Research Article
Management of Hypertension in Normaland Obese Hypertensive Patients through Supplementation with Moringa oleifera Lam Leaf Powder
Edith N. Fombang1*, BlaiseBouba1 and Ngaroua2
1Department of Food Science and Nutrition, National School of Agro-Industrial Sciences, ENSAI, University of Ngaoundere, Adamawa Region, Cameroon
2Department of Biomedical Sciences, Faculty of Science University of Ngaoundere, Cameroon
Corresponding author: Edith N. Fombang, Department of Food Science and Nutrition, National School of Agro-Industrial Sciences, ENSAI, University of Ngaoundere, Adamawa Region, Cameroon, Tel: (+237) 675 19 57 86; E-mail:edfombang@yahoo.fr
Citation: Fombang EN, Bouba B, Ngaroua. Management of Hypertension in Normal and Obese Hypertensive Patients through Supplementation with 02 Moringa oleifera Lam Leaf Powder. Indian J Nutri. 2016;3(2): 143.
Copyright © 2016 Edith N. Fombang et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Nutrition | ISSN: 2395-2326 | Volume: 3, Issue: 2
Submission: 28/08/2016; Accepted: 28/09/2016; Published: 04/10/2016
Abstract
In order to contribute to the management of hypertension, this study investigated the effects of regular supplementation with Moringa oleifera leaf powder on blood pressure of normal and obese hypertensive patients attending the diabetes and high blood clinic of the Regional Hospital in Ngaoundere. Sixty hypertensive individuals aged 28-57 years participated in the study. They were divided into two groups; group 1 consisted of normal weight (25 women and 5 men, BMI = 21.97±2.15 Kg /m2) and group 2 of obese (25 women and 5 men, BMI= 32.33±1.10 Kg/m2) hypertensive patients. Anthropometric parameters, blood pressure and the frequency of urinary excretion were measured at the start of the study and once every 30 days for 6 months following daily supplementation with 30 g of M. oleifera leaf powder. At the end of the study, results show that, obese individuals benefited more from supplementation than normal weight subjects. Supplementation decreased body weight (3.2%), BMI (3.6%), waist circumference (2.5%), hip circumference (4.4%) more in obese group 2 compared to group 1, body weight (2.3%), BMI (2.3%), waist circumference (1.3%), hip circumference (2.9%). As concerns blood pressure, obese people again benefitted more with diastolic pressure dropping down by 14.63 mmHg (16%) in obese against 6.23 mmHg (7.3%) in normal weight subjects. With regards to systolic blood pressure, it decreased more 10.53 mmHg (6.5%) in normal weight compared to 6.86 mmHg (4.2%) in obese patients. Urine frequency increased significantly (p<0.05) in both groups. M oleifera leaf powder has hypotensive properties and promotes weight loss. Thus Moringa has an added advantage when used in the management of hypertension in obese patients.
Keywords: Moringao leifera; Hypertension; Normal weight hypertensive patients; Obese hypertensive patients; Dietary supplementation
Introduction
Today non-communicable diseases NCDs (cancer, chronicrespiratory diseases, diabetes and cardiovascular diseases CVD)constitute a serious threat to human health. They are the leading causes of death worldwide, responsible each year 60% of all deaths globally [1]. Of these, CVD is the leading noncommunicable disease; accounting for nearly half of the 36 million deaths due to noncommunicable diseases (NCDs), with 80% occurring in low and middle income countries [1]. Ten percent of global disease burden is attributed to CVDs, reason why WHO has developed a globalaction plan against these diseases [2]. The fight against cardiovascular disease has an important place in this plan, including the fight against high blood pressure (hypertension). This plan focuses on lifestyle modification and diet changes.
Hypertension is a key risk factor for cardiovascular disease [1]. Worldwide, hypertension is the third largest risk factor contributing to mortality after malnutrition and smoking [3]. It contributes to coronary heart disease and heart and kidney failure. The prevalence of hypertension is increasing in developing countries [1] possiblyin relation to the aging population, urbanization and changing food habits that promote obesity. Obesity is a risk factor for NCDs including hypertension.
