Research Article
The Relationship between Dietary Practices and Nutritional Status of Children Aged 24-59 Months in Chitokoloki Ward, Zambezi District, Zambia
Nkhoma O1, Chipili G1* and Ukegbu PO2
1Department of Nutritional Sciences, School of Applied Sciences and Technology, Mukuba University, P.O. Box 20382. Itimpi, off Chingola Road, Kitwe, Zambia
2Department of Human Nutrition and Dietetics, Michael Okpara University of Agriculture, Umudike PMB 7267, Abia State, Nigeria.
2Department of Human Nutrition and Dietetics, Michael Okpara University of Agriculture, Umudike PMB 7267, Abia State, Nigeria.
*Corresponding author:Chipili G, Department of Nutritional Sciences, School of Applied Sciences and Technology, Mukuba University, P.O. Box 20382. Itimpi, off Chingola Road, Kitwe, Zambia. Email: chipiligiven@yahoo.com
Article Information:Submission: 12/01/2024; Accepted: 18/03/2024; Published: 22/03/2024
Copyright: © 2024 Nkhoma O, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
This study evaluated dietary practices and nutritional status of children aged 24-59 months old in Chitokoloki ward of Zambezi East Constituency, Zambia. A cross sectional study was conducted among 364 children (aged 24-59 months) randomly selected from households in Chitokoloki ward in Zambezi. Sociodemographic
information and dietary practices of children were collected from mothers/caregivers using an interviewer-administered questionnaire. A 24-hour dietary recall questionnaire of the child’s food consumption during the previous 24-h was used to obtain information on dietary diversity. Dietary diversity scores <5 indicated minimum dietary diversity (MDDS). Anthropometry of children were measured and Height-for-age (HAZ), weight-for-age (WAZ), Weight for-height (WHZ) and body mass index-for-age (BAZ) Z-scores were used to determine nutritional status using WHO Anthroplus software. Chi square and logistic regression were used to determine the relationship between dietary practices and nutritional status at p value less than 0.05. The findings revealed that dietary practices of the children were poor as depicted by consumption of <3 meals daily (32.9%) and low dietary diversity score <5 (69.8%). The prevalence of wasting, stunting, underweight, obesity were 11%, 26.5%, 15.0%, and 5%, respectively. Dietary practices were not significantly associated with anthropometric status of the children (p>0.05). This study recommends the need for nutritional interventions and education to promote a more balanced and diverse diet among these children.
Keywords:Dietary Practices; Feeding Practices; Nutritional Status; Malnutrition; Under Five Children
Introduction
Malnutrition poses a significant public health challenge,
particularly among children under five, in many low- and middle income
countries, including Zambia. Malnutrition is a condition
that results from insufficient or excess intake of nutrients, as well as
micronutrient deficiencies [1]. There are various types of malnutrition,
encompassing two overarching categories: undernutrition and
overnutrition. Undernutrition presents as either wasting or low
weight for height (acute malnutrition), stunting or low height for
age (chronic malnutrition), underweight or low weight for age, and
deficiencies or excesses in minerals and vitamins [2]. Over nutrition
includes overweight, obesity and diet-related non-communicable
diseases (NCDs) such as diabetes mellitus, heart disease, some
forms of cancer and stroke [2]. The immediate consequences of
malnutrition in young children include cognitive impairment,
potentially irreversible, and the risk of non-communicable diseases in
later life. Additionally, malnutrition can weaken the body’s ability to
combat infections, impair wound healing, and disrupt the regulation
of salt in the kidneys, potentially leading to issues of overhydration
or dehydration [3].
In 2022, global statistics revealed that among children under five
years old, approximately 22.3 percent were stunted (148.1 million),
6.8 percent were wasted (45 million), and 5.6 percent were overweight
or obese (37 million) [4]. Stunting and wasting were more prevalent
in rural areas, with stunting being 1.6 times higher and wasting
1.4 times higher compared to urban areas, while the prevalence of
overweight was only slightly higher in urban children (5.4 %) than
in their rural counterparts (3.5 %) [4]. In Zambia, data from the
2018 Demographic and Health Survey (ZDHS) reveals that 35% of
children under 5 are stunted, with 12% severely stunted. Boys have
a higher stunting rate (38%) than girls (31%) [5]. Urban areas show
a slightly lower stunting prevalence (32%) compared to rural areas
(36%) [5]. Wasting affects approximately 4% of under-five children,
with 2% being severely wasted [5]. Wasting rates are similar between
boys (5%) and girls (4%). Overweight affects 5% of children under 5,
while 12% are underweight in Zambia [5].
