Research Article
Comparative Analysis and Relationship between Nutritional Status and Physical Efficiency among the Rural and Urban Children
Arora D1, Das A2 and Mahata H3*
1Department of Physiology, Shri Shankaracharya Institute of Medical Sciences, Bhilai, India
2Department of Physiology, Vidyasagar College for Women, Kolkata, India
3Department of Physiology, Midnapore College (Autonomous), Midnapore, West Bengal, India
2Department of Physiology, Vidyasagar College for Women, Kolkata, India
3Department of Physiology, Midnapore College (Autonomous), Midnapore, West Bengal, India
*Corresponding author:Hiranmoy Mahata, Department of Physiology, Midnapore College (Autonomous), Midnapore, West Bengal, India. Email Id: hiranmoymahata27@gmail.com
Article Information:Submission: 12/12/2024; Accepted: 02/01/2025; Published: 04/01/2025
Copyright: ©2025 Arora D, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction:In developing countries like India, the children, irrespective of their community or societal background, do not have a proper or normal growth rate. The growth of a child mainly depends upon the nutritional status. Physical efficiency can easily be determined by the individual capacity for maximal energy output, muscular strength, coordination and movement.
Aim:The primary goal of this research was to assess whether any association between nutritional status and physical efficiency of rural and urban children exists. One Hundred twenty children were chosen at random from Medinipur districts (Purba and Paschim) of West Bengal for this study.
Methodology:All the children (6-9 yrs) were measured for various physical fitness components and nutritional status which was evaluated using different nutritional indices and 24-Hrs recall method. The motor function of the children was measured with the help of reaction time measurement (stick drop test). Modified push-up test was used to evaluate the endurance of the children. Sit and reach test was then used to assess the flexibility among the children.
Results:The results revealed that the rural children have significantly higher endurance (p<0.001) in push up and flexibility (p<0.001), than the urban children. But the urban children showed a significantly (p<0.05) better reaction time than the rural children. The correlation between protein intake and reaction time (p<0.05) and push-up test was significant in case of rural children. Other nutritional parameters are not significantly correlated with physical fitness.
Conclusion:The study found that children in rural areas were more physically fit than in urban areas. These findings demonstrate the impact of living environment has the ability to prop-up an active lifestyle that improves physical fitness. Rural children were more engaged in both scheduled and unstructured (tree climbing, cycling, swimming and helping in household chores and agricultural activities) physical activities which may be overall emphasizing their physical fitness.
Aim:The primary goal of this research was to assess whether any association between nutritional status and physical efficiency of rural and urban children exists. One Hundred twenty children were chosen at random from Medinipur districts (Purba and Paschim) of West Bengal for this study.
Methodology:All the children (6-9 yrs) were measured for various physical fitness components and nutritional status which was evaluated using different nutritional indices and 24-Hrs recall method. The motor function of the children was measured with the help of reaction time measurement (stick drop test). Modified push-up test was used to evaluate the endurance of the children. Sit and reach test was then used to assess the flexibility among the children.
Results:The results revealed that the rural children have significantly higher endurance (p<0.001) in push up and flexibility (p<0.001), than the urban children. But the urban children showed a significantly (p<0.05) better reaction time than the rural children. The correlation between protein intake and reaction time (p<0.05) and push-up test was significant in case of rural children. Other nutritional parameters are not significantly correlated with physical fitness.
Conclusion:The study found that children in rural areas were more physically fit than in urban areas. These findings demonstrate the impact of living environment has the ability to prop-up an active lifestyle that improves physical fitness. Rural children were more engaged in both scheduled and unstructured (tree climbing, cycling, swimming and helping in household chores and agricultural activities) physical activities which may be overall emphasizing their physical fitness.
Keywords:Children; Rural-Urban; Nutrition; Physical Activity; BMI; Endurance; Flexibility; Reaction Time; Sit and Reach Test; Push-Up Test
Introduction
Nutritional status and physical efficiency are critical determinants
and fundamental pillars of a child’s health, which directly or indirectly
influence their growth, cognitive development, and long-term wellbeing
that ultimately affect their overall growth, development, and
potential for a healthy adulthood. However, disparities in these
essential health indicators persist between rural and urban areas,
reflecting broader socio-economic and environmental inequalities.
