Research Article
Challenges and Opportunities in Dietary Assessment of Pregnant Women in Tamil Nadu
Rajarajeswari K1*, Venugopal V2 and Saraswathy M3
1,3Department of Environmental Health Engineering, SRU- ICMR Centre for Advanced Research on Air quality Climate and Health, Sri Ramachandra University, Porur, Chennai, India
2Department of Environmental Health Engineering, Sri Ramachandra University, Porur, Chennai, India
Corresponding author: Rajarajeswari K, Department of Environmental Health Engineering, Sri Ramachandra University, Porur, Chennai-600116, India, E-mail:raji@ehe.org.in
Citation: Rajarajeswari K, Venugopal V, Saraswathy M. Challenges and Opportunities in Dietary Assessment of Pregnant Women in Tamil Nadu. Indian J Nutri. 2017;4(3): 165.
Copyright © 2017 Rajarajeswari K. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Nutrition | ISSN: 2395-2326 | Volume: 4, Issue: 3
Submission:17/05/2017; Accepted: 05/06/2017; Published: 20/07/2017
Abstract
The objective of this article is to describe the challenges in dietary assessment of pregnant women in Tamil nadu and identify opportunities for effective dietary assessment on maternal nutrition. Dietary assessment of 625 pregnant women visiting Government health facilities in Thiruvallur, Kanchipuram and Chennai district of Tamil nadu was done using a detailed Food Frequency Questionnaire (FFQ). Major challenges faced were length of the questionnaire, time taken to administer it & consequent participant fatigue and cultural practices. Gaps in diet recall, portion-size estimation, purposive under-reporting and lack of knowledge leading to over-reporting, were among other challenges. The challenges that were faced by the investigators were all reasonable and could be managed by some modification in the way the dietary assessments were conducted. Though the choice of using FFQ as a tool for dietary assessment for pregnant women is realistic, developing a concise questionnaire with pictorial representations and clues and/or use of food atlas to enhance recall and encouraging participants to report actual consumption will improve precision and accuracy of the dietary assessment for future studies.
Keywords:
Challenges; Dietary assessment; Pregnant women; Food Frequency Questionnaire
Introduction
Dietary pattern has been changing rapidly across the globe due to modernization/globalization and that does not preclude the Indian scenario in which has been the dietary changes have been tremendous in the past few decades. Maternal nutrition plays a key role in the period of human life cycle during which the fetus develops in the mother’s uterus. Maternal nutritional factors, both before and during pregnancy account for >50% of cases of LBW in many developing countries, has suggested that nutritional factors may account for 60% of the observed variation in birth weight [1]. Weight of the newborn is an indicator of infant growth and survival and this is in turn dependent on the maternal nutrition during pregnancy.
Dietary intake and nutritional status assessment provide critical information in understanding individual and community health status [2]. There are two methods of measuring dietary intake: Assessment by structured questionnaire and measurement by biochemical methods [3]. Dietary intake assessment is difficult and all dietary methods that assess the food intake of an individual or a group have their limitations and there is no method that is accurate and without error [3,4]. A comparison of dietary assessment methods used in few studies are listed in (Table 1). There are many motivating factors and barriers to diet intake during pregnancy which affect the nutritional status of pregnant women and thereby the growing fetus [5]. Apart from knowing the dietary intake, it is essential to understand the local practices, myths and beliefs of diet intake to elicit the accurate information on dietary assessment, especially with populations. Diet pattern analysis is, according to some authors, a better way to examine the effect of overall diet on problems related to nutrition and might well give some insight about the consumption of groups of food [6]. The review of dietary pattern and the detailed analysis of other nutrient consumption of populations are very important to approach the study of the relationship between nutrition and pregnancy outcomes.
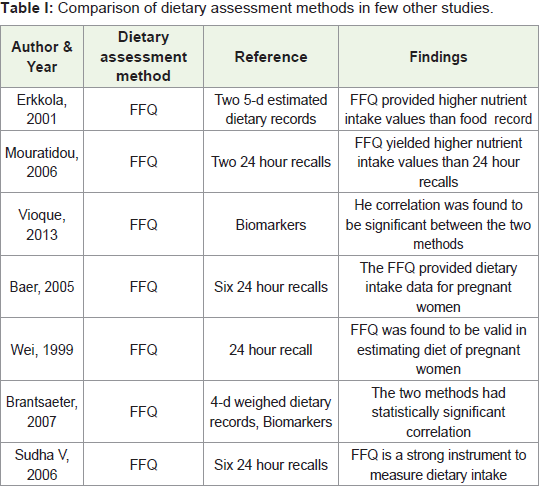
Table 1: Comparison of dietary assessment methods in few other studies.