The nutritional status of children under the age of five is intricately
linked to the dietary practices of their primary caregivers, typically
mothers or other family members. However, a lot of children around
the world are not eating the nutrient-rich foods they need to grow
and develop. Statistics show that globally, 50% if children were not
fed the minimum number of meals or snacks recommended each day
[6]. More than two 69% were not fed foods from at least five of the
eight recommended food groups [6]. Feeding practices of children in
Zambia show low intake of protein rich foods and high consumption
of carbohydrate rich foods. Their diet is mainly composed of cereals,
predominantly maize, starchy roots and, to a lesser extent, fruit and
vegetables, [6]. Research in Zambia has demonstrated that mostly
children under the age of five exhibit low dietary diversity. For
example, a survey of children aged 24 to 59 months in Zambia found
that only 29.6% met the minimum dietary diversity [6]. Another
study by Alamu et al showed that dietary diversity was low (37.3%)
in Zambia [7].
Previous studies have investigated the relationship between
dietary practices/dietary diversity and nutritional status of under
five children. A recent study by Samosir, Radjiman and Aninditya
found that the diversity of food consumption (AOR = 1.15; 95%CI:
1.07–1.24) significantly and statistically influenced nutritional
status of children age 6–23 months in Indonesia [8]. They noted
that higher odds of achieving normal nutritional status, as opposed
to being stunted or severely stunted, were linked to adhering to
dietary diversity in food consumption [8]. In the study by Motadi
and colleagues, a low diversity diet was positively associated with
weight for age and height for age, but not with weight for height. As
the number of food categories decreased, the likelihood of developing
problems with weight for age and height for age increased [8].
Children with a dietary diversity score of less than 4 were significantly
at risk of being underweight and stunted compared to those with a
score of ≥ 4. However, weight for height did not show a significant
association with a reference value greater than 4 [9].
In Zambia, studies on the relationship between dietary practices
and nutritional status of children aged 24-59 focusing on a rural setup
like Chitokoloki Ward are limited. In view of this, this study sought
to investigate the dietary practices of caregivers, the nutritional
status of children aged 24-59 months, and the relationship between
these variables. By shedding light on these aspects, the research
aims to provide evidence-based insights that can guide efforts to
reduce malnutrition, enhance child health outcomes, and ultimately
contribute to the well-being and development of young children in
Chitokoloki Ward and similar rural communities in Zambia.
Materials and Methods
Study design and area:
This cross-sectional descriptive study conducted from February
to April was conducted to assess dietary practices and nutritional
status of children 24-59 months in Chitokoloki ward, located in the
Zambezi East constituency of Zambezi District, Zambia.Study participants:
The study participants mother/caregivers with children aged 24-
59 months selected from households in Chitokoloki ward.Sample Size Determination and sampling technique:
Sample size was calculated based on a single proportion
population formula Z2×p (1-p) /d2 as follows; Z is standard normal
deviation set at 1.96 corresponding to 95% confidence interval (CI)
and p; p is the estimated proportion of children aged 24-59 months
old in northwestern province of Zambia who are stunted (32%) (11);
and d is the desired level of precision (0.05) Therefore, n = [(1.96)2
(0.32) (0.68) / (0.05)2] = 3.8416 x 0.32 x 0.68/0.0025= 0.83593216
/ 0.0025 = 334.27= 334. Hence, a minimum sample size of 334 was
calculated and a 10% attrition rate was added to obtain a sample size
of 367.Households with mothers/caregivers and their children aged
24-59 months old were selected using a random method. Stratified
random sampling was used to divide Chitokoloki ward into strata and
then random selection of the households from the different sections
was done using systematic random sampling.Data collection
A researcher-administered questionnaire was used to collect
quantitative data on demographic and socio-economic characteristics
of the households, dietary practices, dietary diversity and qualitative
24hour recall. The questionnaire was pre-tested on a group of mothers/
caregivers in a non-sampled ward in Zambezi east constituency on 37
mothers with similar characteristics to the sampled study population.
Questionnaire: Structured questionnaires were used to collect
information on socio-demographic characteristics of mothers/
caregivers. The questionnaires were administered by trained research
assistants and researchers to mothers/caregivers with children
24-59months old in the households. A total of 367 questionnaires
were distributed and 364 retained, representing a 99.2% response
rate.