Despite advances in the prevention and treatment of hypertension over the past decade, hypertension remains an important public health challenge. Recent efforts to reduce the prevalence of hypertension have focused on non-pharmacologic means, specifically diet [4]. Antihypertensive therapies always appeal to lifestyle changes, correction of associated metabolic disorders (hypercholesterolemia, diabetes) and various drug classes; but in spite of all these, hypertension is still on the rise.
The cost of care and management of hypertension remainselevated in our communities and consequently most persons are resorting to medicinal plants for a solution. Amongst the many traditional remedies used in the management and treatment of hypertension, Moringa oleifera, a plant native to India but widely cultivated in Africa has found its place among the ranks. It has been shown to possess hypotensive [5,6], hypocholesterolemic and antihyperlipidemic [4,7,8] properties. Most studies that investigatedthe hypotensive effects of M. Oleifera did not consider the weight statusof the patients in their study design; neither did they compare resultsin normal and obese patients. In addition to possessing hypotensive properties, M. Oleifera has also been shown to contribute to weightloss [9] and obesity is a risk factor for hypertension. This study was therefore designed to evaluate the effects of regular supplementation with Moringa oleifera leaf powder on blood pressure of normal and obese hypertensive patients.
Materials and Methods
Study Site
The study was carried out at the Ngaoundere Regional Hospital for a period of six months from March to September 2014.The study was done in collaboration with the health personnel working in thesaid clinic.
Sampling
The target sample for our study consisted of men and womencoming for consultation at the Diabetes and high blood pressure clinic at the Ngaoundere Regional Hospital. From this population, men and women at least 25 years old, hypertensive, obese (BMI > 30 kg/m2) or normal weight (BMI between 18.2 and 24.9 kg/m2), not pregnant, not on any medication for hypertension, not on a low salt diet, having a systolic blood pressure (SBP) of ≥ 140 mmHg and a diastolic blood pressure (DBP) of ≥ 90 mmHg, be available for regular weekly meetings and having given their informed consent to participate in the study by signing a consent form; were recruited for the study. All those who did not meet these criteria were excluded from the study. The study was approved by the ethics committee of the Ngaoundere Regional Hospital.
Execution of study
Following selection of subjects as per the inclusion criteria, 60 subjects were recruited and divided in to 2 groups of 30 persons each; Group 1, normal weight hypertensive individuals and Group2, obese hypertensive individuals. Baseline parameters for both groups were taken on day 1 and thereafter subject's diets were supplemented with 30 g of Moringa oleifera leaf powder daily. This powder was given to them weekly in sachets of 30 g representing a daily dose. The intervention period lasted for 24 weeks (6 months). Measurement of baseline parameters was repeated monthly for a total of 6 times throughout the duration of the study and values compared. Parameters measured were anthropometric (Age, weight, height, waist circumference, hip circumference, waist hip ratio) and clinical parameters (systolic and diastolic blood pressure; urine frequency).
Methods of Measurement
Measurement of anthropometric parameters
Weight was measured in kilograms using a mechanical balance (Camry brand) with a weighing capacity of 1 to 150 kg in 200gdivisions. The subjects were measured bare footed with minimal clothing.
Height was measured in meters using a stadiometer with a movable head piece graduated to 250 cm. The subject stands erect & bare footed on the stadiometer. The head piece is leveled with the skull vault and the height is recorded to the nearest 0.5 cm.
Body mass Index BMI was calculated using the formula.
BMI= Weight / Height2(kg/m2).
Following BMI measurements subjects were classified in to normal weight and obese based on the following classification [10].
BMI: 18.5 - 24.9 kg/m2 normal weight;
BMI > 30 kg/m2 obese.
Waist and hip circumference which are indications of fat distribution in the body were measured using a non-stretchable tape (type Oranta), length 150 cm, graduated to a millimeter. Waist circumference was measured at the level of the navel, while hip circumference was measured at the level of the hips, considering the area of largest circumference.
Waist Hip Ratio (WHR) was calculated as the ratio of the waist to hip circumference. A high WHR is an indication of central obesity which is a risk factor for heart diseases, hypertension and diabetes. This ratio varies with sex. A WHR greater than 90 in men and 80 in women is indicative of central obesity [10].
