaceted. Nutrition has both local and systemic impacts on the oral cavity [1]. While diet and eating patterns have a local effect on the teeth, saliva and soft tissues, nutrition also has considerable implications and it gave a good assessment as a component of comprehensive care due to the systemic impact. Nutrients is essential to the growth, development, and maintenance of tissues, effectiveness of the immune system, prevention of cell damage and, in general, to increased resistance to many chronic, and some infectious diseases [1,2]. The oral cavity is often one of the first sites where nutrient deficiencies can be clinically noted.
Nutrient deficiencies can have a clinical manifestations and a significant impact on the function of the oral cavity. The function of oral cavity includes taste, salivation, mastication, and swallowing food. Any alterations in the structure and function of the oral cavity may compromise intake and contribute to the development of a nutrient-deficiency state.
Development of nutrient deficiencies
The oral cavity is a mirror of the body and has important anatomical location with a role in many physiologic processes, such as digestion, respiration, and speech. The mouth is frequently involved in conditions that affect the skin or other multi-organ diseases. In many instances, oral involvement precedes the appearance of other symptoms or lesions at other locations. An imbalance of supply and demand of nutrient will lead to deficiencies that is meaning, inadequate to meet the demands of the body [3].
Oral tissues, such as the gingiva (gums), bone, teeth, and muscles of mastication (chewing muscles), are living tissues, and they have the same nutritional requirements as any other living tissue in the body. A poor diet can have defect impact on health, causing deficiency diseases such as scurvy, health-threatening conditions like obesity and metabolic syndrome, and such common chronic systemic diseases as diabetes, osteoporosis, and cardiovascular disease [4].
Nutrient stores may be not reflecting in serum levels. If body stores are depleted, biologic and physiologic performance and cell functions became altered dependent on the specific nutrient [5].
Diet and nutrition play a key role in:
- Tooth development.
- Gingival and oral tissue integrity.
- Bone strength.
- Prevention and management of diseases of the oral cavity.
The medical history and presenting symptoms with examination is important to detecting deficiency conditions and possible causes. Any diseases can increase nutrient consumed and thereby leading to a deficiency. Infections in the oral cavity due to bacteria and fungus may alter tissue integrity, increase nutrient utilization.
Inadequate intake may be due to functional difficulties such as poor dentition, tooth loss, xerostomia, and systemic disease, as well as socioeconomic problems, anorexia, and depression, also prolonged poor dietary intake due to ill-fitting dentures and difficulties with mastication has been shown to result in inadequate intake of zinc, calcium, and B6 [6].
Under or low intake nutrition and oral health
Under nutrition may produce characteristic signs and symptoms in the oral cavity. The oral diseases associated with vitamin deficiencies are common in emerging “third-world” nations. In these countries, the limited supply of nutrient-dense foods or the lack of specific nutrients in the diet (vitamin C, niacin, etc.) may produce characteristic oral manifestations. In addition, unusual food practices, such as chewing sugar diet throughout the day or other regional or cultural nutritional practices may decrease the oral health of specific populations.
For example, in a typical B vitamin deficiency, a person may complain that the tongue is red and swollen and “burns” (glossitis), that changes in taste have occurred, and that cracks have appeared on the lips and at the corners of the mouth (angular cheilosis). In a vitamin C deficiency, petechiae (small, hemorrhaging red spots) may appear in the oral cavity, as well as on other parts of the body, especially after pressure has been exerted on the tissue. In addition, the gums may bleed upon probing with a dental instrument.
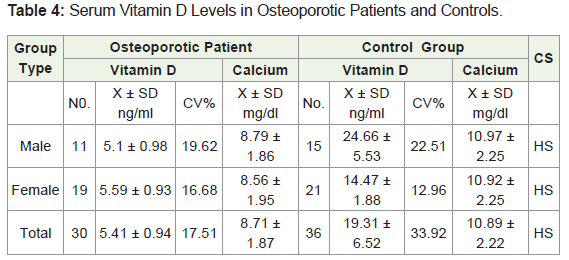
In humans, calcium deficiency causes the production of hypo plastic enamel (poorly mineralized enamel) similar to the osteoporosis produced in bone. Teeth appear to have a biological priority over bone when calcium is limited in the diet.
