Research Article
Comparison of Efficacy and Feasibility of Global Leadership Initiative on Malnutrition (GLIM) Criteria and Subjective Global Assessment (SGA) To Evaluate the Nutritional Status of Patients at A Tertiary Hospital
Ramani K1 and Swetha A2*
1Clinical Dietitian, Department of Clinical Nutrition, Yashoda Hospitals, Behind Hari-Hara Kala Bhavan, S.P Road, Secunderabad, India
2Deputy Chief Dietitian, Department of Clinical Nutrition, Yashoda Hospitals, Behind Hari-Hara Kala Bhavan, S.P Road, Secunderabad, India
2Deputy Chief Dietitian, Department of Clinical Nutrition, Yashoda Hospitals, Behind Hari-Hara Kala Bhavan, S.P Road, Secunderabad, India
*Corresponding author:Swetha A, Deputy Chief Dietitian, Department of Clinical Nutrition, Yashoda Hospitals, Behind Hari-Hara Kala Bhavan, S.P Road, Secunderabad India Email Id: swetha.anisingaraju@gmail.com
Article Information:Submission: 28/05/2024; Accepted: 22/06/2024; Published: 25/06/2024
Copyright: © 2024 Ramani K, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background:Over one billion people suffer from malnutrition as a result of illness, financial hardship, starvation, conflict, and natural disasters. The gold standard for identifying malnutrition in hospitalized patients is Subjective Global Assessment (SGA) as it is a common occurrence. Nevertheless, the
American Society of Parenteral and Enteral Nutrition (ASPEN) and the European Society for Clinical Nutrition and Metabolism (ESPEN) have proposed new assessment tools in the last few decades, such as the Global Leadership Initiative on Malnutrition (GLIM), but there hasn’t been much research done on the
accuracy of these tests.
Methodology:This observational study conducted at tertiary hospital which includes 100 subjects of age group (18-60 years) with or with-out comorbidities. The nutrition risk was diagnosed with a systemic nutritional risk screening (NRS) and nutritional assessment was done with SGA and GLIM criteria. While the GLIM recommends using DEXA (Dual X-ray absorptiometry, (BIA Bioelectrical Impedance Analysis), and CT (Computerized Tomography) scans to evaluate the decreased muscle mass, in the present study, TSF, MAMC, MUAC and hand grip were used as functional measures.
Results:Data obtained revealed that about 97% were moderately malnourished when screened with NRS tool. Further the assessment tools SGA and GLIM reported that 65% and 73% of the subjects were moderately malnourished whereas 5% and 27% subjects were severely malnourished.
Conclusion:This study concludes that the majority of the hospitalized patients were moderately malnourished. GLIM shows the fair sensitivity and accuracy in depicting the nutritional status of the patients than SGA and demonstrates that the practicality of GLIM was difficult.
Methodology:This observational study conducted at tertiary hospital which includes 100 subjects of age group (18-60 years) with or with-out comorbidities. The nutrition risk was diagnosed with a systemic nutritional risk screening (NRS) and nutritional assessment was done with SGA and GLIM criteria. While the GLIM recommends using DEXA (Dual X-ray absorptiometry, (BIA Bioelectrical Impedance Analysis), and CT (Computerized Tomography) scans to evaluate the decreased muscle mass, in the present study, TSF, MAMC, MUAC and hand grip were used as functional measures.
Results:Data obtained revealed that about 97% were moderately malnourished when screened with NRS tool. Further the assessment tools SGA and GLIM reported that 65% and 73% of the subjects were moderately malnourished whereas 5% and 27% subjects were severely malnourished.
Conclusion:This study concludes that the majority of the hospitalized patients were moderately malnourished. GLIM shows the fair sensitivity and accuracy in depicting the nutritional status of the patients than SGA and demonstrates that the practicality of GLIM was difficult.
Keywords:Glim; Sga; Nrs; Malnutrition
Introduction
Malnutrition is one of the most common clinical conditions
in this population, with estimates of 20–60% of adult hospital
patients having it [1]. The increased needs, excessive nutrient loss
or a combination of both of these make the hospitalized patients
vulnerable to malnutrition. Increased morbidity, mortality, re
hospitalization rates, and health care costs are just a few of the serious
negative effects of malnutrition that have an impact on patients and
the health care system [3].
The fundamental components of nutritional management for
hospitalized patients include nutritional status assessment, risk
factor identification, and early nutritional interventions. Despite
the importance of identifying malnutrition and developing effective
prevention and treatment strategies, a worldwide agreement on the
diagnosis of malnutrition remains elusive. The Global Leadership
Initiative on Malnutrition (GLIM) has recently put forth new
diagnostic criteria to establish global consensus on the fundamental
factors of adult malnutrition diagnosis. These include two etiologic
criteria, lower disease burden/inflammation and reduced food intake
or assimilation and three phenotypic criteria, non-volitional weight
loss, low body mass index, and reduced muscle mass. To diagnose
malnutrition, at least one of the two etiologic and phenotypic criteria
have to be met [4]. Several earlier research have assessed how well
the GLIM criteria identify malnutrition in cohorts with particular
disease [5].
