Research Article
A Systematic Review on the Burden of Nonnutritional Causes of Anemia among Pregnant Women in India
Khanam A1, Ranjith A2, Vohra K1, Sharma T2, and Yadav K2*
National Centre of Excellence and Advanced Research on Anemia Control (NCEAR-A) Centre for Community Medicine (CCM) All India Institute of Medical Sciences (AIIMS) New Delhi, India
Centre for Community Medicine (CCM) All India Institute of Medical Sciences (AIIMS) New Delhi, India
Centre for Community Medicine (CCM) All India Institute of Medical Sciences (AIIMS) New Delhi, India
*Corresponding author:Kapil Yadav, Centre for Community Medicine (CCM) All India Institute of Medical Sciences (AIIMS) New Delhi, India.E-mail Id: dr.kapilyadav@gmail.com
Article Information:Submission: 09/10/2024; Accepted: 07/11/2024; Published: 11/11/2024
Copyright: © 2024 Khanam A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction:Anemia is significant public health problem of multifactorial causation. Nutritional causes such as iron, folate, vitamin B12, vitamin A deficiencies, and protein-energy malnutrition can result in anemia. The non-nutritional causes of anemia include genetic disorders such as hemoglobinopathies, infectious diseases, and various other chronic diseases. Non-nutritional causes of anemia constitute a significant burden in world and also in India. This review aimed to study the burden of different non-nutritional causes of anemia among pregnant women in India.
Methods:PubMed and Google Scholar were searched for studies reporting on the prevalence of non-nutritional causes of anemia among pregnant women in India, published from 2012 to 2024. The systematic review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Result:A total of 297 studies were identified, of which 27studies were included in the systematic review. The prevalence of beta-thalassemia disease was 2.1%, beta-thalassemia trait ranged from 0.7 to 8.5%, sickle cell disease from 0.7 to 1.6%, and sickle cell trait from 0.2 to 15.6% amongst pregnant women. The prevalence of malaria was in the range of 0.8 to 29.3%, among pregnant women in India.
Conclusion:Non- nutritional causes of anemia constitute a significant burden amongst pregnant women in India. Non-nutritional causes of anemia need to be addressed to achieve targets of control of anemia. There is a need for more scientifically sound basic research investigating the prevalence of different non-nutritional causes of anemia in pregnancy.
Methods:PubMed and Google Scholar were searched for studies reporting on the prevalence of non-nutritional causes of anemia among pregnant women in India, published from 2012 to 2024. The systematic review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Result:A total of 297 studies were identified, of which 27studies were included in the systematic review. The prevalence of beta-thalassemia disease was 2.1%, beta-thalassemia trait ranged from 0.7 to 8.5%, sickle cell disease from 0.7 to 1.6%, and sickle cell trait from 0.2 to 15.6% amongst pregnant women. The prevalence of malaria was in the range of 0.8 to 29.3%, among pregnant women in India.
Conclusion:Non- nutritional causes of anemia constitute a significant burden amongst pregnant women in India. Non-nutritional causes of anemia need to be addressed to achieve targets of control of anemia. There is a need for more scientifically sound basic research investigating the prevalence of different non-nutritional causes of anemia in pregnancy.
Keywords:Anemia Burden; Hemoglobinopathies; Thalassemia; Sickle Cell Disease; Pregnant Women; India
Introduction
Anemia is one of the most important public health problems
in many developed and as well as developing countries, including
India. Anemia in pregnancy is associated with maternal and
fetal complications such as low birth weight, preterm delivery,
impaired neurological development of the child, maternal
mortality, and morbidity.[1] The World Health Organization
(WHO) defines anemia in pregnancy as a condition in which
the haemoglobin concentration in the blood falls below 11 g/
dl. It results in reduced oxygen-carrying capacity of the blood
and the inability to fulfil the physiological needs of the individual.