Measurement of Clinical Parameters
Measurement of Blood Pressure: Blood pressure was taken with the individual sitting and using a digital blood pressure monitor (Omron Hem 712C) with arm cuff. The individual was allowed to sitquietly for 10 minutes, and cuff pressure gauge and the strain saddledaround his arm. The apparatus was turned on. The reading was taken at the end of the operation from the display screen of the apparatus indicating the systolic pressure, diastolic pressure and the pulse.
Urinary Excretion Frequency:. The frequency of urination was measured monthly. A day prior to their monthly appointments, patients were asked to monitor their urine frequency and to note it. The base level was considered as zero and the increase above that calculated.
Preparation of M. oleifera powder
Moringa leaves were obtained from Maroua in the far North Region of Cameroon. Leaflets were detached from stems, washed with tap water, drained in plastic colanders and dried under shade (average temperature 27 ± 4 °C)protected from dust and insects with a mosquito net. Leaves were overturned periodically throughout the duration of drying which took between 3 to 4 days. Dried leaves were ground into powder using a hammer mill, packaged in sachets of 30 g each and stored in glass bottles away from light.
Statistical Analyses
Collected data was entered in to Excel (Microsoft cooperation Inc.)and means and standard deviations calculated. Analysis of Variance was carried out and means were separated using the Duncan's multiple range test at a probability level of 95% using Statgraphics Plus 5.0 software. Results are expressed as mean ± standard deviation.
Results
Anthropometric and clinical characteristics of patients
Both study groups are homogeneous in terms of gender (25women and 5 men each), height (1.67 m and 1.62 m for group 1 and 2 respectively), and age (41.10 and 41.37 years respectively for group 1 and 2) [Table 1]. As concerns weight, subjects in Group 1 had significantly (p<0.05) lower weights (61.43 ± 6.14 kg), compared to those in group 2 (84.83 ± 7.17 kg) consistent with the fact that group 1 was normal weight individuals while group 2 was made up of obese individuals. BMI, waist and hip circumference were significantly higher (p<0.05) in obese group 2 compared to normal weight group 1 [Table 1]. WHR on its part was comparable in both groups Table 2.
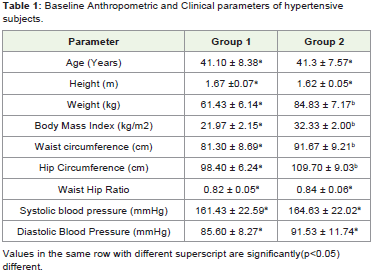
Table 1: Baseline Anthropometric and Clinical parameters of hypertensive subjects.
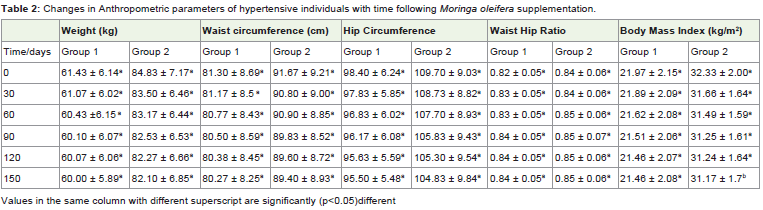
Table 2: Changes in Anthropometric parameters of hypertensive individuals with time following Moringa oleifera supplementation.
Both systolic and diastolic blood pressures were comparable in both groups. Systolic blood pressure was 161.43 mmHg in group 1 and 164.63 mmHg in group 2, whereas Diastolic blood pressure was 85.60 and 91.53 mmHg respectively in groups 1 and 2.
Changes in Anthropometric parameters with Moringa leafpowder supplementation
Supplementation of patients' diets with Moringa leaf powder over a period of six months brought about reductions in weight, waist and hip circumferences in both groups. Although these decreases were not significant they were slightly higher in the obese group 2 compared togroup 1. BMI on the other hand was significantly (p<0.05) reduced in group 2 after 6 months of supplementation with Moringa leaf powder. The reduction in BMI in group 1 was not significant. Waist hip ratio increased slightly with Moringa supplementation in both normal and obese patients.