While urbanization has brought improved access to healthcare
and nutrition services for some, rural communities continue to
face unique challenges, including limited resources, inadequate
infrastructure, and cultural barriers. Rural children often face
heightened vulnerability to malnutrition, stunting, and reduced
physical fitness.
The nutritional status of children is a critical determinant of their
physical and cognitive development, with long-term implications for
health and wellbeing. Adequate nutrition is essential for the growth,
development, and maintenance of optimal health, while nutritional
deficiencies can lead to impaired growth, increased susceptibility to
infections, and reduced cognitive function.
Physical efficiency, encompassing cardiovascular endurance,
muscular strength, and flexibility, is equally important for child
health outcomes. Regular physical activity has been shown to improve
cardiovascular health, reduce the risk of obesity and chronic diseases,
and enhance mental wellbeing. Physical fitness is an important
measure of a child’s (or adolescent’s) health and a reliable indication
of health in their adulthood [1]. Throughout human history,
maintaining physical fitness has been considered a crucial component
of daily living. For the most part, the people of ancient times relied
on their own strength and energy to survive [2]. It involved being
proficient in several core abilities, including strength, endurance,
speed and agility for running, jumping, and climbing, among other
abilities needed to get their livelihood. Urbanization has led to a shift
towards more sedentary lifestyles, characterized by reduced physical
activity and increased reliance on processed foods. In contrast, rural
areas often face challenges related to food insecurity and limited
access to nutrient-dense foods, reduced access to healthcare services,
health education and higher rates of poverty and socioeconomic
disadvantage.
In India, there is an immense financial gap between rural and
urban regions. The majority of Indians (about 70%) live in villages. In
India, there are notable distinctions between rural and urban areas.
The disparity in people’s living standards between rural and urban
locations is one of the most significant distinctions that can be very
well observed. Many individuals prefer to live in rural areas because
of its peaceful atmosphere. Compared to metropolitan regions, rural
places are not so fast-paced, polluted, or highly inhabited. Rural places
are less crowded, less dirty, and slower moving. The atmosphere is
cleaner and fresher in rural places [3]. But still, people living in urban
areas enjoy a better standard of living due to their economic status
[4].
The present comparative analysis aims to investigate the rural urban
disparities in nutritional status and its effect on physical
efficiency among children, exploring the complex interplay of factors
contributing to these differences and informing targeted interventions
to bridge the gap and ensure equitable health outcomes for all leading
to development of targeted interventions and public health strategies.
Material and Methods
Selection of study area and subjects:
The study consists a total of 120 subjects who were children
(aged 6 to 9) and picked randomly from various villages (rural) and
town (urban) of both Medinipur districts (Purba and Paschim) of
the Indian state of West Bengal. Sixty children from rural and sixty
children from urban area were selected randomly, irrespective of
their gender.Inclusion criteria
Aged between 6-9 years
Both genders
Standard growth with ideal health
Capable of understanding basic instructions
Aged between 6-9 years
Both genders
Standard growth with ideal health
Capable of understanding basic instructions
Exclusion criteria
The study excluded children with known endocrine disorders, respiratory illnesses, musculoskeletal disorders, and neurological disorders
Children who do not cooperate or understand the instructions
Any type of nerve damage in the upper limb, including an open wound, recent fracture, contracture, or other injury
Any other condition that prevents the children from performing the tests
The study excluded children with known endocrine disorders, respiratory illnesses, musculoskeletal disorders, and neurological disorders
Children who do not cooperate or understand the instructions
Any type of nerve damage in the upper limb, including an open wound, recent fracture, contracture, or other injury
Any other condition that prevents the children from performing the tests
Ethical Consideration:
Prior to commencing the study, the mandatory nature and
objectives of the research were thoroughly explained to the
children, ensuring their comprehensive understanding. To maintain
confidentiality and protect the participants’ identities, their names
and personal information were kept strictly private throughout the
research process.Anthropometric Measurements:
Height (in cm.):Before measuring the vertical distance from the
floor to the subject’s highest point (vertex), or largest bulging section
of the head, the subject was first instructed to stand straight on a flat
surface barefoot. An anthropometric rod was used to measure height
with an accuracy of 0.1 cm. By averaging three measurements, the
final measurement was calculated.Weight (in Kg.):A portable flour-type weighing machine (Libra)
