Research Article
Community Perception and Acceptance ofMicronutrient Fortified Complementary Food in Integrated Child Development Services (ICDS), Gujarat, India
Nakkeeran N1, Chaturvedi A2, Bhagwat S3, R Sankar4 and Patel R5
Corresponding author: Dr. N. Nakkeeran, Indian Institute of Public Health Gandhinagar, Sardar Patel Research Campus, Drive-in Road, Thaltej, Ahmedabad-380054, Fax: 91 79 40240445, Ph: 91 79 40240444;; E-mail: nnakkeeran@gmail.com
Citation: Nakkeeran N, Chaturvedi A, Bhagwat S, Sankar R, Patel R. Community Perception and Acceptance of Micronutrient Fortified Complementary02 Food in Integrated Child Development Services (ICDS), Gujarat, India. Indian J Nutri. 2015;2(1): 107.
Copyright © 2015 N. Nakkeeran et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Nutrition | Volume: 2, Issue: 1
Submission: 03/06/2015; Accepted: 06/30/2015; Published: 08/07/2015
Abstract
Background: Fortification of complementary food is seen as a potent intervention to address child malnutrition. Government of Gujarat introducedBalbhog; an extruded fortified blended “a pre-cooked, cereal-based supplementary food in powder form”, to promote complementary feeding in 2007-08.Thestudy aimed to understand community perception, acceptance and practices associated with Balbhog.
Methods:The study used Focus Group Discussions for data collection involving mothers feeding Balbhog to their 6-36 months old children and in-depthinterviews with women who were non-users. Data were collected from four districts, representing four of the six regions of Gujarat.
Results: The study found that Balbhog was acceptable to most women and their children. Women had a strong recall about the product and its ingredients.Many caregivers attributed possible improvement in children’s appetite and weight gain to the product. Quick preparation time and ease in cooking were otherreasons for acceptance. Balbhog was being made available but often not in stipulated quantity and mothers were not aware of their entitlement. The frequencyof feeding differed across caregivers. The common practice was to feed children on demand. Targeting the product to under-three year children emerged as achallenge. Often the product was not perceived as ‘ready-to-eat’ instead caregivers improved the preparation by adding additional ingredients. The quality ofthe product, preference for homemade food and a perception that Balbhog is meant for poor were barriers highlighted by non-users.
Conclusion: Acceptance and usage of Balbhog depends on product features, its availability, ease in preparation and social evaluation of the product.There is a significant scope to improve the availability of the product within the entitled amount. There is also a need for nutrition counselling on Balbhog toimprove its initiation at appropriate age, improve consistency, frequency and quantity of its feeding and focusing the feeding to targeted age groups.
Keywords: Micronutrient fortification, Complementary feeding, Qualitative method, India
Introduction
Traditional complementary foods provided to children in theage group of 6-36 month are most often cereal based [1] and dietarylipids, proteins and micronutrients such as iron, zinc and calcium are low in these foods [2]. Bioavailability of such micronutrients in cerealbased diets is usually low [3]. A national level survey has shown thatamong children of 1-3 years age group the average daily intake ofcereals, millets, pulses, green leafy vegetables, milk and milk products,fats and oils in India is significantly lower than the Recommended Dietary Intake [4].Given these facts the nutrient and energy density ofcomplementary food have to be increased to meet the requirementsof children in 6-36 month age group. Fortification of staple foodgrains like wheat and rice is not a suitable strategy as the quantityconsumed by children of this age group is too small to provide therequired level of micronutrients [1]. For instance, NFHS-3 showedthat only 41 percent of the 6-23 months old children are fed semisolidfoods adequate number of times in Gujarat and appropriatefeeding practices are followed for only two out of ten children [5]. Forthese reasons fortified complementary food is being seen as a potentintervention in developing countries to address child malnutrition[1,3,6,7].
Studies from a number of developing countries have shownthat, among selected groups, fortified complementary feeding, eitheralone or in association with other interventions has positive effecton improving micronutrient status, anaemia status [8-14], height[11] and underweight [12]. In addition, these literature have alsopointed to a number of behavioural, cultural and logistical issuessuch as frequency of feeding, acceptance, social values attachedto foods, palatability, cost, ability or willingness to purchase,packaging, preparation and the extent to which these foods replaceother traditional complementary foods [2,3,13]. These issues havestrong implications for success and effectiveness of such programs[15] and are yet unexplored in different contexts in which fortifiedcomplementary foods are being introduced.