Various techniques have been developed to obtain customary dietary intakes including the 24 hours dietary recall, diet history, Food Frequency Questionnaire (FFQ) and weighed food record. None of these methods is accepted as the gold standard method which can measure an individual’s nutritional intake and each has its own strength and weaknesses [7]. Biomarker assessment is said to be one of the best indicators of nutritional status which when combined with other methods of assessment, can become the near accurate method to assess the nutritional status of a pregnant woman [3,8]. In spite of its uncertainties, the most often used technique to assess diet in epidemiological studies involving large populations is the FFQ, due to its ease of use and capability to classify/analyze the specificity of food or nutrient intake [3]. A study on food intake measurement in scientists found that “very few subjects were able to accurately remember the types and amounts of food they had consumed in the previous 24 hours” [9]. If scientists are unable to recall what they have eaten in the past 24 hours, it is unreasonable to assume that a regular person would be able to accurately remember what she/he consumed days or months ago and this factor makes the nutritional assessment method very ineffective methodology. Participants usually modify their eating behavior when asked to record their intake (observation effect) and/or mis-report their changed eating behavior (reporting effect) [10].
A Food Frequency Questionnaire (FFQ) is a limited checklist of foods and beverages with a frequency response section for subjects to report how often each item was consumed over a specified period of time. Semi quantitative FFQs collect portion size information as standardized portions or as a choice of portion sizes. FFQs vary widely in the number of foods listed and their degree of specificity: They also differ in the method of soliciting frequency data and portion sizes. Some questionnaires provide frequency categories from which to select while others leave the frequency response open ended. Some FFQs also ask the respondent to estimate usual portion sizes [11].
Strengths of FFQ
FFQs are representative of “habitual” intake. It’s a preferable method of measuring intake for nutrients with very high day-to-day variability. Questionnaire processing is significantly less expensive than food records or diet recalls. FFQs can be easy for literate subjects to complete as a self-administered form and suitable for very large studies which are designed to rank individuals according to intake [12].
Weaknesses of FFQ
Administration of FFQ is a retrospective method that relies upon the respondent’s memory. It is less sensitive to measures of absolute intake for specific nutrients. Arbitrary groupings of foods may not correspond to the perception of the respondent. Exclusion of foods popular to particular minority groups that are significant contributors of nutrients will skew the data [12].
Use of FFQ as a Tool for Dietary Assessment forPregnant Women
FFQs are used to recall the diet intake for a specific period and it can be used as a dietary assessment tool for the most significant part of women’s life, that is, during their pregnancy, which gives good estimation of diet intake [13]. The FFQ allows us to identify the risk of malnutrition at an early stage, as early as pre conception or first trimester and suggest for timely correction and thereby improve the well being of the new born. Even though administration of FFQ could be time consuming and requires use of memory to recall the diet intake, it is one of the useful tools for dietary assessment of pregnant women especially to identify the diet pattern [3].
More studies are needed to assess the performance of FFQ as indicator of long term dietary intake using method of triad [14]. In this study, we administered FFQ as a dietary assessment tool to pregnant women of any trimester when they visit the health care facility for their regular check-ups.
Setting and participant recruitment
The participants were selected from the Primary Health Centers (PHC) of Thiruvallur and Kanchipuram district in rural areas and urban health posts of Chennai district. Women attending this government run facility are usually from the lower and lowermiddle socio economic class. In rural settings, employment rate of the women population is less relatively less compared to in urban settings, as majority of the pregnant women prefer to stay at home during pregnancy to avoid any pregnancy related complications due to travel and/or work.
Dietary assessment tool
FFQ, the most widely used tool in nutritional assessments, provides a lot of unique opportunities useful for practice in both rural and urban areas. The FFQ developed for the study, is suitable to elicit information from pregnant women of both rural and urban areas as there is not much variability seen in the diet pattern of the pregnant women across regions based on the pilot study done in the region.