was used to determine the weight of subjects. Children were asked to
stand straight on the weighing machine in minimum clothing and
reading was taken from the scale of the machine with an accuracy of
0.1 Kg.
Nutritional Assessment:
Body Mass Index (in Kg. / m2): The Body Mass Index (BMI)
indicates the degree of adiposity of body weight to characterize
variation in body composition. From the measured height and weight
of the subjects, the BMI was computed using the following standard
equation [5,6]
BMI = weight (kg.)/height2 (m)Head Circumference (in cm.):A measuring tape was used
to measure the maximum circumference of the head above the
attachment of the ears. The tape was placed slightly above the ridges
of the eyebrows and wrapped around the back of the head [7].
Mid Upper Arm Circumference (MUAC) (in cm.): When the
arm is relaxed, the maximum circumference of the right arm at
the biceps was measured using a non-stretchable tape positioned
perpendicular to the upper arm’s long axis [8,9]. The figure is upright,
facing forward, with relaxed upper limbs and shoulders and hands
toward the sides [7].
Diet Survey (24Hrs. recall method):
The dietary survey of 24-hour recall method consists of a detailed
interview in which the food intake from the previous day is reported.
The 24-hour recall method is commonly used in dietary surveys and
research due to its low burden on respondents, as it does not require
literacy and allows for customization based on the individual’s food
knowledge. It was noticed how the subjects estimated portion sizes
using food models or photos, or how much each meal weighed on
average. The approach depends on the subject’s recollection. The
percentage of calories, protein, fat, and carbohydrate was then
computed from the collected data [10].Study of Physical Efficiency:
Reaction Time (in sec.) by Ruler Drop Test: Reaction time (RT)
is measured using the ruler drop method [11]. A flat, horizontal table
surface was used, and the subject was instructed to sit with their
dominant side elbow bent to a 90-degree angle, their mid-pronated
forearm resting on it, and their dominant hand open at the edge of the
surface. According to Aranha and his coworkers [11], the examiner
positioned the ruler vertically such that the lower end would line up
with the web space, or five centimetres, between the child’s thumb and
index finger. The thumb and index fingertips were then positioned
horizontally. The child was instructed to grab the ruler as soon as it
was freed from the examiner’s hold. The participant was instructed
to aim at the falling stick rather than the tester’s hand or not to raise
or lower your hand to try to grab the falling stick. Before each drop,
there was a ready or preliminary command. Children were required
to see a demonstration of the test procedure and take part in two
practice runs in order to become accustomed to it [12].Score: Twelve trials were taken, the slowest three and the fastest
three readings were rejected and the middle six were recorded as the
scores. Then mean of these six scores were used for the analysis.
The distance the ruler travelled from starting 5 cm was recorded.
Then this distance was converted into time by using the following
formula: T = 2d /g, where ‘d’ was the distance traveled by the ruler
and ‘g’ was the gravitational constant (9.8 m/s).
Endurance Test by Modified Push-Up test:
The performer lowers their body towards the floor until their
chest reaches it while keeping their knees bent and lying on the
ground and their hands precisely beneath their shoulders. They were
then instructed to push themselves back to the beginning position.
Throughout the trial, it is imperative that the body must remain in
a straight line from the knees to the hips to the shoulders, without
sagging [13,14]. The arms remained extended, shoulder-width apart,
and perpendicular or straight angle to the body. The subject was
asked to maintain this posture while lowering their upper body to
allow their elbows to bend to a 90-degree angle [15]. The subject was
instructed to do as many repetitions as possible without rest [15].Score: The score was the number of correct modified push-ups
continuously executed by the subject without any rest. Scoring was
terminated if performed stopped to rest. If the chest does not touch
the mat or if the arms are not extended on an execution, the trial is
not been counted.