In the following pages we present findings from a qualitativestudy to understand community perception, acceptance and practicesassociated with a micronutrient fortified complementary food,distributed in the name of Balbhog.
Balbhog was introduced in 2007-08 by Government of Gujaratat scale after an initial pilot project supported by UN-World FoodProgramme (WFP) and Global Alliance for Improved Nutrition(GAIN). It was introduced as part of supplementary nutritionprogram under Integrated Child Development Services (ICDS) forchildren in the age group of 6- 36 months and delivered through anetwork of anganwadi centres (AWC) by anganwadi workers andhelpers. Balbhog is a specifically formulated pre-cooked, cerealbasedmicronutrient fortified food in powder form [16] made fromwheat, pulse flour, edible oil, sugar, defatted soybean and enrichedwith eleven essential macro and micronutrients (Table 1). Seven, fivehundred grams packets are provided per month to all under-threeyear children enrolled in AWC while ten packets are provided toseverely malnourished children. The product is expected to meet 33percent and 50 percent of energy and micronutrient requirementsrespectively of under-3 children.
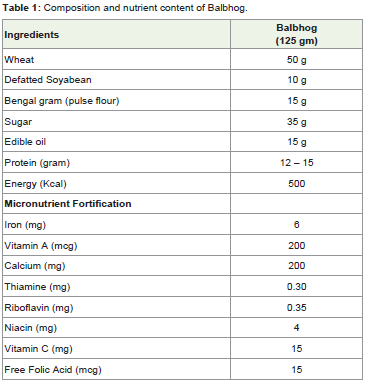
Table 1: Composition and nutrient content of Balbhog.
The government supports complementary feeding program bycelebrating Annaprashan day which encourages timely initiation,optimum feeding and monthly demonstration of preparation andfeeding of Balbhog to children in the age group of 6 to 9 months.The guideline recommends use of Balbhog but it does not emphasizeBalbhog as the only complementary food and encourages diversity incomplementary foods [17].
The objectives of the study were to (a) Understand perceptions of beneficiaries on Balbhog (b) Bring out associated practices pertainingto use of Balbhog and (c) Understand consumption pattern ofBalbhog.
Materials and Methods
Selection of participants
Four districts, Surat, Patan, Dahod and Jamnagar representingfour of the six regions of the state were randomly selected from districtsgrouped in to regions. From each district two rural and one urbanICDS projects were randomly identified and subsequently villageswere randomly selected from the district list of AWCs. Mothers of6-36 months aged children were purposively recruited. Participantsrepresenting different settlements as well as major caste and religiouscommunities including scheduled caste, scheduled tribe, and urbanpoor families. Non-users of Balbhog too were purposively identifiedand interviewed.
Data collection
In each district four focus group discussions (FGD) with usersand three in-depth interviews (IDI) with non-users of Balbhogwere conducted. Altogether 16 FGDs and 11 IDIs were conducted.Discussion guides and interview schedules for FGDs and IDIsrespectively were designed, piloted and the final version of the guideswere then translated in to the local language.
Data collection was done by a team of six Gujarati speakingresearchers with training in Food and Nutrition or Public Health. Atransect was used to identify an appropriate location that was relativelymore accessible to participants, spacious and neutral for conductingFGD. IDIs were conducted at participants’ home. Participants wereprovided with information on the study and an informed consent wastaken. The discussion guide was used but in a flexible manner. An interview guide was used for this purpose. Both FGDs and IDIs wereaudio recorded along with manual note taking.interview guide was used for this purpose. Both FGDs and IDIs wereaudio recorded along with manual note taking.
Analysis
The process of analysis began immediately after data collection.At the end of each FGD debriefing, reviewing and completion ofmanually written notes were done. Important aspects discussed inthe FGD, logistic and methodological problems faced, map and foodchartdrawn were discussed and noted. Further, after completingFGDs in one district the transcripts were heard to take forwardthe learnings to conduct FGDs in the subsequent districts. Audiorecordings were verbatim transcribed, corroborated with writtennotes, translated in to English and assigned in to Atlas-ti 6.2.28 foranalysis. ‘Framework analysis’ [18] approach was used for analysisof data. Two of the researchers who were involved in data collectiondid the analysis. After familiarisation of FGD/IDI data a thematicframework was identified. The background characteristics ofparticipants in different FGDs/IDIs too were considered for arrivingat meanings of data wherever possible and relevant.