[2] WHO estimates the prevalence of anemia among pregnant
women is 41.8% globally. [3] The National Family Health Survey
(NFHS-5) 2019 – 2021 in India estimated the prevalence of
anemia among pregnant women to be 52.2%. [4]
The causes of anemia are multifactorial and include both
nutritional and non-nutritional causes. Nutritional causes such
as iron, folate, vitamin B12, vitamin A deficiencies, and protein-
energy malnutrition can result in anemia, as these nutrients
are needed for the synthesis of hemoglobin in the body. Iron
deficiency is known to be the most common cause of nutritional
anemia during pregnancy. The non-nutritional causes of
anemia include genetic disorders such as hemoglobinopathies
(thalassemia, sickle cell disease) and hemophilia, infectious
diseases (malaria, tuberculosis, soil-transmitted helminths), and
various other chronic diseases.[5]
Hemoglobinopathies including thalassemia and sickle cell
disease (SCD) are the most common single-gene disorders
(autosomal recessive)and constitute a significant health problem
in certain parts of the world, including India.[6] Thalassemia
is a blood disorder characterized by inherent defects in the
synthesis of globin chains of the hemoglobin. This impairs
normal hemoglobin synthesis, thereby affecting the production
of red blood cells (RBCs), resulting in anemia. Communities like
Sindhis, Punjabis, Gujaratis, Bengalis, Mahars, Kolis, Saraswats,
Lohanas, and Gaurs have shown higher frequencies of carrier
state of beta-thalassemia. [7] SCD is a genetic blood disorder
in which an abnormal hemoglobin S is produced, making RBCs
more susceptible to destruction in the small blood vessels. This
increased destruction of RBCs is implicated in the pathogenesis
of anemia associated with SCD. SCD is known to be prevalent
in certain tribal communities of southern, eastern, and western
states of India.[8]
Infectious diseases particularly malaria and tuberculosis, and
soil-transmitted helminth infestations have been recognized as
important health problems in tropical and sub-tropical regions
of India. The malarial parasite multiplies inside the human RBCs,
leading to their destruction, causing anemia.15 Studies have
reported a strong association between tuberculosis and anemia,
but the direction of this relationship and the exact mechanism
are not known.[9] Soil-transmitted helminth infestations lead
to severe anemia through intestinal blood loss and by causing
deficiencies of various micronutrients.[10] Chronic diseases are
associated with inflammation resulting from infectious causes,
metabolic causes, autoimmunity and other causes. Inflammation
results in cytokine-mediated increase in hepcidin levels in the
body. Hepcidin is a protein molecule that inhibits intestinal
absorption of iron and it is released primarily by the liver.[11]
For developing strategies to control the non-nutritional
causes of anemia in pregnancy, we need to estimate the magnitude
of the problem posed by them. There have been limited studies
conducted in India to assess the prevalence of non-nutritional
causes of anemia among pregnant women. Also, there are no
previous systematic reviews addressing this question. Therefore,
this review aimed to estimate the burden of different non nutritional
causes of anemia among pregnant women in India.
Methodology
Search strategy: This systematic review was reported
according to the Preferred Reporting Items for Systematic
Reviews and Meta-Analyses (PRISMA) guidelines. PubMed and
Google Scholar were searched for relevant published articles.
The following keywords were used for the literature search
– prevalence Anon-nutritional causes of anemia, pregnancy,
prevalence of infectious diseases (Malaria, Tuberculosis and
helminths), hemoglobinopathies, chronic diseases (Liver and
kidney) and all combination of these words. All relevant studies
published from 2012 to 2024 were identified during the search
process. To increase the width of the search, the list of references
of all relevant studies found in the above search was also
screened.
Eligibility Criteria:
Inclusion criteria: This systematic review included
all observational studies conducted in India that assessed
the prevalence of non-nutritional causes of anemia such as
hemoglobinopathies (beta-thalassemia disease, thalassemia
trait, sickle cell disease, and sickle cell trait),hemophilia,
infectious diseases (malaria,tuberculosis, soil-transmitted
helminths),chronic liver disease, and chronic kidney disease,
which were published in different peer-reviewed journals during
the last 10 years from 1st January 2012 to 30thJanuary 2022.
The search was run again on 31st August 2024 to include all
available evidence. Only studies published in English language
were included. There were no restrictions specified for the study
setting, study duration, and outcome assessment technique.Exclusion criteria: Studies without full text, commentaries,
duplicated studies, anonymous reports, and irrelevant data were
excluded.
Search Methods: Two reviewers independently searched
PubMed and Google Scholar using the keywords such. After
removing the duplicates, the identified studies were first screened
by title and abstract. Those studies found relevant on title and
abstract screening were considered for full-text evaluation by
applying the inclusion and exclusion criteria. The screening
was done by two independent reviewers, and any disagreement
between them was resolved through discussion with help from a
third reviewer.