Current study aims to compare the efficacy and feasibility of
GLIM criteria and SGA to evaluate the nutritional status of patients.
Materials and Methods
Research design:Prospective observational study
Study Sample:
This prospective observational study included 100 individuals
from the Inpatient ward.Study Site:
The current study is a single-centre, hospital-based investigation
conducted from January 2023 to March 2023 in various departments
of Yashoda Hospital, Secunderabad.Inclusion criteria:
The study includes male and female, aged >18 to 60 years who
were hospitalized in various departments as inpatients. Every
patient underwent a medical examination in accordance with the
predetermined proforma. Patients were included in the study only
after providing written, informed consent.Exclusion criteria:
The study excludes patients who do not meet the inclusion criteria.
Age groups those under 18 and above 60 years as well as those from
the outpatient clinic and who failed to provide the informed consent
were excluded from the study.The information was collected using a self-administered, semistructured,
and validated questionnaire which includes two parts
such as socio demographic profile, assessment tools (NRS TOOL,
GLIM, SGA). NRS Tool 2002 was used as a common tool for
nutritional screening. GLIM includes, phenotypic criteria (weight
loss, BMI, reduced muscle mass), Etiological criteria (Impaired food
intake, inflammation (albumin and (C-reactive protein (CRP)). SGA
includes (weight loss, functional capacity, BMI, edema/ascites, gastro
symptoms and albumin). The various other anthropometric tools
and instruments were used in data collection are height, weight, BMI,
MUMC, MUAC (Mid-Upper Arm Circumference), Hand grip, TSF,
calf circumference.
Statistical Analysis:
Data was analyzed using Statistical Package for the Social
Sciences (SPSS) version 21.0. Comparison of quantitative variables
like frequency, percentage between the groups was done using the
Pearson chi-square test where p<0.05 was considered statistically
significant.Results
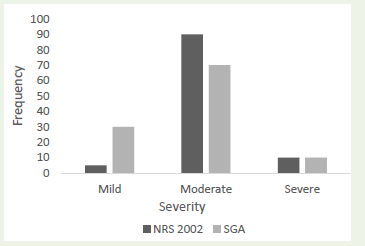
[Figure 1] depicts that the results of the nutritional risk screening
(NRS) showed that the majority of patients had a moderate risk and
the few had a severe or mild risk. When 100 respondents underwent a
nutritional assessment using the Subjective Global Assessment (SGA)
tool, it was found that the majority of patients (>60) and less than
40% fell into the moderate and mild categories, while the few had
severe grades.
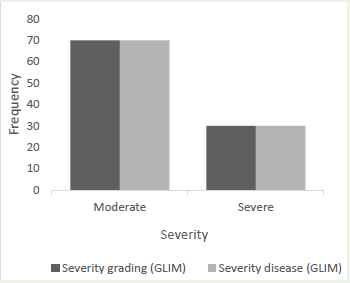
In the current study, after assessing the level of disease severity
using the GLIM criteria, it was found that over 70% of patients had
moderate risk of illness and over 20% had severe risk. The analysis
also showed that >70% and >25% were classified as moderate grade
and severe grade, respectively, based on the GLIM criteria. Utilizing
the recently developed GLIM criteria to evaluate the individual’s
nutritional status, the research showed that 85% of patients were at
risk of malnutrition and less than 20% were not [Figure 2].