Anthropometric measurements and indicators: Anthropometric
assessment for each child were determined following standard
procedures. Measurements were taken in triplicate for height and
duplicate for weight using calibrated equipment before finding the
average in line with UNICEF regulations [10]. Measures included
standing height, weight and mid-upper arm circumference [11].
Height was measured to the nearest 0.1cm using a ASECA 217 portable
stadiometer; and weight to the nearest 001 kg on a standardized
Mechanical Salter scale and SECA scale.The anthropometric status
of the children was categorised by using the appropriate cut-offs for
classification established by the World Health Organization [12].
Measurements of weight and height were converted to age and sex specific
z-scores to establish anthropometric status, according to the
World Health Organization Anthro [13]. For underweight, wasting
and stunting, the cut-off marks were >-2SD. The cut-off value for
malnourished was <13.5cm.
Dietary practices: Dietary practices were assessed using the
dietary diversity score and the number of meals eaten daily by the
children.
Dietary Diversity: Dietary diversity score was calculated based
on 24 h recall of mothers of the child’s consumption of 8 food groups
within the past 24 h (Food and Agriculture Organization, 2007). The
foods consumed by children the day before the survey were classified
into the following seven food groups according to WHO protocol
(17) as follows:
(1) breast milk
(2) grains, roots and tubers and plantains
(3) pulses (beans, peas, lentils) seeds and nuts
(4) daily products (milk infant formula, yoghurt, cheese)
(5) flesh foods (meat, fish, poultry, organ meets)
(6) eggs
(7) vitamin A-rich fruits and vegetables (leafy green vegetables,
yellow fruits and vegetables)
(8) other fruits and vegetables (12). A DDS of 5 was considered
as the minimum DDS. Accordingly, a child with a DDS of less than 5
was classified as having low dietary diversity.
Statistical Analysis
Data was analyzed using Statistical package for Social Sciences
(SPSS) software version 26. WHO Anthro was used to calculate
WHZ (wasting), HAZ (stunting), WAZ (underweight) and BAZ
(overweight/obesity). Descriptive statistics (frequencies, percentages,
means and standard deviation) were computed for socio demographics
and dietary practices. Chi Square analysis and Logistic
regression analysis were used to assess the relationship between
dietary practices and nutritional status at p-value less than 0.05.
Ethical Approval:
Approval for the study was obtained from the Tropical Diseases
Research Centre (TDRC) in Ndola Zambia with ethic approval
number 00003729.Results
Characteristics of children and mothers/caregivers:
Results on [Table 1] revealed that characteristics a total of 364
under five children were recruited to participate in this study. The
study had more female (52.5%) than males (47.5%) children. About
a third (35.7%) of the children were aged between 49-59 months old.
The findings demonstrated that roughly half of the children (50.5%)
possessed a Birth weight ranged from 3.1 to 4.0 kilograms (50.5%),
majority were exclusively breastfed (98.9%), 97.5% were immunized
and less than half (46.2%) had suffered an illness in the past one
month.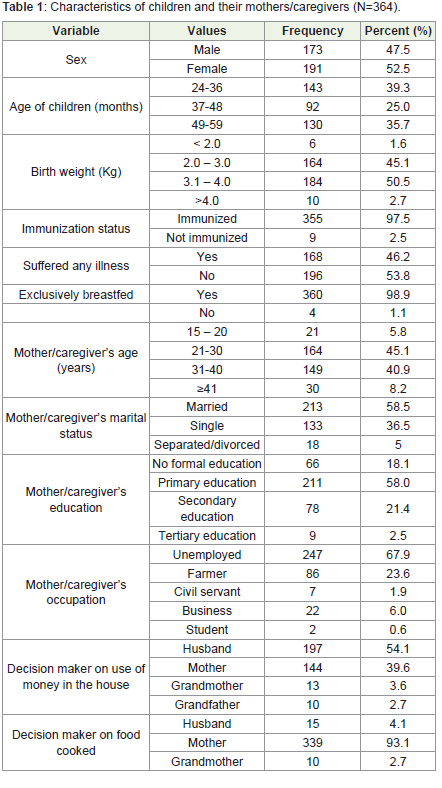
Majority (45.1%) of the Mothers/caregivers were between the ages
of 21-30. More than half of them had formal education up to primary
education (58%) and were unemployed (67.9%). The majority of the
women and caregivers were married (58.5%) and were unemployed
(67.9%) and only 23.6% were farmers. Most of the households had
husbands/fathers decide how money is used (54.1%) while the
mothers/wives decide what is to be eaten (93.1%).