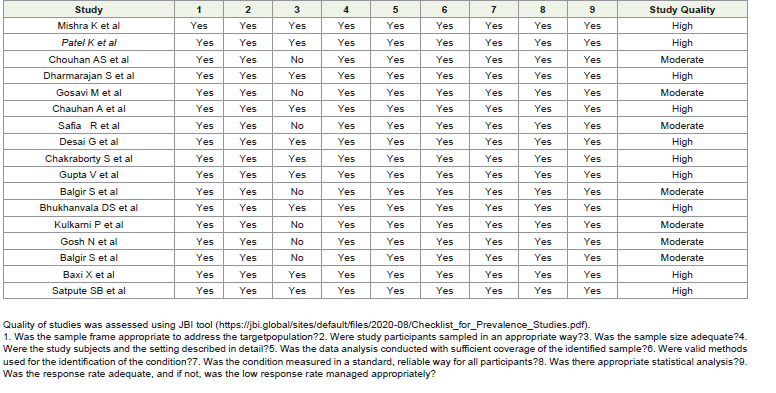
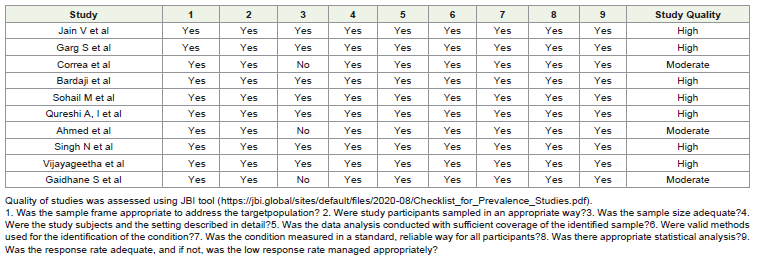
Study quality assessment: The quality of the included
studies was assessed using JBI tool (https://jbi.global/sites/
default/files/2020-08/Checklist_for_Prevalence_Studies.pdf).
Quality assessment of the studies was done by two independent
reviewers with disagreements resolved through discussion.
Data extraction: Data from the studies considered for
inclusion in the review were extracted onto Microsoft excel.
The following data were extracted –author’s name, publication
year, study design, study area/setting, study period, sample
size, age distribution of the participants, presence and severity
of anemia, prevalence of non-nutritional causes of anemia such
as hemoglobinopathies (thalassemia, sickle cell disease) and
hemophilia, infectious disease (malaria, tuberculosis, helminths)
chronic liver disease, and chronic kidney disease among the
study participants. Data extraction was done by two independent
reviewers, with disagreements resolved through consensus.
Results
Selection of the studies:
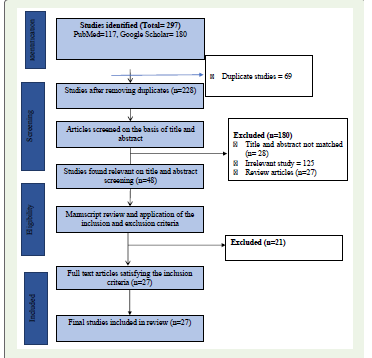
A total of 297 studies were identified by a literature search on
two databases. Out of all the studies identified 69 were duplicates.
After the removal of the duplicates 228 studies were subjected
to title and abstract screening, during which 180 studies were
excluded because they were found irrelevant. Forty-eight studies
were assessed for eligibility by full-text evaluation by applying
the inclusion and exclusion criteria. Twenty-one studies were
found ineligible and the remaining 27 studies were included in
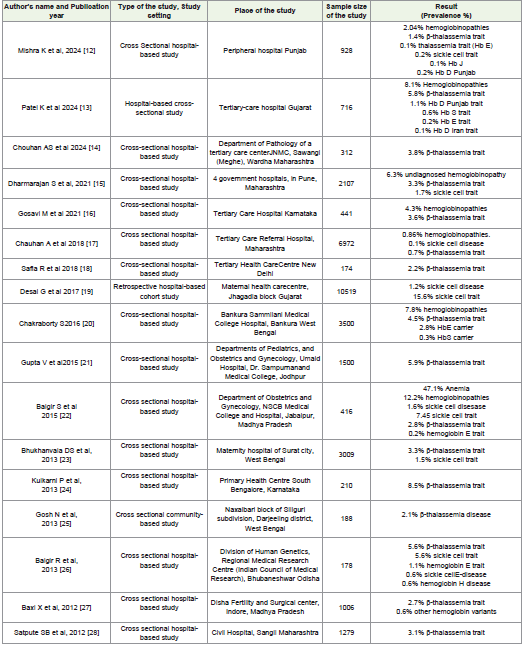
the current review. [Figure 1].Characteristics of the included studies:
A out of twenty-seven studies were included in the review. Six
were community-based studies, and the twenty-one remaining
studies were hospital-based. A total of seventeen studies
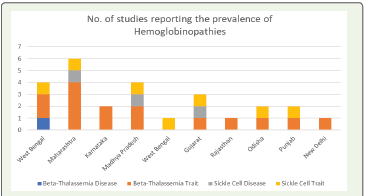
reported the prevalence of hemoglobinopathies [Table 1]. Only
one study conducted in West Bengal reported the prevalence
of beta-thalassemia disease. Fifteen studies reported the
prevalence of beta-thalassemia trait, four studies were conducted
in Maharashtra, and two each conducted in Karnataka, Madhya
Pradesh, West Bengal, and one each in Gujarat, Rajasthan, Odisha,
Punjab and New Delhi. Three studies reported the prevalence
of sickle cell disease, one each was conducted in Maharashtra,
Madhya Pradesh, Gujarat. Six studies, one each conducted in West