Material and Method
The study was carried out on 120 cases from hospitals and special clinics during period from October 2016 to May 2017 in Al-Najaf city, and 60 controls. All patients had been involved in this study from both sexes, the age between 12-65 years (90 females, 30 females control and 30 males, 30 males control), females divided in pregnant women 50, the ages between 15-38 years and non-pregnant women 40, and the ages between 12-65 years. The blood sample was collected from patients for analyzed to knowing the type of vitamin or any group deficiency, the patients were include poor and low socioeconomic style life.
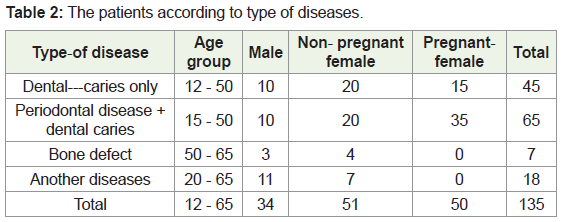
A-Dental caries only: Forty-five cases were obtained from patients (29 females and 13 males), the ages range between 12-50 years.
B-Periodontal disease + dental caries: Eighty cases were diagnosed clinically and dental X-ray (70 females and 10 males), ages range between 15-50 years.
C-Bone Defect: Thirteen cases were diagnosed clinically and by X-ray (4 females and 3 males), age was range between 50-65 years.
D-Another diseases of oral cavity: This group consists of twelve patients (11 females and 7 males), ages range between 20-50 years.
Statistical analysis
In this search the usual statistical methods were used in order to analyze and asses the obtained results.
Description statistics:
1-Statistical tables.
2- Arithmetic mean (x).
3-Standard Deviation (SD).
4- Coefficient of variation (C.V %).
Inferential statistics: These were applied in order to accept or reject the statistical hypothesis.
They include: 1-Student (t- test), in order to find the comparative significance (C. S.) between the two means for each contrast and determine it was highly significant (H. S.), significant (Si.), and not significant (N. S).
Aim of This Study
1-To assess the clinical relationship between the oral disease and systemic disease through the nutrient deficiency.
2-To improve the diagnosis of such systemic disease from oral manifestation and prevent missed diagnosis for such cases.
3-To improve the clinical treatment for such cases.
Results and Discussion
The results of this study showed that the people in the Najaf city they do have we founded there are many factors that affected the nutrient and then affected the oral manifestation later (Tables 1-9).

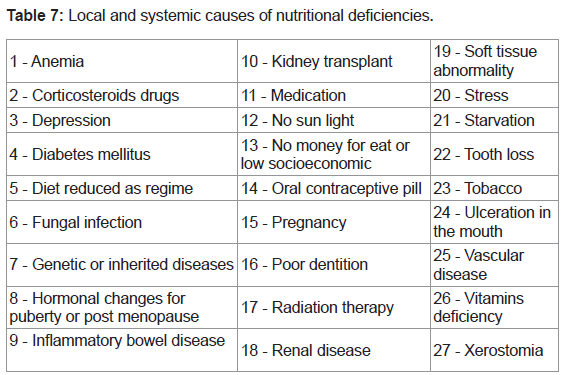
In this clinical study, the total number of these cases was 120; all of them were suffering from one or more of the following signs and symptoms as pain, bleeding tendency of gingiva, ulceration, loss of taste, burning sensation of tongue, difficulty in eating and swallowing, bad odor, decrease saliva, mobility of teeth, ugly teeth as discoloration, and those with dental caries for filling, extraction, and the lowest for the prophylaxis. These cases were including the following:
1-Patients with dental caries.
2-Patients with periodontal diseases (including pregnant women).
3 -Patients with diabetes mellitus.
4-Patients with kidney disease and kidney transplantation.
5-Patient with drugs induced problem.
6-Patient with bowel diseases.
7-Patient has liver diseases
8-Patient was taken chemotherapy.
9-Poor patient with low socioeconomic and patient doing diet regime.
The mouth is frequently the mirror of the body involved in conditions that affect the skin or other multiorgan diseases. In many instances, oral involvement considered the first location of many symptoms or lesions at other parts.