Dietary Practices:
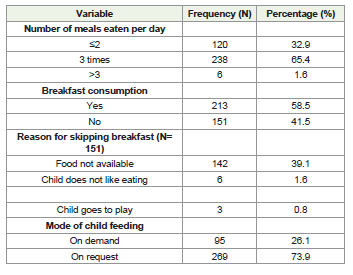
Dietary Practices of children:[Table 2] show some of the dietary
practices adopted by the mothers/caregivers for their children.
Slightly below two-thirds (65.4%) of the children had three (3) meals
per day and 41.5% skipped breakfast. Food not being available was
the major reason for skipping breakfast (39.1%) and majority of the
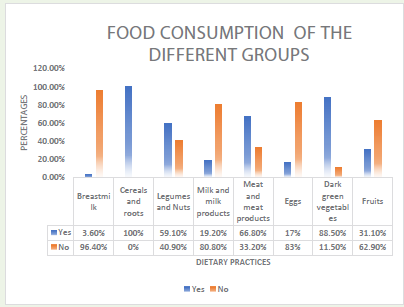
children were fed on request (73.9%).Consumption of food from different foods groups:[Figure 1]
shows the frequency of consumption of foods from different foods
groups. Results revealed that majority (94.60%) were no longer
breastfeeding, while a substantial proportion (88.50%) consumed
dark green vegetables daily. All children had cereals and roots (100%)
included in their diets, whilst legume and nut consumption were
reported by 59.1%. Milk and milk products were notably absent from
the diets of most children (80.80%), with only 19.20% incorporating
them. Meat and meat products were consumed by approximately
two-thirds (66.80%) of the children, while eggs were included by only
17%. Additionally, fruit consumption was relatively low (31.10%),
suggesting limited fruit intake among the children.
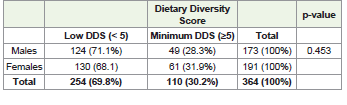
Dietary Diversity Score of children:[Table 3] shows the Dietary
Diversity Score grades of the participants. DDS ranged from 1 to
7 and a DDS of less than 5 was classified as low dietary diversity.
Slightly more than two-thirds (69.8%) of the children had low Dietary
Diversity Scores, only 30.2% of the children achieved a minimum
DDS of more than 5 food groups as recommended by WHO. The
table further shows that males (71.7%) had lower dietary diversity
scores than the females (68.1%), though this was not significant
(p>0.05).
Nutritional status of the children:
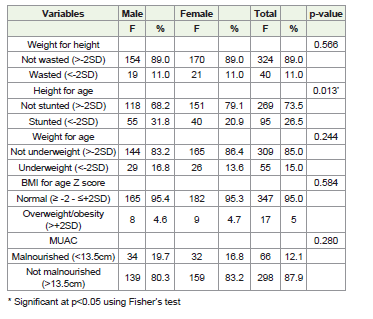
Nutritional status of children based on sex:[Table 4] shows
the anthropometric characteristics of the participants based on sex.
The prevalence of wasting, stunting, underweight, obesity and low
MUAC were 11%, 26.5%, 15.0%, and 5%, respectively. The prevalence
of stunting was higher among male compared to female children
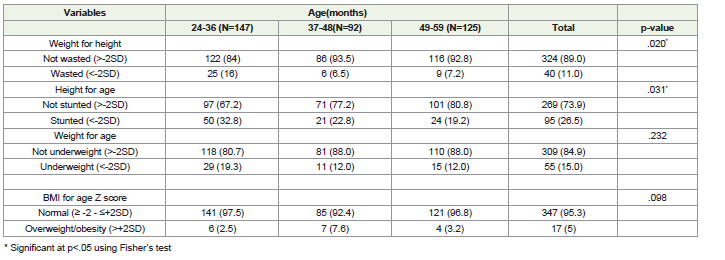
(p<0.013).Nutritional status of the children based on age:[Table 5] shows
the anthropometric status of the children based on age (months).
Comparison based on age showed wasting and stunting were
significantly higher among children aged 24-36 months (p=0.020 and
p=0.031), respectively.