Flexibility Test by Sit and Reach Test:
The sit and reach test was selected to assess flexibility because
it is a widely used method for evaluating flexibility in children and
teenagers [16,17]. The subjects were instructed to take off their
shoes. Next, they were asked to take a seat on the floor with both legs
extended straight in front so the soles were pressed flat on the box
and both the knees were kept locked and pressed flat against the floor.
A helper could support the knees downward. The palm was kept
pointing downwards. Hands were positioned side by side or on top
of one another.The person whose flexibility was to be assessed tries to reach as
far forward as possible with both hands along the box’s measuring
scale [18,19].
Statistical Analysis:
For the representation of data, percentages and frequencies were
used for categorical data; for continuous variables, mean and standard
deviation were used while for categorical variables, the Chi-square
test. The statistical software IBP SPSS (version 2.0) and Microsoft
Office Excel (2019) were used for all statistical analysis.Results
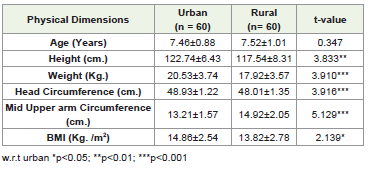
Anthropometric dimensions of urban and rural children are
given in [Table 1]. Urban children showed significantly higher values
for height (p<0.01), weight (p<0.001), head circumference (p<0.001),
and BMI (p<0.05) in comparison to rural children. However, rural
children had significantly greater (p<0.001) MUAC than the urban
children.
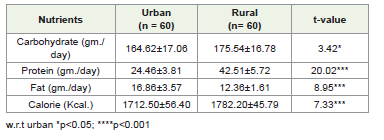
In rural children, carbohydrate, protein, and calorie intake were
significantly higher (p<0.001) than the urban children [Table 2]. But,
fat intake in urban children is significantly higher (p<0.001) than the
rural children.
[Table 3] represents the physical efficiency of rural and urban
children. In modified push-up and flexibility test, the rural children
performed significantly better (p<0.001) than the urban children.
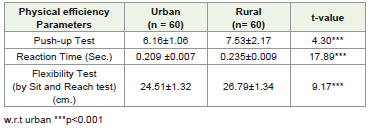
But in reaction time test, urban children had significantly better
performance than rural children.
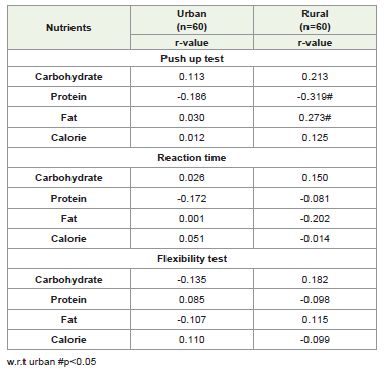
The fitness parameters were assessed for their association with
nutrient and calorie intake. The current study observed [Table 4] that
there was no significant correlation between any physical efficiency
parameter and the consumption of calories, proteins, fats, and
carbohydrates in both rural and urban children. In the case of rural
children, perhaps there was very little association between the pushup
test and the consumption of protein.
Discussion
Machado-Rodrigues and his team [20] reported that in urban
children, increased height, weight, and BMI were caused by their
sedentary lives, access to a more diverse diet, and processed foods.
Rao and his team [21] highlighted that limited healthcare and lower quality
diets contribute to lower height and weight among rural
children compared to their urban counterparts, where healthcare is
more accessible, resulting in better overall growth indicators. Mai and
his colleagues [22] studied that urban child benefit from higher family
income and parental education, leading to better nutritional intake,
which supports growth in height and weight compared to rural areas.
Ramana and his coworkers [23] found that urban children were
more likely to be overweight or obese due to sedentary behaviors and
reduced physical activity. This contributes to higher BMI than rural
children, who often engage in more outdoor and physical activities
[24].