Results
Knowledge and perceptions on Balbhog, its availability and benefits
a. Awareness about the product: A majority of the womenacross four districts were aware about Balbhog and were able toidentify, describe and differentiate Balbhog packets from otherfortified take home rations (THRs) such as sheera, upma and sukhadi13(SUS) in terms of appearance of packets, contents, colour, taste, andgranule size. Many members were also able to recall the compositionof Balbhog such as flour, pulse flour and sugar:
“Balbhog is written on top of it”, “… coffee colour lines and apicture is on top, a picture of mother and a daughter is there. “It iswritten on the packet that there is calcium”, “vitamins, iron”, “Bengalgram flour, sugar”
Some of the participants however could not differentiate Balbhogpackets from other THR packets externally. It is also possible that formany, there was no need to differentiate between Balbhog and otherTHR products as they received both kinds and the contents wereoften used interchangeably.
b. Availability and Distribution of Balbhog: Availabilityof Balbhog was a major factor that shaped the extent of utilisation.People did not have to make efforts to obtain these packets as AWWwould inform the eligible mothers about the arrival of supply whowould then collect it from the centre. In some cases women sharedthat if they miss collecting the packets from AWCs, then AWW orher helper would deliver the packets at their home. However, therewas no fixed day for distribution of Balbhog rather it depended on thearrival of supply at the AWC.
“If it comes today in balwadi (AWC) then immediately on next daythey come to call us”
“If we are the only ones remaining to collect Balbhog packets, thenshe comes and gives us”
There were however variations in number of packets received bywomen both within and between districts. The FGDs revealed thatwomen were not aware of the number of entitled packets and receivingthese packets was often seen as a gesture of benevolence from AWWrather than as their entitlement. As a result they expressed gratitudeeven if they were given only half the numbers of the entitled packets.It also appeared that distribution seemed to be partly arbitrary withquantum of packets distributed varying between one month and thenext depending on available stock and it also varied across familiesof similar entitlements. Some mothers pointed out that AWWsdistributed packets on the basis of nutritional status of children.
“Yes I get four packets”
‘If it is Balbhog they give 3 packets. If others have more childrenthen they give us (less) 2 packets and if someone has not taken thenthey will give (those packets to) us saying ‘take them as your child eats’ ”
“Sometimes they give on the basis of weight (of the child)”
“As our children are healthy and a few (others) are weak they tell usthat those children need more … hence we take one and come”
c. Perceived benefits of Balbhog: Participants reporteda number of benefits of Balbhog which could be grouped into fourthemes.
(i) Child eats well, gains weight, becomes healthy, and does notfall ill.
“Child’s appetite increases, even weight increases”. “… fever won’tcome”
“She was very thin. After starting Balbhog she became healthy”
“Weight will increase by Balbhog and not by Sitaram (locallyavailable fried snack)”
“No disease will linger”. “… and studies well”.
(ii) It has nutrients and is nourishing
“It is good, it is good for the children because iron and all comesfrom it”
“They get vitamin which forms blood. It is good if they eat thisinstead of outside food”
“Remains healthy, would receive sufficient nutrition”
(iii) Child likes hence easy to feed
The general perception among women is that if a child eatshappily without fuss then the product must be good and should begiven to the child.
“This they eat without difficulty. If something else we have to feedforcefully. But with this (Balbhog), if we give this in a bowl along withspoon (child) will eat on their own”.
(iv) Easy to prepare, saves time
Occasionally women also mentioned that Balbhog saves themthe daily trouble of deciding on what to prepare for lunch, dinner orsnacks. It was always an option. As everything is added into it, it iseasy to prepare.
The perceived benefits were also explored in the situation ofsupply of Balbhog being stopped. Many women expressed that if thesupply is stopped, it may affect child’s food intake; as the product hasmany healthy ingredients they will not be able to procure these forhome-made product.
“It will make difference, children eats this every day and if wechange what they eat daily then they will not eat”
Practices associated with use of Balbhog
The practices pertaining to Balbhog was studied under themes ofpreparation of food from Balbhog, additional ingredients used, ageof introduction of Balbhog, frequency of consumption and intrahouseholddistribution.
a. Preparation of food from Balbhog, including additionalingredients: Most women indicated that preparation of Balbhog wasnot a problem as it had all the necessary ingredients, came with clearinstructions on how to cook and could be easily prepared using onlyboiling water. However, a majority of the women had expressed thatBalbhog prepared in plain water does not come out well. Many hadexpressed that children preferred Balbhog when it is roasted in oil orghee (clarified butter), cooked in milk, and sugar or jaggery (molasses)additionally added. It improved taste, consistency and makes it softer.However it added extra cost to the family and therefore a few womenreported using only water.