[Figure 3] demonstrates that out of 100 patients, 30 had lost nothing
at all, 50% had lost moderate amounts of weight whereas less than 20
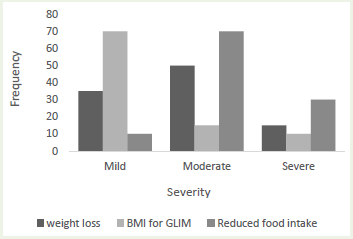
percent had a significant amount of weight loss. Only the low BMI
group (<18.5 kg/m2) was included in the BMI calculation according
to the GLIM assessment tool. The findings showed that, because the
obesity variable is excluded from the GLIM criteria, less than 20
individuals were classified as moderately or severely underweight,
and more than 75% were classified as well or overnourished. Based on
patient memory, the oral food consumption data showed that most
individuals (>60%) had moderate food intake (<50% of oral intake),
while a minimum of (>20%) participants had very low food intake
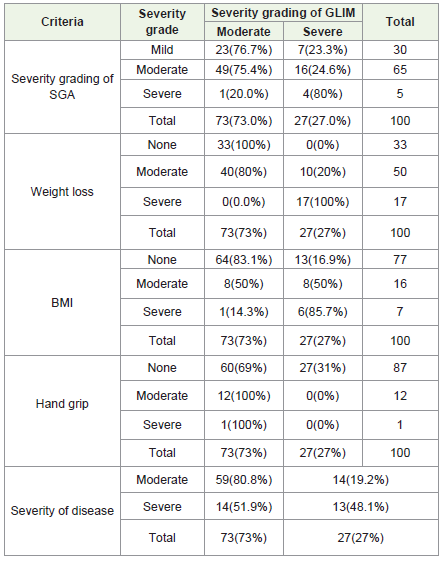
(<25% of oral intake). [Table 1] shows the prevalence of malnutrition
diagnosed by GLIM and other criteria. After SGA diagnosis, 30
patients were malnourished slightly and a GLIM study disclaims that
of these thirty patients, twenty-three were moderately malnourished
and seven were severely malnourished. Results also show that on
SGA diagnosis,65 patients were malnourished moderately and a
GLIM study disclaims that of these 65 patients, 49 were moderately
malnourished and 16 were severely malnourished. SGA and GLIM
reports only 5, 4 patients were severely malnourished whose values
were statistically significant (p= 0.023). Weight loss studies shows that
33 patients were nourished normally and GLIM shows moderately
nourished. In both the studies 17 patients were severely malnourished
indicating the values are statistically significant (p= 0.000). BMI study
shows 77 patients were normal and GLIM reports that of these seventy seven
patients, 64 moderately malnourished and 13 were severely
malnourished. Results also show that on BMI diagnosis,16 patients
were malnourished moderately and GLIM depicts of these 50% were
moderately malnourished and 50% were severely malnourished. BMI
reports only 7 patients were severely malnourished whereas GLIM
reports 6 patients were severely malnourished. These values are
statistically significant (p = 0.000). Results shows maximum patients
(87) were normal with hand grip, whereas with GLIM maximum
(60) were moderately nourished. These values were statistically
insignificant (p= 0.063). On comparison of severity of disease with
GLIM study, severity shows 73% were nourished normally whereas
27% were severely malnourished. GLIM studies show that 80.8% were
moderately nourished and 48.1% were severely malnourished which
depict the values are statistically significant. (p= 0.004).
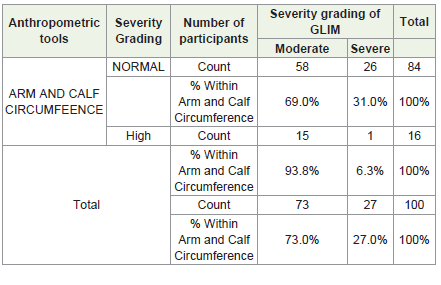
Studies with Arm and calf circumference shows that, 16 patients
were found to be severely malnourished, Nonetheless, the GLIM
study’s findings indicate that 15 patients had moderate malnutrition
and one patient had severe malnutrition [Table 2] . These values are
statistically significant (p= 0.041).
Current study with Arm and calf circumference tool shows that,
84 patients have normal nutrition levels, whereas in the GLIM study,
malnutrition was classified as moderate in 58 (69.0%) and severe in 26
(31.0%) patients, respectively.
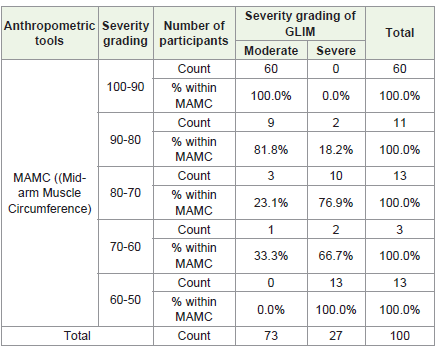
[Table 3] depicts that 60% of patients were with normal muscle
circumference and less than 20 percent patients were with lowest
muscle according to Mid-arm Muscle Circumference (MAMC)
tool, whereas severity grading of GLIM shows that 60 patients were
moderately malnourished and 13 patients were severely malnourished
with low muscle. These values are statistically significant (p= 0.000).
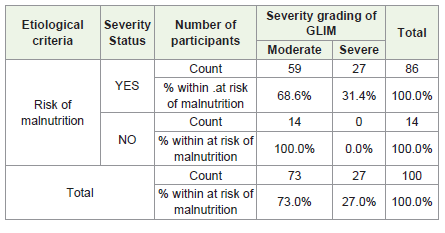
Present results also shows that 86 patients were at the risk of
malnutrition. Severity grading by GLIM study show that, malnutrition
was classified as moderate in 59 (68.6%) and severe in 27 (31.4%)
patients, respectively. Studies also show that 14 individuals have
normal nutrition levels whereas GLIM study’s findings indicate that
14 patients had moderate malnutrition and there is no patient with
evere malnutrition [Table 4] . These values are statistically significant
(p=0.014).