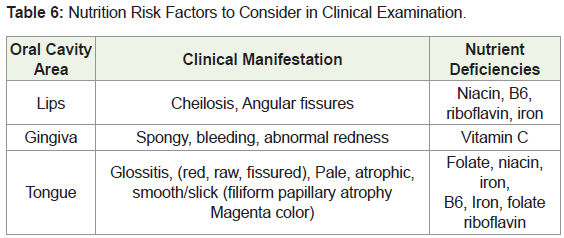
Nutrition risk evaluation was part of the scope of practice of all health professionals; early detection of risk for nutrient deficiencies during medical or dental exams, recognition of oral manifestations of nutrient deficiencies and other diseases [1,7,8]. There is a clear relation between oral health and nutrition. Nutrients plays a big role in maintaining the normal function of the oral cavity [1]. Nutrient deficiencies will cause oral defect and this alter dietary intake, resulting in deficiency states, malnutrition and poor wound healing following procedures or surgeries. Such cases as the following.
Anemia
Mucosal conditions, such as glossitis, recurrent aphthae, candidal infections, and angular stomatitis may be more common in patients with anemia. Glossitis may be the first sign of folate or iron or vitamin B12 deficiency. The tongue appears reddened, and the papillae are atrophic, producing a smooth appearance. Fatigue and decreased resistance to infection are common systemic symptoms. The oral mucosa exhibit pallor. This pallor is a common and easily recognizable feature of anemia.
Changes in the tongue
There are several changes that can occur on the tongue during nutrient deficiency states.
A painful, magenta colored, atrophic, smooth tongue is noted during a riboflavin deficiency. Glossitis may also be evidence of a vitamin B6, folate or B12 deficiency. However, during a chronic folate deficiency, the tongue papillae will become atrophied, resulting in a shiny, smooth surface appearance. Glossitis with loss of filiform papillae may also be seen in individuals with iron-deficiency anemia. A niacin deficiency results in a raw beefy, bright red, swollen, and painful tongue. Glossodynia may also be present in diabetes, resulting in painful mastication and swallowing.
Angular stomatitis and cheilosis
Stomatitis; inflammation of oral mucosa. Angular stomatitis (painful fissures at the corners of the mouth) and cheilosis (dry scaling of the lips and corners of the mouth) are common findings in riboflavin deficiency. Similar findings may be noted with niacin and B6 deficiency states. The similarity of these findings may be due to riboflavin’s role in B6 and tryptophan (which is converted to niacin) metabolism. Angular stomatitis, however, may be associated with iron deficiency anemia [9]. Angular cheilitis, however, is often associated with fungal infections, lip-sucking, and dehydration [10].
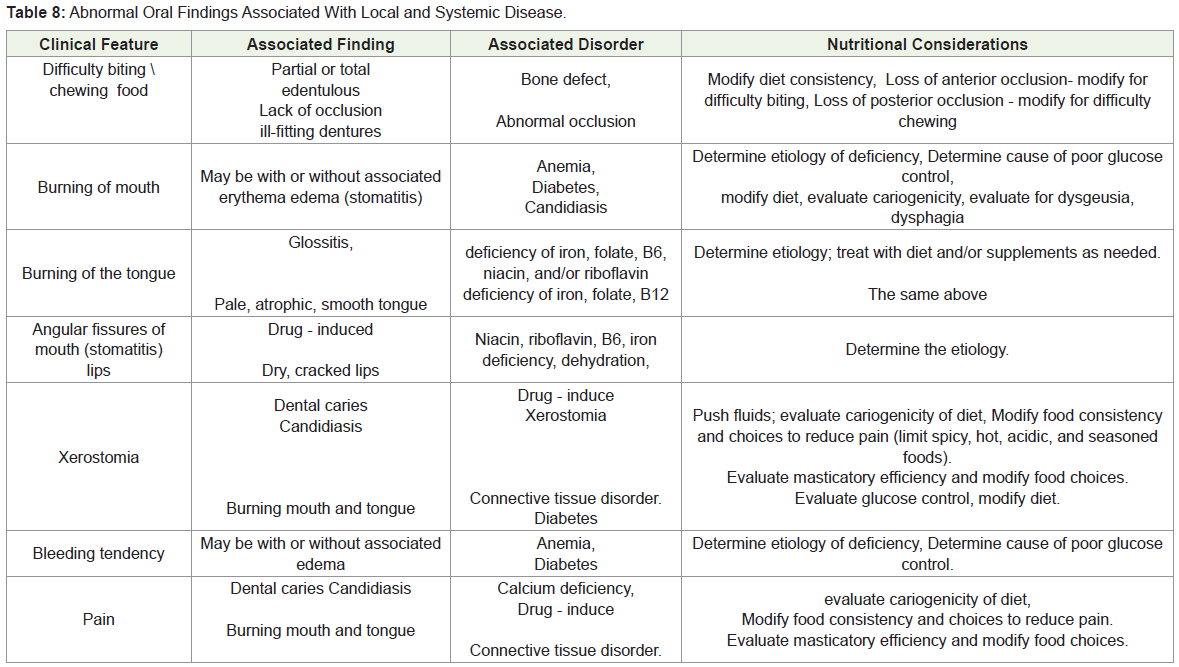
Oral manifestations of systemic diseases in relation to nutrient deficiencies:
Diabetes Mellitus
Diabetes mellitus is a systemic disease associated with delayed wound healing and oral manifestations which may alter nutrient intake and so affected the nutrition status. Poorly controlled diabetes mellitus is associated with glossodynia, xerostomia, candidiasis, gingivitis, periodontitis and altered taste [11-13] Up to 30% of individuals over the age of 19 with type 1 diabetes have periodontal disease [13]. Good oral health important in order for individuals to be able to consume a diet adequate for maintaining glycemic control, in order to restore oral and overall health.