“It does not come out good in plain water. Children don’t eat, don’tfind it tasty”
“If we roast in ghee and add milk or water then children eat”, “If weadd sugar then it becomes sweet and children eat”
“As it is less sweet we have to add sugar or something in it”
It was noted that most women treated Balbhog as a snack and notas the main meal. Feeding Balbhog during lunch was perceived tospoil the appetite of the child for the main meal. In other words thereis a lack of recognition of Balbhog as an ideal complementary food,which perhaps implied the need for enhanced nutritional counsellingby AWWs. Women prepare d different recipes from Balbhog asinstructed by AWWs and some experimented with traditional ornew recipes on their own. A common response was that children alsopreferred to eat Balbhog in the raw powder form. The raw powderbeing sweet and granular, by adding a bit of oil, dry balls of Balbhogcould also be instantly prepared and consumed.
b. Age of introduction of Balbhog: Many women reportedthat they initiated Balbhog after the child completed 6 months, asinstructed by the guideline. There were however many cases wheremothers initiated Balbhog much later.
“We started after 9 months”
“When he became one year old”
“I started when his teeth began to come out”
c. Frequency of consumption: Participants perceived thatBalbhog was being used in most households and only a few householdsin their area did not use it. There were instances narrated of migrant families requesting neighbours to collect their share of Balbhog foruse on their return.
“Two times we feed powder (Balbhog) and rest is homemade food”
“Mine asks daily, frequently he asks, as he likes its taste”
“Not daily, have to prepare alternate day, don’t eat daily”
“Prepare and give them whenever they feel like eating”
“Eats sometimes, don’t eat daily”
Once the Balbhog gets prepared it tends to get thick and stickyvery soon. To avoid wastage caregivers therefore prepared only theright amount that the child usually consumed or only after the childdemands for it.
d. Intra household distribution: Within the family, targeting theproduct to children of specific age group was a problem. The Balbhogwas often shared among all children and even among adult womenalthough it was rarely consumed by adult men. The women found itdifficult to prepare separate food for children and hence whenever aBalbhog preparation was made it was shared with all children in thefamily; likewise a child under the age of three was also fed with whatwas prepared for other grown up children in appropriate form.
“Older children eat, whoever in the family likes, eats”
“One is five years old, he also eats Balbhog”
“Men don’t eat only all ladies eat”
Perceptions and factors affecting non-usage
In-depth interviews were conducted with non-users of Balbhogto find their perceptions and factors that influenced their decisions.Further, even among the users reasons for irregular or infrequentuse were explored. While a few economically better off families hadexpressed that Balbhog is meant only for children of poor families,the latter had their own reasons for not using the product. In general,reasons adduced for low or non-use of Balbhog included poor state ofthe packets when it reached the beneficiaries, poor mouth-feel whenit was prepared in plain water, poor taste or undesired smell, childrefusing, or occasionally child having diarrhoea on consuming rawBalbhog, mother not knowing how to prepare it, not aware of thenutrient content of it and not having time to visit AWC to collect thepackets.
“Sometimes it does not come in good condition and somethingmight be in it and if we cook that and eat we may fall sick”
“Mine doesn’t eat and I also don’t prepare so we don’t take it”
“As there is medicine in it, there is smell she does not eat”
“She gets diarrhoea hence it is better not to feed”
“Don’t know, it was something to be prepared in water. As wewould not understand anything, left everything”
“As we have eaten homemade one, we don’t like all that, medicine and all is mixed in it”
“Why should (we) take and waste it when we don’t require? … Wedon’t bring we tell them that you give our packets to any poor person asmine does not eat … as they are poor and cannot afford to feed otherthings to their children hence if they prepare this and feed their childrenit will be good, they would not be getting fruits and all.”
Another important reason cited is that the local cuisine hada number of other food items prepared from rice, wheat, or othercoarse grains as the base with additional ingredients such as potatoes,grams, buttermilk and vegetables, given to children and that cannotbe replaced by Balbhog.
“She eats homemade one but does not eat the one prepared frompowder (Balbhog), eats dry powder only”
“Give milk, dal-rice, chapatti, vegetables boiled potatoes”
“Mine likes homemade one of semolina”
Discussion
The study has brought out community perceptions on theproduct, its availability and distribution, perceived benefits tochildren, practices associated with preparation, initiation, targeting,frequency of consumption, and factors leading to low or non-use ofthe product.