Bengal, Odisha, Maharashtra, Punjab, Madhya Pradesh, Gujarat
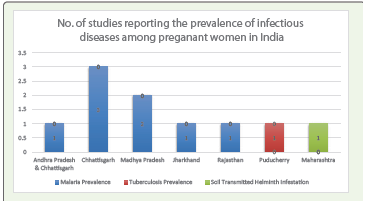
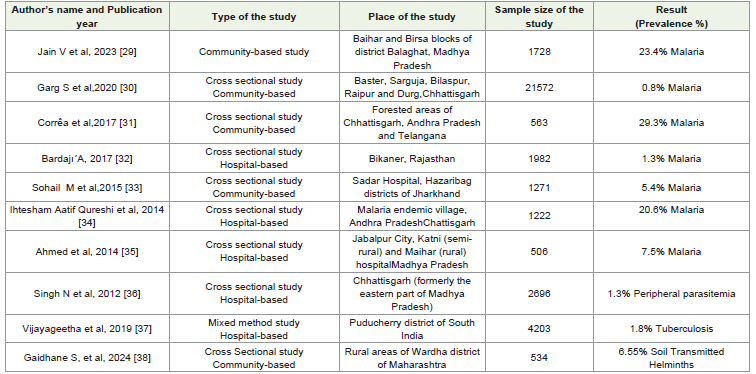
reported the prevalence of sickle cell trait. Ten studies reported
the prevalence of infectious diseases among pregnant women.
Eight studies reported malaria prevalence, of them one study
was conducted in two states – Andhra Pradesh and Chhattisgarh,
three studies were from Chhattisgarh, two studies were from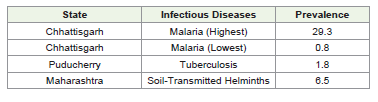
Madhya Prades hand one each from Jharkhand and Rajasthan.
One study from Puducherry reported tuberculosis prevalence
among pregnant women. One study conducted in Maharashtra
reported the prevalence of soil transmitted helminth infestation
anemia status in included studies.
Anemia status in included studies:
The studies reported a wide variation in anemia across
various states of India, particularly in studies focusing on
hemoglobinopathies. In Punjab, 38.7% of the pregnant women
were found to be anemic, In Maharashtra, one study noted that
all pregnant women had microcytic anemia, In Karnataka, 46.7%
of the women were anemic, whereas another study from the
state showed a lower prevalence of 22.7%. A study from Madhya
Pradesh reported 47% anemia prevalence, with another study
from the same state reporting 42.8%. Other states such as New
Delhi, Maharashtra, Gujarat, Jodhpur, and West Bengal did not
report anemia prevalence in the studies. The prevalence of anemia
in the infectious diseases was notably high. Madhya Pradesh
reported 79% anemia, while Andhra Pradesh and Telangana
had an even higher rate of 92.4%. Rajasthan recorded 88.3%
anemia prevalence, and Jharkhand reported 86%. Chhattisgarh
had 73.2% anemia and another study did not report anemia. In
Puducherry, 63.3% of the population was anemic. These figures
suggest a significant burden of anemia across different states,
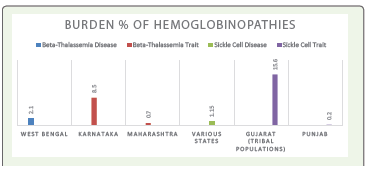
particularly in areas affected by infectious diseases.Burden of hemoglobinopathies among pregnant women:
We included seven teen studies that estimated the prevalence
of hemoglobinopathies among pregnant women in India. The only
identified study that reported the prevalence of beta-thalassemia
disease reported a 2.1% prevalence in West Bengal. Among the
included studies, the prevalence of beta-thalassemia trait was
the highest at 8.5% in Karnataka, and the lowest was reported
in a study in Maharashtra (0.7%). The prevalence of sickle
cell disease reported in the studies were between 0.7 – 1.6%.