(1 μg of vitamin D = 40 IU).
In our study we were found that many systemic conditions are known to adversely affect the mouth or teeth, and these patients require additional oral care and management so a dental evaluation should accompany the medical and psychological evaluation of a suspected eating disorder.
The diet of early modern humans varied significantly depending on location and climate. The diet in the tropics tended to be based more heavily on plant foods, while the diet at higher latitudes tended more towards animal products [14,15].
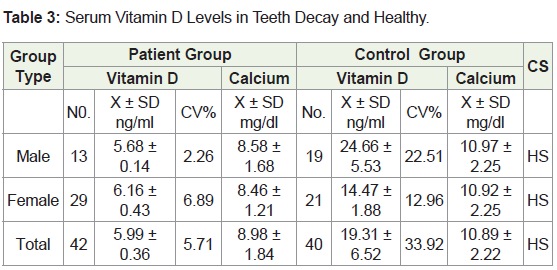
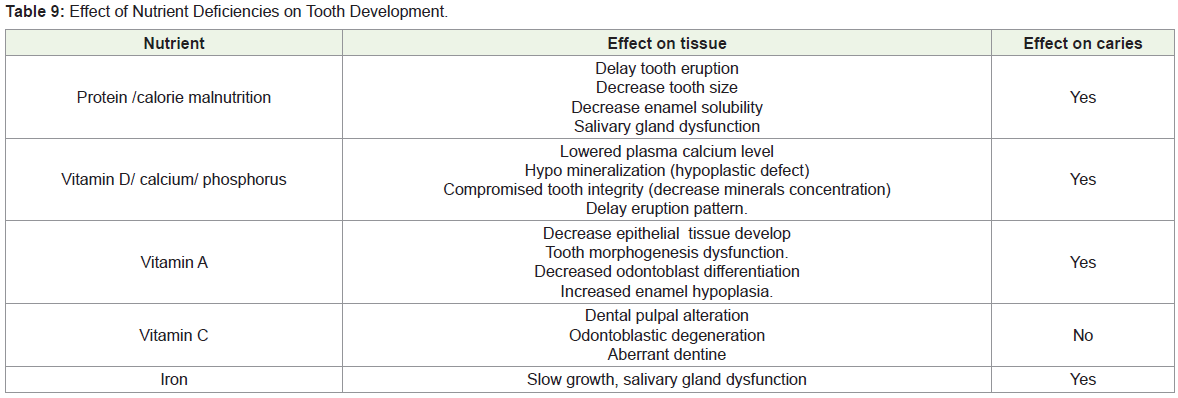
Effects of nutrient deficiencies on tooth development as dental caries:
Teeth are made from protein matrix that is mineralized with collagen (requiring vitamin C), calcium, and phosphorus to form a hydroxyapatite (requiring vitamins D and A).
The decay process was happened by plaque formation, sticky mix of microorganisms, protein, polysaccharides, and bacteria metabolizing fermentable carbohydrate produce acid. Acid production oral pH < 5.5 allows tooth demineralization. So gradual demineralization of enamel; proteolytic destruction of tooth structure as calcium and phosphorus, can be affected any tooth surface.