Barman’s team (2024) observed that rural children had higher
MUAC compared to urban children, with rural children engaging
in more physical labor and outdoor activities that support muscular
development. Urban children, on the other hand, were found
to be more sedentary, which can result in higher fat stores but
lower muscle mass, reflected in MUAC [26]. Ramanujam and his
colleagues [27] conducted a study that also found that rural children
had higher MUAC than their urban counterparts. This was largely
attributed to the fact that rural children had more physically active
lifestyle and diets consisting of protein-rich pulses and dairy (such
as lentils and locally available milk products), contributing to greater
muscle development. The researchers [28] attributed this to regular
consumption of nutrient-dense foods such as pulses, legumes, and
locally sourced vegetables, which may support muscle development
in rural children. Studies [29,30] also suggest that higher physical
activity levels and traditional diets (rich in pulses, grains, and local
vegetables) may contribute to higher lean body mass, reflected in
higher MUAC values in rural children.
Khed and Saravanakumar [31] found that rural children had
higher intake of carbohydrates and calories compared to urban
children. Rural diets emphasized staples like rice and chapati with
added protein from lentils and pulses. The researchers noted that rural
families often eat meals based on traditional foods that are high in
both carbohydrates and protein to meet the high energy demands of
rural lifestyles. Nabdi’s team [32] noted that rural children consumed
higher amounts of carbohydrates and overall calories, primarily
from staple foods like wheat and millet. This was attributed to the
agricultural lifestyle in rural areas, where energy-dense foods are
prioritized to support physically demanding tasks, both for children
and adults.
Arya and Dubey [33] highlighted those urban children in India
consume higher levels of dietary fat due to the increased consumption
of fast food, snacks, and processed foods, which are more accessible
in urban areas. Studies suggest that urban children are more exposed
to calorie-dense and high-fat foods than rural children, who consume
more traditional, lower-fat diets [34]. The increased availability of
processed foods and fast foods rich in saturated fats in urban areas
contributes significantly to higher fat consumption among urban
children [35].
Researchers [36,37] pointed that involvement of rural children
in activities like carrying water, working on farms, and walking long
distances was cited as a primary factor contributing to their increased
upper body strength and muscular endurance in comparison to their
urban counterparts. Raghav [38] and Kumari [39] stated that rural
children’s higher physical activity levels were identified as a major
factor, whereas urban children’s sedentary lifestyle (due to screen
time and indoor activities) was linked to lower muscular strength and
endurance [39].
Emerging research [40,41] indicates that rural children’s higher
level of physical activity, including unstructured outdoor play
and chores that require frequent bending, lifting, and stretching
which often involve movements that enhance flexibility, which
are commonly part of rural daily routines. The authors [42,43]
highlighted that urban child spend more time on sedentary activities,
such as using digital devices and watching television.
Reigal and his research team [44] pointed that urban children’s
participation in organized sports and games that improve reaction
time, such as badminton and tennis, was a significant contributing
factor to the improvement of hand-eye coordination, neuromotor
skills and reflexes [45]. But such activities are less common in
rural areas. Researchers [46] attributed this to lifestyle differences,
suggesting that urban children are more likely to engage in activities
requiring fast responses, such as video games and interactive sports
and digital tools, which are more accessible in urban settings in
comparison to rural area [47].
High protein intake might lead to a reduction in carbohydrate
consumption. Carbohydrates are the primary source of energy for
high-intensity, short-duration activities like push-ups [48,49]. A
lack of sufficient carbohydrates could impair performance despite
high protein consumption. Carbone and Pasiakos [50] stated that
dietary protein is essential for muscle repair and growth, it does not
directly enhance physical performance without a well-balanced diet.
Adequate carbohydrate intake is necessary to provide energy during
exercise.
Conclusion
Hence, from the present study, it may be concluded that
children in rural areas tend to be more physically fit than in urban
areas. This may be due to the direct impact of their living standard
and environment, which contributed to their active lifestyle that
ultimately improves physical fitness. Rural children were more
engaged in both scheduled and unstructured physical activities which
may be overall emphasizing their physical fitness. But their reaction
time might be due to a slower reflex as they do not spend more time
in online or playing video games which somehow contributed to the
faster reaction time seen in urban children.
Acknowledgment
We would like to express our deepest gratitude to the children
who participated in the present study and all the other stakeholders.
References
Citation
Arora D, Das A, Mahata H. Comparative Analysis and Relationship between Nutritional Status and Physical Efficiency among the Rural and Urban Children. Indian J Nutri. 2025;12(1): 305.