Thehighest prevalence of sickle cell trait (15.6%) was reported
among tribal populations of Gujarat. Punjab reported the lowest
prevalence of sickle cell trait (0.2%).Burden of infectious diseases:
We included ten studies that reported the prevalence of
infectious diseases among pregnant women in India. As shown
in [Table 1] out of the eight studies that estimated the prevalence
of malaria infection, the highest (29.3%) and the lowest (0.8%)
prevalence were reported in Chhattisgarh. One study reported
the prevalence of tuberculosis to be 1.8% among pregnant
women in Puducherry. One study reported a 6.5% prevalence of
soil-transmitted helminth infestation among pregnant women in
Maharashtra.
The burden of chronic disease (chronic kidney disease, chronic liver disease) among pregnant women:
We failed to identify any study reporting the prevalence of
chronic diseases (chronic kidney disease, chronic liver disease)
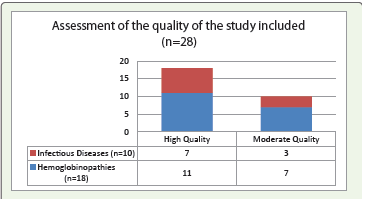
among pregnant women in India.Study Quality Assessment:
Out of the twenty-eight studies included, eighteen (64.2%)
were rated as high-quality studies, and the remaining ten (35.7%)
were rated to be of moderate quality. Out of the eighteen studies
reporting on hemoglobinopathies, eleven studies were assessed
to be of high quality and the remaining seven were of moderate
quality. Out of ten studies reporting on infectious diseases,
seven were of high quality and the remaining three studies were
of moderate quality as can be seen in [Figure 7].Discussion
This systematic review attempted to assess the burden of
various non-nutritional causes of anemia. The burden of betathalassemia
disease of 2.1% and beta-thalassemia trait ranged
from 2.2 to 8.5%. Studies from other countries reported the
prevalence of beta thalassemia disease 3.6% in Lao, 3.8% in
Thailand, 1.3% in China and 0.5% in Bangladesh. Similarly, the
prevalence of beta thalassemia trait reported in the included
studies was similar to that reported in Pakistan (6%) and
Indonesia (5.7%).[39-42]The prevalence of sickle cell disease
in our review ranged from 0.7 to 1.6% and that of Sickle cell
trait from 1.5 to 15.6%.Other countries like Africa and United
Kingdom estimated around 1% sickle cell disease prevalence
among pregnant women which is similar to that reported in
studies from India.[43,44]
Not many studies have been conducted to assess the prevalence
of hemoglobinopathies among Indian pregnant women. Most
of the studies conducted were hospital-based or conducted in
specific population groups with small sample sizes. India has a
diverse population and consanguineous marriage is common in
many cultural groups in India, leading to hemoglobinopathies
being concentrated in certain geographical areas and among
certain population groups. Hence the findings of these studies
may not be generalizable at the population level. This evidence
suggests the need for more studies, especially community-based
large studies, in more representative population groups to
estimate the actual prevalence of different hemoglobinopathies
among pregnant women in the country.
The review reported the prevalence of malaria in the range
of0.8 to 29.3% among pregnant women in India.[27-33] Other
countries reported prevalence of malaria rangingfrom 18–40%
in Burkina-Faso, 32% in Zambia, 29% in Congo, 27% in Uganda,
13% in Tanzania, 12% in Liberia and 4% in Ethiopia.(45–49)
Previous studies show that the prevalence of malaria is lower
in Asian countries as compared to Africa. It was found to be
around 6% in Laos and 0.4% in Afghanistan.[50,51]Within
India, there is wide geographical variations in the prevalence of
malaria among pregnant women,likely attributable to the wide
variations in geography, terrain and climatic conditions including
precipitation. Most of the studies that reported the prevalence of
malaria among pregnant women were conducted in Chhattisgarh
and neighboring states which are endemic for malaria. Studies
assessing the prevalence of tuberculosis and other infectious
causes of anemia in pregnancy were limited. There is need for
nationally representative studies that assess the prevalence of
different infectious causes of anemia so as to take appropriate
measures to tackle them.