The FFQ was designed in such a way that it captures the frequency of consumption of common food items, consumption of special diet for pregnancy and foods that are avoided by the pregnant woman along with the reasons for avoiding those items. The 114 food items in the FFQ are grouped as cereals, proteins (lentils & dhals), nonvegetarian foods, fats, oils and sugars, milk & milk products, fruits and vegetables. Questions to collect information about the vitamins and mineral supplements consumed by the pregnant women were also collected.
Changing consumer pattern and market, there was an induction of variety of foods from other states/countries that had a notable change in the intake of food by the pregnant women [15]. So the current trend of new foods like pizza and noodles, mostly consumed in the urban areas, were also added to the FFQ. It was observed that, both rural and urban women rarely reported intake of special pregnant food items and felt shy to respond to the questions related to intake of the western foods like “Pizza” in particular. The food items were divided into seven groups and the frequency of consumption of each item was given in the FFQ as per day, per week and per month with the average consumption for each of the listed item.
The FFQ was six pages in length and the respondents were made to sit comfortably and then were requested to answer the questionnaire. Each FFQ took roughly about 40-45 minutes to be completed and the respondents felt little uncomfortable sitting for such a long period and that too recalling the frequency of diet they had consumed over the past three months period.
Under-Over Reporting
Major challenge faced was to get a true estimate of the intake of balanced diet of pregnant women as some women tend to under-orover- report the intake due to various cultural factors. Though intake of dietary supplements was also captured by the FFQ, the resolution and accuracy of supplements intake could not be precisely estimated. Since the participants were recruited from the government primaryhealth centers or the urban health posts are supplied with free vitamin and mineral supplements during their antenatal visits, a bias was observed in participants to report falsely about the actual consumption of the vitamins. Many of the participants reported consuming the vitamins, though they did not consume it for various reasons, due to fear of losing the free supplement if otherwise reported.
Variation in diet intake in different trimesters
There is still an unclear picture about the diet pattern changes of a woman during pregnancy. The questionnaire administered towards the end of each trimester found a diet intake pattern that varied widely in different trimesters influenced by various factors that included media driven, physician’s opinion, family beliefs and pregnancy symptoms of the individual. So it was difficult to capture all the changes by interviewing once during their entire pregnancy to arrive at an estimate of the dietary intake during pregnancy. Our study observed that due to the symptoms of morning sickness, nausea and vomiting, first trimester women tend to eat less, but gradually improved their food intake during their second trimester. During third trimester, it was reported that the women tend to eat less for the fear of delivering bigger and heavier babies. An pilot attempt made to collect FFQs from the same individual for all the trimesters was not too successful for lack of time, resources and also due to the customary practice of the pregnant women moving to her parents’ place during the last trimester for delivering the child.
Lack of time and interest
Women have the responsibility of taking care of their family and have to complete all the household chores during the day and take care of the children in the family. Apparently they have limited time to spend in answering the questions for the study, especially if it is time consuming long questionnaire and if they have to tease their brains to remember their dietary intake from the past. Many women took part in the survey intermittently and while attending to their household chores which was a distraction in recalling their dietary intake from the past. The length of the questionnaire (which took approximately 40 minutes of their time) made them reluctant to spend that amount of time to answer the questions. Many women showed lack of interest half-way through the questionnaire in responding to the questionnaire and appeared distracted and some responded to the questionnaire in a hurry out of sheer courtesy which questions the reliability of their answers. Answers like “same as the other day/ same as breakfast” and “not much changed everyday” with an aim to complete the survey quickly were taken as indicators of unreliable responses. Clearly the participant fatigue was high due to the length of the questionnaire and the time taken to complete it.
A wide difference existed between the attitude of rural and urban women while answering the questionnaire. Rural women, even though they had multiple responsibilities, tried not to show their impatience due to fatigue or lack of interest. Urban women on the other hand, openly started questioning on the remaining time left for completion of the questionnaire and said they have work to be completed and would prefer continuing with the questions later or suggested answering over phone at a later time. In few instances, appointment had to be made in advance due to time constraints for the women to collect the data. Notably, some women were even hesitant to give the appointment to complete the questionnaire and in few instances the appointments were cancelled. The observation from study was that the assessment of diet of rural women was much easier to conduct and the data was much more complete than that of the urban women. Many women also expressed their desire for being compensated for their time spent for the interview and when found out that compensation was not made, lost interest in responding to the questionnaire and gave reluctant responses. Dietary advice, at the least, was one of compensations expected by the pregnant women for their time.