The women had a strong recall about the appearance of thepackage, colour and the product ingredients. Lack of appetite and thestruggle to feed children is one of the major factors for poor feedingpractices in children. The general perception among many caregiversis that if a child eats Balbhog happily then the product must be goodand should be given to the child.
Many caregivers attributed possible improvement in children’sappetite and weight gain to the acceptance of the product. Thepresence of vitamins and minerals in the product were also valuedby caregivers as they were related by them to healthy growth ofchildren. Apart from product features, ease in procuring andpreparation, children consuming without much fuss and thereforesaving caregivers’ time were other reasons given by participants foracceptance of Balbhog.
The result of the FGDs showed that Balbhog was being madeavailable but often not in stipulated quantity to all eligible families.The lack of awareness about the entitlement seems to be a majorbarrier and there is a need to make people aware of their entitlementand create demand on the ICDS system to deliver the recommendedpackets every month. Measures should be taken to reduce productdamage in transition and storage at AWC as poor packet qualityduring distribution affected uptake of the product. A perceptionamong selected sections that Balbhog is meant for poor was anotherfactor contributing to its non-usage among better off households.
Balbhog was being reportedly used by women but the frequencyof feeding differed across women ranging from daily to once ina week. The common practice was to feed children on demand.Similarly though many families initiated feeding of Balbhog by7thmonth, among many women this was delayed till 9thmonth or later. Targeting the under-three year children in households emerged as aproblem as Balbhog was often shared among other elder children andfamily members. As noted by an earlier study here too we find thatproviding fortified complementary food in conjunction with specificeducational messages rather than alone may be more beneficial.Family members have to be sensitized on the importance of feedingBalbhog fortified with micronutrients. It is important to emphasisethe right age to introduce Balbhog, regularity, frequency, appropriateconsistency and quantity of feeding Balbhog, hygienic way ofpreparing the product and the need to avoid excessive displacementof breast milk while feeding Balbhog. The role of micronutrients inphysical and mental growth and in prevention of anaemia in childrenneeds to be stressed during interaction with women [19].
Although Balbhog is projected as pre-cooked and ready to eatproduct it is largely not being perceived so by the community. Theresults of the study showed that preparation of Balbhog in plainwater did not come out well and hence caregivers had to improve itby adding additional ingredients like sugar, clarified butter, oil andmilk. This not only improved the palatability of the preparation andbrought it closer to the local cuisine in terms of taste and form butit also increased the energy density of the food. For many womenthis implies additional cost and they followed standard recipe ofpreparation with plain water. In other words, introducing smallvariations in preparations or increasing certain additions like oil andsugar in the pre-mix may further increase its acceptability as well as itseffectiveness in addressing malnutrition.This also points to potentialresearch possibilities of assessing the role of micronutrients vis-Ã -visthe energy rich additional ingredients in child’s growth. Studies haveshown that fortified milk-based or fat-based complementary foodsyield promising results [20,21].
Though the product has a wider acceptance it is being given notas the only but one of the complementary foods along with a numberof other homemade recipes. Balbhog was often seen as a snack givenbetween regular homemade meals and not replacing that latter.Availability of a range of homemade foods that are affordable andacceptable to children compels one to explore the option of homefortificationthat has been found to be acceptable in other contexts[15,22,13] as an alternative or additional strategy.There is a significantscope to improve supply related aspects. At the familial level there isample opportunity for nutrition counselling to improve initiation ofBalbhog at appropriate age, consistency, frequency and quantity offeeding, storage and focusing the feeding to targeted age groups toensure a higher energy density of complementary feeding.
Acknowledgements
The present study was part of larger study done in Gujarat funded by Global Alliance for Improved Nutrition (GAIN). The authorswould like to acknowledge support of Department of Women andChild Development, Government of Gujarat, and participants of thestudy and research associates who had helped in collecting data.
References
- Lutter CK, Rivera JA (2003) Nutritional Status of Infants and Young Children and Characteristics of Their Diets. J Nutr 133: 2941S-2949S.
- Faber M (2004) Complementary foods consumed by 6-12 month old rural infants in South Africa are inadequate in micronutrients. Public Health Nutr 8: 373-381.
- Lutter CK, Dewey KG (2003) Proposed Nutrient Composition for Fortified Complementary Foods. J Nutr 133: 3011S-3020S.