India, over the last fifty years has implemented several
national-level programs to supplement IFA in pregnancy.
However, anemia levels continue to remain high. In addition
to measures to address the nutritional causes of anemia,
there is a need to pay due attention to the non-nutritional
causes of anemia. The National guideline on Prevention and
Control of Hemoglobinopathies was launched in the year 2016
which provides a strategic framework for the prevention and
management of hemoglobinopathies in the country. The National
Vector Borne Disease Control Programme (NVBDCP) of the
Government of India and the National Strategic Plan for Malaria
Elimination in India 2017–2022 attempts to eliminate malaria in
a phased manner in the country. The recently launched Anemia
Mukt Bharat (AMB) strategy has introduced a 6*6*6 intervention
strategy highlighting the need for addressing non-nutritional
causes of anemia to reduce the burden of anemia in India. One
of the six interventions under the AMB strategy is to intensify
awareness, screening, and treatment of non-nutritional causes of
anemia with special focus on malaria and hemoglobinopathies in
the endemic pockets of the country. There is a need for integrating
various programs and guidelines addressing non-nutritional
causes for the effective control of anemia in the country. Existing
platforms in health care centers, anganwadi centers, VHNDs,
Nutrition week, and World Thalassemia Day can serve as avenues
to create awareness about non-nutritional causes of anemia.
Frontline workers like ASHAs, ANMs, and health workers need to
be trained in screening for carrier status of hemoglobinopathies,
prevention and care of disease, and counseling diseased/carrier
couples and their families.
Strength:
To best of our knowledge the first systematic review
to summarize the evidence from published studies on the
prevalence of non-nutritional causes of anemia among pregnant
women in India. The review included all the studies published
during the last 12 years.Limitation:
The number of studies eligible for inclusion in this review
was limited, which might have affected the estimates of burden
different non-nutritional causes of anemia among pregnant
women in India. Moreover, most of the studies were hospitalbased
and concentrated in specific geographical regions or
population groups leading to the non-generalizability of findings
of the study. No studies were available that assessed the
prevalence of chronic liver disease and chronic kidney disease
among pregnant Indian women.Conclusions
The prevalence of different non-nutritional causes of anemia
among pregnant women varied highly from region to region.
Small sample sizes and varied study designs challenged drawing
of valid conclusions. There is need for more studies with robust
designs and adequate sample sizes to assess non-nutritional
causes of anemia among pregnant Indian women. Non-nutritional
causes other than hemoglobinopathies and malaria have not
been adequately investigated. Thus, the study advocates the need
for better prevalence
Estimation from nationally representative studies to enhance
our understanding of the burden of different non-nutritional
causes of anemia among pregnant women in India.
Additional File:
Search strategy: PubMed Search: Hemoglobinopathies:
1. (((thalassemia [Title/Abstract])) AND (pregnant [Title/
Abstract])) AND (India[Title/Abstract]) (13) 2. (((Sickle cell
disease [Title/Abstract])) AND (pregnant[Title/Abstract])) AND
(India[Title/Abstract]) (5) 3. (((hemophilia[Title/Abstract])) AND
(pregnant[Title/Abstract])) AND (India[Title/Abstract]) (NIL)
Infectious Diseases: 1. (((malaria[Title/Abstract]))
AND (pregnant[Title/Abstract])) AND (India[Title/
Abstract]) (36) 2. (((tuberculosis[Title/Abstract])) AND
(pregnant[Title/Abstract])) AND (India[Title/Abstract]) (26) 3.
(((helminths[Title/Abstract])) AND (pregnant[Title/Abstract]))
AND (India[Title/Abstract]) (3)
Chronic disease: 1. (((chronic kidney disease [Title/
Abstract])) AND (pregnant[Title/Abstract])) AND (India[Title/
Abstract]) (4) 2. (((chronic liver disease [Title/Abstract])) AND
(pregnant[Title/Abstract])) AND (India[Title/Abstract]) (3)
Google Scholar: Hemoglobinopathies; thalassemia sickle cell
disease “Pregnant women” India (2940)
Infectious Diseases: Malaria Pregnant women India (18,000),
Tuberculosis Pregnant women India (17,700)
India helminths “Pregnant women” (5,500)References
Citation
Khanam A, Ranjith A, Vohra K, Sharma T, and Yadav K. A Systematic Review on the Burden of Non-nutritional Causes of Anemia among Pregnant Women in India. Indian J Nutri. 2024;11(2): 303.