Myths and Beliefs
There are many traditional beliefs in Tamil nadu regarding certain foods that “should” or “should not” be eaten during pregnancy, such as avoiding black grapes, papaya, preparations with sesame seeds and chicken. The concept of ‘hot’ and ‘cold’ foods has a major influence on nutrient intake of pregnant women and also the quantity of food “to be consumed” in various trimesters [16]. Another myth was that revealing the special pregnancy diet and the quantity they consume during pregnancy might bring bad luck out of fear of “evil gaze”. Dietary supplements are provided by the Government to the pregnant women of all trimesters of pregnancy during each antenatal visit. Due to various cultural beliefs, pregnant women tend to avoid diet supplements, but report otherwise due to the anxiety of losing the benefit.
So the major challenge was to elicit the actual quantity of food consumed and nutrient intake of the pregnant women which had a huge bearing on the accuracy of the dietary intake assessment.
Opportunities for Better Dietary assessments inFuture
The shortcomings of the current methods adopted for dietary assessments for Indian pregnant women point to the fact that there are opportunities to improve the shortcomings by addressing the challenges experienced in the current study that could pave way for a robust method for use for pregnant women in South India. A short and concise FFQ tool kit could be developed for future studies of dietary assessment of pregnant women that may find wide spread acceptance among the target group. Interview by a trained dietician with further advice also might provide the motivation for the pregnant women to participate and feel satisfied or compensated for the time spent [17]. In government run facilities, apart from providing free supplements and consultation, there are multiple advantages of instituting a dietary assessment section for diet guidance/counseling for all pregnant women [18]. By such a facility, data on diet intake of the pregnant women can be easily recorded that could be the “goto” data source for understanding the changing patterns and trends in dietary intake and city/regional/state could be easily extracted for future nutritional studies and for policy prescriptions. An accurate dietary assessment can have greater implications in public health by understanding the gaps and implementing preventative programs for reducing nutrition-related complications of pregnancy. The end users of the government facilities in South India are mostly women from lower socioeconomic status who have limited access to latest technology. To bring about awareness and educating these pregnant women about well balanced nutrition is the need of the hour for a healthy future generation who form a strong foundation of the country. Further research in developing and assessing rigorous, robust but feasible dietary assessment methods are the need of the hour and merits further attention [19-24].
Conclusion
In this article, we have described the challenges faced in thedietary assessment of pregnant women in rural and urban settings of Southern India. Though the dietary data obtained from FFQ is reliable, they have their sets of challenges and short comings in terms of conducting it for a large cohort due to various factors, including social settings, and precision of the data collected in rural and urban settings. Though dietary assessment studies have the potential to add important perspectives to public health, they are laden with many pitfalls and factors to be considered when planning and carrying out diet and nutrition survey studies among pregnant women were identified that include the use of visual-aid reinforcement, involvement of key family members, the use of incentives and tangible benefits to reward study participants. A new modified short and concise FFQ tool kit including visual-aids for portion size could be developed and validated for use in large population studies that could benefit future studies and be advantageous in developing and strengthening the dietary database of pregnant women in southern India. It was also observed that data collection through the community health centers with trained dieticians might improve the reliability and accuracy of the quality of the data.
Acknowledgement
K.Rajarajeswari and M. Saraswathy were supported through funds provided by the Indian Council of Medical Research (ICMR) for the SRU- ICMR Center for Advanced Research on Air Quality, Climate and Health (SRU-CAR). Authors are grateful for the financial support provided by ICMR and the technical guidance provided by Dr. Kalpana Balakrishnan, Director, SRU-CAR, Dr. S.Sankar, HOD, Department of Environmental Health Engineering, SRU and members of the ICMR-CAR Advisory Committee, for the conduct of the field work. Authors are also thankful to the pregnant women who participated in the study. None of the authors had a conflict of interest.
References
- Kramer MS (2004) Maternal nutrition and adverse pregnancy outcomes: Lessons from epidemiology. In: Hornstra G, Uauy R, Yang X (Eds), The impact of maternal nutrition on the offspring. Karger Publishers, 55: 1-16.
- Wojtusiak J, Gewa CA, Pawloski LR (2011) Dietary assessment in Africa: Integration with innovative technology. Afr J Food Agric Nutr Dev 11: 5629-5645.