Discussion
Finding out the patient’s nutritional status in relation to SGA’s
superior efficacy over GLIM was the study’s main objective. The
NRS was utilized as a nutritional screening tool in this study and
SGA and GLIM were used as nutritional assessment tools. Loss of
appetite, reduced intake of nutrients and altered lean body mass
anabolism/catabolism play a key role in development of infections.
Loss of appetite, reduced intake of nutrients and altered lean body
mass anabolism/catabolism play a key role in development of
infections [6]. Nutritional approach should be based on a careful
and periodic assessment of nutritional status and on timely dietary
counseling. When protein and energy intakes are reduced, nutritional
supplementation by means of specific oral formulations administered
would be the first-step intervention, and represents a valid nutritional
approach in prevention and treatment of diseases since it is easy,
effective and safe [7]
Systematic analysis of the data revealed that, based on the
NRS 2002 tool, about 97% of the participants were moderately
malnourished. Our study shows that nutritional status of the patients
was determined as severely and moderately malnourished using the
assessment tools SGA & GLIM. Malnutrition diagnosis of hospitalized
patients presents satisfactory criterion validity and results show
that patients were malnourished according to the SGA and GLIM
criteria tools [8]. As a result, the study’s findings indicate that the
GLIM criteria were more accurate in determining malnutrition than
the SGA, the accepted industry assessment instrument. Nutritional
problems deserve more attention in hospitalized patients. Several
studies have explored the relationship between disease prognosis and
malnutrition based on the GLIM [9].
Even though the GLIM criteria have a high degree of accuracy,
there are certain drawbacks in using it frequently. It includes only the
low BMI category, which is being below 18.5 kg/m2, and it excludes
the overweight or obese variable, which makes it difficult to use GLIM
to assess malnutrition in obese or obese sarcopenic patients [10].
Present study results with BMI criteria shows that maximum patients
were normally nourished few were moderately malnourished and
least were severely malnourished. Unintentional weight loss (UWL)
may be used as initial screening for protein-energy malnutrition in
the medical and surgery gastroenterology outpatient setting. The
impact on clinical outcome and of early nutritional intervention in
these settings need to be addressed [11].
Additionally, in order to determine the reduced muscle mass, the
GLIM criteria recommend using DEXA (Dual X-ray absorptiometry)
scans, BIA (Bioelectrical Impedance Analysis), and CT (Computerized
Tomography) scans. However, because the majority of patients
refused to undergo these tests, it was not economically feasible to
do so. In the present study the subject’s decreased muscle mass,
anthropometric and functional measurement instruments including
hand grip, MUAC, TSF, MAMC, and calf muscle circumference
were used to access the nourishment levels which was significantly
correlated with the GLIM severity of the grading.
As per the previous study, 37.8% and 32.8% of the GLIM and
SGA diagnosed had been classified as malnourished which shows
GLIM assesses malnutrition with a fair degree of accuracy when
compared to SGA. The study also revealed that, in contrast to
SGA, which allows for physical examination of the patient, GLIM
required more time for patient assessment analysis, and also the
manual evaluation of variables [12]. The data on decreased muscle
mass was not feasible because of real-world obstacles or difficult
when using BIA [13]. Malnutrition is a mostly modifiable condition
with potentially deleterious consequences, if left untreated.
Malnourished patients can be detected early and treated in a timely
fashion through comprehensive nutritional care management. This
contributes to improvements in the patient’s clinical outcome [14].
An interdisciplinary approach and nutritional therapies are effective
in cost containment (improving quality of treatment, avoiding
unnecessary interventions, and simplifying management), which is
especially relevant for the modern healthcare policy [15].
Conclusion
The study finds that most hospitalized patients had moderate
malnutrition, and that, when compared to SGA, the GLIM criteria
demonstrated a fair level of sensitivity and accuracy in determining
the patients’ nutritional status among the two assessment instruments.
Furthermore, the study concludes that GLIM tool feasibility was
more difficult than SGA because of a number of real-world obstacles.
Acknowledgements
The authors would like to thank Management Yashoda Hospitals
for continuous support and special thanks to Dr. Amidyala Lingaiah
(Director of Medical Services Yashoda Hospitals).
References
Citation
Ramani K, Swetha A. Comparison of Efficacy and Feasibility of Global Leadership Initiative on Malnutrition (GLIM) Criteria and Subjective Global Assessment (SGA) To Evaluate the Nutritional Status of Patients at A Tertiary Hospital. Indian J Nutri. 2024;11(2): 294.