In our study especially our city due to social behaviors , due to several time war, because of terrorism, low socioeconomic, all this lead to poverty, physical destitution, hunger and lack of healthy food, also because religious reasons our women must cover all the body with black cloths, and wear a veil and sometimes black gloves when they go outdoors. These factors act as a good reason for preventing the people from taking a good healthy foods, so increased in nutritional deficiencies. This issue also was discussed as, they reported that “people of cultures such as Bedouins living in the Nagged Desert, who are required to have most of the skin surface covered by clothing, due to prevent them from exposed to the heavy sun light, are prone to develop vitamin D deficiency” [16].
Inadequate nutrition in the period from conception to approximately 12 years of age can affect the formation of enamel, causing pits and areas of roughness and these can be more susceptible to decay.
Research demonstrates that stress can make it more difficult for the body to fight off infection, including periodontal diseases; a diet which low in important nutrients can compromise the body’s immune, already know, tobacco use is linked with many serious illnesses such as cancer, lung disease and heart disease, as well as numerous other health problems.
We’ve probably heard a few old wives’ tales about pregnancy, including “A tooth lost for every child.” While it seems far-fetched, it actually is based loosely in fact.
Careful periodontal monitoring and excellent oral hygiene is especially important for women who may be noticing changes in their mouths during times of hormonal fluctuation. To help ensure good oral health.
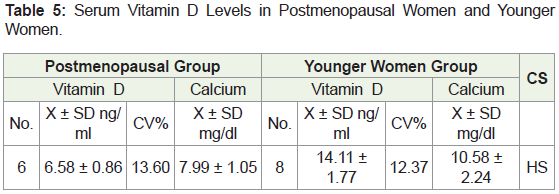
Pregnancy and contraceptive pill
The oral mucous membrane, and the gingiva, undergoes changes during pregnancy which, from clinical and histological observations, should be termed pregnancy gingival hyperplasia, gingivitis beginning in the second or third month of pregnancy that increases in severity throughout the eighth month. During this time, some women can notice nutrient deficiencies due to swelling, bleeding, redness or tenderness in the gum tissue; and diseases that interfere with the body’s immune system may worsen the condition of the gums. The gingival changes observed occasionally in women taking oral contraceptives may also be due to hormonal causes.
Women often become anemic during pregnancy because the demand for iron and other vitamins is increased. The mother must increase her production of red blood cells and, in addition, the fetus and placenta need their own supply of iron, which can only be obtained from the mother.
Most people in our society, carbohydrate food is the main meal to fill hunger, as well as the adaptation of fast foods that contain insufficient nutrients, the use of soft drinks and the lack of eating vegetables, fruits and meat and failure to eat food containing vitamins and minerals led to the emergence of sign and symptoms that represent lack of healthy nutrition and affect the health of mouth and teeth.
In a new study at January 2018 in University of Southern California, that pregnant women with vitamin D deficiency in first trimester may give birth to obese babies [17].
As mentioned, lifestyle- and obesity-related diseases are becoming increasingly prevalent all around the world. There is little doubt that the increasingly widespread application of some modern food processing technologies has contributed to this development. The food processing industry is a major part of modern economy.
Nutrition is taught in schools in many countries. In England and Wales the Personal and Social Education and Food Technology curricula include nutrition, stressing the importance of a balanced diet. However, statistics collected by the World Health Organization from 1990-2000 show in France may have been underestimated and, in fact, may be similar to that of neighboring countries [18].
In 1992, The U.S. Department of Agriculture introduced the Food Guide Pyramid. In 2002, a Natural Justice study showed a relation between nutrition and violent behavior. In 2005, a study found that obesity may be caused by adenovirus in addition to bad nutrition [19].
Dietary and physical activity guidelines from the USDA are presented in the concept of a food pyramid, which superseded the Four Food Groups.
The U.S. Department of Health and Human Services provides a sample week-long menu which fulfills the nutritional recommendations of the government [20].
Conclusion
1-The dentist must have a good experiences and social communication, and competence and caring for the patients.
2-Improving the awareness of nutritious meal choices and establishing long-term habits of healthy eating have a positive effect on cognitive and spatial memory capacity, potentially increasing a student’s potential to process and retain academic information.