- Willett W (1987) Nutritional epidemiology: Issues and challenges. Int J Epidemiol 16: 312-317.
- Cade J, Thompson R, Burley V, Warm D (2002) Development, validation and utilization of food-frequency questionnaires- A review. Public Health Nutr 5: 567-587.
- Meltzer HM, Brantsaeter AL, Ydersbond TA, Alexander J, Haugen M (2008) Methodological challenges when monitoring the diet of pregnant women in a large study: Experiences from the Norwegian mother and child cohort study (MoBa). Matern Child Nutr 4: 14-27.
- Sarah R Crozier, Hazel M Inskip, Keith M Godfrey, and Siân M Robinson (2007) Dietary patterns in pregnant women: A comparison of food frequency questionnaires and four-day prospective diaries. Br J Nutr 99: 869-875.
- Thompson FE, Byers T (1994) Dietary assessment resource manual. J Nutr 124(11 Suppl): 2245S-2317S.
- Cuenca MH (2015) Food questionnaires and dietary recalls: The challenges of assessing food consumption to identify poor nutrition in a changing world. Adv Food Technol Nutr Sci Open J 1: 58-61.
- Todd KS, Hudes M, Calloway DH (1983) Food intake measurement: Problems and approaches. Am J Clin Nutr 37: 139-146.
- Wrieden W, Peace H, Armstrong J, Barton K (2003) A short review of dietary assessment methods used in National and Scottish research studies. Briefing paper prepared for: Working group on monitoring Scottish dietary targets workshop. Edinburgh pp. 1-16.
- Tefft ME, Boniface DR (2000) Estimating food and nutrient intake from food frequency questionnaire data by reference to a standard weighed diet survey. J Hum Nutr Diet 13: 219-224.
- Food frequency questionnaires.
- Robinson S, Godfrey K, Osmond C, Cox V, Barker D (1996) Evaluation of a food frequency questionnaire used to assess nutrient intakes in pregnant women. Eur J Clin Nutr 50: 302-308.
- Kabagambe EK, Baylin A, Allan DA, Siles X, Spiegelman D, et al. (2001) Application of the method of triads to evaluate the performance of food frequency questionnaires and biomarkers as indicators of long-term dietary intake. Am J Epidemiol 154: 1126-1135.
- Griffiths PL, Bentley ME (2001) The nutrition transition is underway in India. J Nutr 131: 2692-2700.
- Nag M (1994) Beliefs and practices about food during pregnancy. Econ Polit Wkly pp. 2427-2438.
- Garduñoâ€Diaz SD, Husain W, Ashkanani F, Khokhar S (2014) Meeting challenges related to the dietary assessment of ethnic minority populations. J Hum Nutr Diet 27: 358-366.
- Pérez-Rodrigo C, Escauriaza BA, Bartrina JA, Allúe IP (2015) Dietary assessment in children and adolescents: Issues and recommendations. Nutr Hosp 31 Suppl 3: 76-83.
- Erkkola M, Karppinen M, Javanainen J, Räsänen L, Knip M, et al. (2001) Validity and reproducibility of a food frequency questionnaire for pregnant Finnish women. Am J Epidemiol 154: 466-476.
- Mouratidou T, Ford F, Fraser RB (2006) Validation of a food-frequency questionnaire for use in pregnancy. Public Health Nutr 9: 515-522.
- Vioque J, Navarrete-Muñoz EM, Gimenez-Monzó D, GarcÃa-de-la-Hera M, Granado F, et al. (2013) Reproducibility and validity of a food frequency questionnaire among pregnant women in a Mediterranean area. Nutr J 12: 26.
- Baer HJ, Blum RE, Rockett HR, Leppert J, Gardner JD, et al. (2005) Use of a food frequency questionnaire in American Indian and Caucasian pregnant women: A validation study. BMC Public Health 5: 135.
- Wei EK, Gardner J, Field AE, Rosner BA, Colditz GA, et al. (1999) Validity of a food frequency questionnaire in assessing nutrient intakes of low-income pregnant women. Matern Child Health J, 3: 241-246.
- Brantsæter AL, Haugen M, Alexander J, Meltzer HM (2008) Validity of a new food frequency questionnaire for pregnant women in the Norwegian Mother and Child Cohort Study (MoBa). Matern Child Nutr 4: 28-43.