>Changes in clinical parameters with Moringa leaf powdersupplementation
Important decreases were recorded in SBP and DBP over time in both groups with Moringa supplementation [Table 2]. Reductions were evident as from the first month of supplementation and continued throughout the experimental period. At the end of the 6 months intervention period, SBP decreased by 6.5% and 4.2% respectively in both groups 1 and 2, while DBP recorded a slightly higher drop (7.3% and 16% respectively in group 1 and 2). Decrease in DBP was significant (p<0.05) as from the fifth month in group 2.Urine frequency increased with consumption of Moringa oleifera leaf powder. These increases were however significant (p<0.05) only as from 90 days in group 1 and 60 days in group 2 [Table 3]. Compared to values at one month, urine frequency at the end of the six months study increased by 41.9% in group 1 and by 27.2% in group 2.
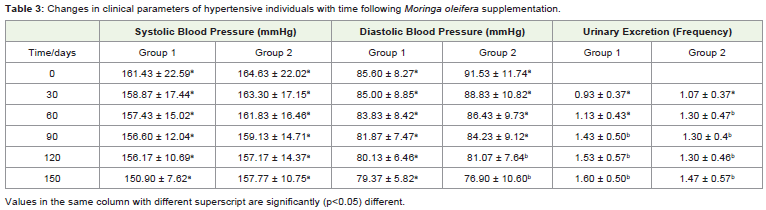
Table 3: Changes in clinical parameters of hypertensive individuals with time following Moringa oleifera supplementation.
Discussion
This study had as objective to investigate the effect on bloodpressure of supplementing Moringa oleifera leaf powder in diets ofnormal weight and obese hypertensive individuals. The two groups, normal weight hypertensive (Group 1) and obese hypertensive (Group 2) were homogeneous in terms of number, gender and height. The individuals in the group 2 weighed more given their obese status and consequently had a higher BMI (32.33 kg/m2)compared to normal weight group 1 (21.97kg/m2).Given that majority of the members in the groups were women, cut off values for women for waist and hip circumference, as well as WHR were considered in interpreting these results. In this regard, central obesity was present in both groups as indicated by their WHR which was above the risk threshold of > 0.8 [Table 1]. Central obesity is a risk factor for heart disease, hypertension and diabetes [10]. Values of systolic and diastolic blood pressure [Table 1] affirmed that these patients were hypertensive [1].
Regular consumption of Moringa has been shown to reduce cholesterol, triglycerides, LDL-C levels and body weight in animal models [4,7,8] and could explain the reductions observed in body weight, waist and hip circumference in this study considering that the subjects were not on any weight loss diet or medications. The loss in weight thus contributed to the reduction in BMI recorded in both groups. Naznin et al. [9] working on rats, observed a significant decrease in their body weight after intraperitoneal administration of decoctions of M. oleifera leaves for 8 days, and attributed this to reduction in serum triglycerides and cholesterol. Since fat accumulates around the waist and hip area, and reduction in fat with consumption of Moringa leaf powder has been reported [7], this could explain the drop in waist circumference (WC) and hip circumference (HC) following supplementation. HC decreased more (2.9 and 4.4%) compared to WC (2.4 and 1.2%) in groups 1 and 2 respectively. WHR on the contrary appeared to increase slightly possibly as a result of the higher decrease in HC compared to WC. The higher differences observed with the obese group 2 compared to group 1 may be related to the fact that the obese group have more stored lipids and cholesterol and as such the effect on these components is more evident in them.
Daily supplementation of patients diets with Moringa leaf powder was beneficial as it significantly (P<0.05) reduced systolic and diastolic blood pressure in both groups, although only DBP was reduced down to normal levels (< 80 mmHg) at the end of intervention.
Moringa leaves contain tannins and flavonoids which are known to increase capillary resistance, venous tone and stability of collagen.They have inhibitory activities on decarboxylase, elastase and angiotensin converting enzyme thus reducing circulating angiotensin[4,11]. These properties contribute to the efficacy of Moringa oleifera leaf powder in reducing blood pressure in hypertensive individuals. Moringa leaves equally possess antioxidant properties which could fight oxidative stress; a contributing factor to hypertension [1,5]. Flavonol quercetins of dried M. oleifera leaves have equally shown anti-dyslipidemic, hypotensive, and anti-diabetic effects in obese Zucker rat model with metabolic syndrome. Its hypotensive effect has been confirmed in human studies [4].