3-It is important for physicians to recognize the link between systemic disease and oral findings. Some systemic conditions may first manifest with oral findings and a trained physician may detect and diagnose these conditions earlier, thereby initiating treatment sooner.
4-Patients experiencing this side effect should be monitored and encouraged to maintain good oral hygiene and frequent dental visits.
Acknowledgements
Just wishing to recognize the valuable help of all provided during my research. Without their care and funding, it was impossible to reach the goal. I would like to pay special thankfulness, warmth and appreciation to the persons who made my research successful and assisted me at every point. A lot of thanks also to my patients for acceptance to work with me in this research in order to get the benefit of research in our community. Last but not the least; emotional support can also be considered as a key to success. So, I wish to thank such supporters like my husband, daughters and sons, and friends.
References
- (1996) Position of the American Dietetic Association: Oral health and nutrition. J Am Diet Assoc 96: 184-189.
- Navia JM (1995) A new perspective for nutrition: the health connection. Am J Clin Nutr 61: S407-S409.
- (1994) Shils ME, Olsen JA, Shike M, editors: Clinical manifestations of human vitamin and mineral disorders: A resume Chapter 55. In: Modern nutrition in health and disease. 8th (eds). Philadelphia: Lea and Febiger pp: 909-923.
- Long RG, Hlousek L, Doyle JL (1998) Oral Manifestations of Systemic Disease. Mt Sinai J Med 65: 309-315.
- Beaton GH, Patwardhan VN (1976) Physiological and practical considerations of nutrient function and requirement. In: Beaton GH, Bengoa JM, editors. Nutrition and preventive medicine. Geneva: World Health Organization Monograph Series 62: 445-481.
- Sebring NG, Guckes AD, Li SH, McCarthy GR (1995) Nutritional adequacy of reported intake of edentulous subjects treated with new conventional or implant-supported mandibular dentures. J Prosthet Dent 74: 358-363.
- Heymsfield SB (1997) Nutrition support at the scientific frontier. JPEN J Parenter Enteral Nutr 21: 252-258.
- Maillet JO, Young EA (1998) Position of the American Dietetic Association: nutrition education for health care professionals. J Am Diet Assoc 98: 343-346.
- Sweeney MP, Bagg J, Fell GS, Yip B (1994) The relationship between macronutrient depletion and oral health in geriatrics. J Oral Pathol Med 23: 168-171.
- Brightman VJ (1994) Red and white lesions of the oral mucosa. In: Lynch MA, Brightman VJ, Greenberg H, editors. Burket’s oral medicine, diagnosis and treatment (9th eds). Philadelphia: JB Lippincott Co.
- Touger-Decker R, Sirois D. Dental health (1996) In: Powers MA. Handbook of diabetes medical nutrition therapy. Chapter 33. Baltimore: Aspen Publishers pp: 638-648.
- Emrich LS, Shlossman M, Genco RJ (1991) Periodontal disease in non-insulin-dependent diabetes mellitus. J Periodontol 62: 123-131.
- (1997) Centers for Disease Control. National diabetes fact sheet. Atlanta: Centers for Disease Control.
- Institute of Medicine (1997) Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride. Washington (DC): National Academies Press (US).
- Villa P, Bouville C, Courtin J, Helmer D, Mahieu E, et al. (1986) Cannibalism in the Neolithic. Science 233: 431-437.
- Taha SA, Dost SM, Sedrani SH (1984) 25-Hydroxyvitamin D and total calcium: extraordinarily low plasma concentrations in Saudi mothers and their neonates. Pediatr Res 18: 739-741.
- Daraki V, Roumeliotaki T, Chalkiadaki G, Katrinaki M, Karachaliou M, et al. (2018) Low maternal vitamin D status in pregnancy increases the risk of childhood obesity. Pediatr Obes.
- Ducimetière P, Lang T, Amouyel P, Arveiler D, Ferrières J (2000) Why mortality from heart disease is low in France. Rates of coronary events are similar in France and Southern Europe. BMJ 320: 249-250.
- (2006) Red Book: 2006 Report of the Committee on Infectious Diseases 27th (Eds). Pickering LK (ed): 831-835.
- (2007) Oral health in America: A Report of the Surgeon General. Rockville MD: US Department of health and human services, National Institute of Dental and Craniofacial research, National Institutes of Health; 2000.