- National Nutrition Monitoring Bureau (2006) Diet and Nutritional Status of Population and Prevalence of Hypertension among Adults in Rural Areas. Hyderabad: National Institute of Nutrition.
- International Institute for Population Sciences & ORC Macro (2007) National Family Health Survey -3, 2005-06 India. Vol. I. Mumbai: IIPS.
- Lutter CK (2000) Processed complementary foods: summary of nutritional characteristics, methods of production and distribution, and costs. Food Nutr Bull21: 95-100.
- Rivera JA, Lutter CK (2001) The potential role of processed complementary foods in Latin America. In: Nutrition and Growth (eds. Martorell, R. &Haschke, F.) pp. 281-303. Nestle´ Nutrition Workshop Series Pediatric Program Volume 47, Lippincott Williams and Wilkins: Philadelphia, PA.
- Walter T, Dallman PR, Pizarro F, Velozo L, Pena G, et al. (1993) Effectiveness of iron-fortified infant cereal in prevention of iron deficiency anemia. Pediatrics 91: 976-982.
- Lartey A, Manu A, Brown KH, Peerson JM, Dewey KG (1999) A randomized, community-based trial of the effects of improved, centrally processed complementary foods on growth and micronutrient status of Ghanaian infants from 6 to 12 mo of age. Am J Clin Nutr 70: 391-404.
- Oelofse A, Van Raaij JM, Benade AJ, Dhansay MA, Tolboom JJ, et al. (2003) The effect of a micronutrient-fortified complementary food on micronutrient status, growth and development of 6 to 12 month old disadvantaged urban South African infants. Int J Food Sci Nutr 54: 399-407.
- Rivera JA, Sotres-Alvarez D, Habicht JP, Shamah T, Villalpando S (2004) Impact of the Mexican programme for education, health and nutrition (PROGRESA) on rates of growth and anemia in infants and young children: a randomized effectiveness study. JAMA 291: 2563-2570.
- Lutter CK, Rodriguez A, Fuenmayor G, Avila L, Sempertegui F, et al. (2008) Growth and Micronutrient Status in Children Receiving a Fortified Complementary Food. J Nutr 138: 379-388.
- Adu-Afarwuah S, Lartey A, Brown KH, Zlotkin S, Briend A, et al. (2008) Home fortification of complementary foods with micronutrient supplements is well accepted and has positive effects on infant iron status in Ghana. Am J Clin Nutr 87: 929-938.
- Eichler K, Wieser S, Ruthemann I, Brugger U (2012) Effects of micronutrient fortified milk and cereal food for infants and children: a systematic review. BMC Public Health 12(506).
- Jefferds ME, Ogange L, Owuor M, Cruz K, Person B, et al. (2010) Formative research exploring acceptability, utilization, and promotion in order to develop a micronutrient powder (Sprinkles) intervention among Luo families in western Kenya. Food Nutr Bull 31: S179-S185.
- Global Alliance for Improved Nutrition (2009) Combating Malnutrition ...Our mission.
- Gujarat, Government of (2010) Annaprashan Day: Introduction of complementary foods in the infant's feeding schedule - Guide Book. Integrated Child Development Services, Women and Child Development Department, Government of Gujarat.
- Ritchie J, Spencer E (1994) Qualitative data analysis for applied policy research. In Analyzing Qualitative Data. [A Bryman and RG Burgess, editors]. London: Routledge. Ritchie J, Spencer L. Qualitative data analysis for applied policy research. In: Bryman A, Burgess R, editors. Analysing qualitative data. London: Routledge; 1993. pp. 173-194.
- Dewey KG, Adu-Afarwuah S (2008) Systematic review of the efficacy and effectiveness of complementary feeding interventions in developing countries. Matern Child Nutr 4: 24-85.
- Sazawal S, Dhingra U, Dhingra P, Hiremath G, Kumar J, et al. (2007) Effects of fortified milk on morbidity in young children in north India: community based, randomised, double masked placebo controlled trial. BMJ: 334- 140.
- Adu-Afarwuah S, Lartey A, Brown KH, Zlotkin S, Briend A, et al. (2007) Randomized comparison of 3 types of micronutrient supplements for home fortification of complementary foods in Ghana: effects on growth and motor development. Am J Clin Nutr 86: 412-420.
- Zlotkin SH, Schauer C, Agyei SO, Wolfson J, Tondeur MC, et al. (2006) Demonstrating zinc and iron bioavailability fromintrinsically labeled microencapsulated ferrous fumarateand zinc gluconate sprinkles in young children. J Nutr 136: 920-925.