Increase in urinary frequency implies much water and possibly sodium is eliminated from the system and consequently blood pressure is reduced [12]. This could also be one of the mechanisms by which Moringa leaf powder lowers blood pressure. Tejas et al. [13], mentioned that ingestion of a decoction of M. oleifera leaves increased urinary output in rats.
Moringa’s widespread combination of diuretics along with lipid and blood pressure lowering properties make it useful in managingcardiovascular diseases. Its blood pressure lowering effect has been attributed to isothiocyanates and thiocarbamate glycosides, hypotensive principles that have been isolated from Moringa leaves [5,6]. Moringa’s high content of potassium may also be a contributing factor to its hypotensive effect as documented evidence shows that diets high in potassium and potassium supplementation significantly lower blood pressure [14].
Conclusion
This study highlights the fact that Moringa oleifera leaf powder could be used as a hypotensive in the management of hypertension;and more especially that obese hypertensive patients could benefit more from using this powder as it additionally promotes weight loss thereby improving its efficacy as a hypotensive.
Thus consumption of Moringa leaf powder could be beneficialfor weight loss and reducing blood pressure as well as for preventingother diseases which have obesity as risk factor. Obese subjects couldderive important benefits from consuming Moringa powder.
References
- World Health Organization (2013) A global brief on Hypertension. WHO Press, Geneva, Switzerland.
- World Health Organization (2013) Global action plan for the prevention and control of noncommunicable diseases 2013-2020. WHO Press, Geneva, Switzerland.
- Murray CJL (2015) Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 386: 2287-2323.
- MbikayM (2012) Therapeutic potential of Moringa oleifera leaves in chronic hyperglycemia and dyslipidemia: A review. Front Pharmacol 3: 24.
- Biswas SK, Chowdhury A, Das J, Roy A, Hosen SMZ (2012) Pharmacological potentials of moringa oleifera lam.: a review. International Journal of Pharmaceutical Sciences and Research 3: 305-310.
- Kumar PS, Mishra D, Ghosh G, Panda CS (2010) Medicinal uses and pharmacological properties of Moringa oleifera. International Journal of Phytomedicine 2: 210-216.
- Oinam N, Urooj A, Preetham PP, Niranjan NP (2012) Effect of Dietary Lipids and Drumstick Leaves (Moringa oleifera) on Lipid Profile and Antioxidant Parameters in Rats. Food and Nutrition Sciences 3: 141-145.
- Ghasi S, Nwobodo E, Ofili JO (2000) Hypocholesterolemic effects of crude extract of leaf of Moringa oleifera Lam in high-fat diet fed Wistar rats. J Ethnopharmacol 69: 21-25.
- Naznin A, Mamunur R, Shah A (2008) Comparison of Moringa oleifera leaves extract with atenolol on serum triglyceride, serum cholesterol, blood glucose, heart weight, body weight in adrenaline induced rats. Saudi Journal of Biological Sciences 15: 253-258.
- Whitney E, Sharon RR (2011) Understanding Nutrition. (12thedn) Belmont, CA: Wadsworth, pp 620-625.
- Khurana S, VenkataramanK, Hollingsworth A, PicheM, Tai TC (2013) Polyphenols: benefits to the cardiovascular system in health and in aging. Nutrients 5: 3779-3827.
- Shah SU, Anjum S, Littler WA (2004) Use of diuretics in cardiovascular disease: (2) hypertension. Postgrad Med J 80: 271-276.
- Tejas GH, Joshi UH, Bhalodia PN, Desai TR, Tirgar P (2012) Aparanomic view on pharmacognostic, pharmacological, nutritional, therapeutic and prophylactic values of Moringa oleifera Lam. International Research Journal of Pharmacy. 3: 1-7.
- Houston MC, Harper KJ (2008) Potassium, magnesium, and calcium: their role in both the cause and treatment of hypertension. J Clin Hypertens (Greenwich) 10(7 Suppl 2): 3-11.