Relationship between Dietary Practices and anthropometric Status:
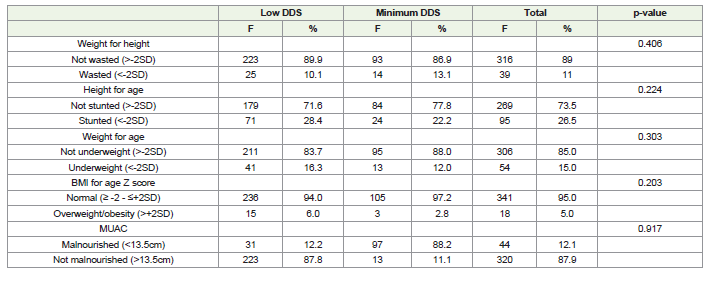
Bivariate relationship between dietary practices and nutritional
status:[Table 6] illustrates the relationship between dietary practices
and nutritional status. While there were slight disparities in the
nutritional status of children with low Dietary Diversity Score (DDS)
compared to those who met the minimum DDS criteria, such as the
higher stunting rate in children with low DDS (28.4%) compared
to those with the minimum DDS (22.2%), this difference was not
statistically significant (p-value = .224). In summary, the analysis
revealed no statistically significant (p > 0.05) difference in nutritional
status between children who achieved a minimum DDS and those
with low DDS.[Table 7] investigates the association between Dietary Diversity
Score (DDS) and the nutritional status of under-five children,
employing binary logistic regression analysis. The key findings are
summarized below:
Weight for Height (WHZ): No significant relationship was found
between DDS and Weight for Height (p-value = 0.408).
Height for Age (HAZ): The odds of stunting were 28% lower
for children with minimum DDS compared to those with low DDS,
but this result was not statistically significant (AOR = 0.720, 95% CI
[0.424, 1.224]; p-value = 0.225).
Weight for Age (WAZ): The odds of being underweight were
29.6% lower for children with minimum DDS compared to those
with low DDS (AOR = 0.704, 95% CI [0.361, 1.375]). However, this
result did not reach statistical significance.
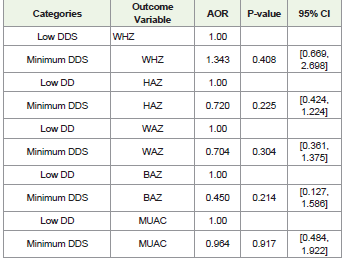
BMI for Age (BAZ): No statistically significant relationship was
found between DDS and BMI for Age (p-value = 0.214).
Mid-Upper Arm Circumference (MUAC): No statistically
significant relationship was found between DDS and MUAC (p-value
= 0.917).
In a nutshell, the analysis indicates that there is no statistically
significant association between DDS and Weight for Height, Height
for Age, BMI for Age, or MUAC. Although there are observed
decreases in the odds of stunting and underweight for children with
a minimum DDS, these reductions are not statistically significant in
this study.
Discussion
The study assessed the relationship between dietary practices/
diversity and nutritional status of children 24-59 months in
Chitokoloki ward, Zambezi District, Zambia. The revealed that 32.9%
of the children do not consume up to three meals per day, following
a traditional meal pattern that includes breakfast, lunch, and super.
More than two third had low DDS with cereals and roots (100%) and
consumed dark green vegetables (88.50%) commonly consumed while
eggs, milk and milk products and fruits were relatively less frequently
consumed. The prevalence of stunting, wasting, underweight and
overweight/obesity were 11%, 26.5%, 15.0% and 5%, respectively. The
was no significant relation between dietary practices/diversity and
anthropometric status.
The practice of children not consuming up to three meals a day as
reported in this study is lower than a similar study in Nigeria, which
reported 78.9% adherence to three meals per day [23]. Notably, the
nutritional quality of these meals was not assessed in this study.
Regarding reasons for missing meals such as breakfast, the study found
that food unavailability at home was the primary cause of breakfast
skipping (39.1%). These findings underline the food security and
access challenges faced by a portion of the studied population. This
situation has health implications, particularly concerning breakfast’s
role in providing energy for the day and supporting cognitive and
physical function.
The study provided insights into the frequency of consumption
of foods from different groups by the children. While dark green
vegetables, cereals, and roots were commonly consumed, there was
limited inclusion of milk, eggs, and fruits in children’s diets. The
findings indicate that while carbohydrates are a prominent part
of diets of the children, there is a notable lack of diversity in food
choices, particularly regarding animal-based proteins (egg and milk
products) and fruits. This dietary pattern may have implications for
overall nutritional balance and access to essential nutrients from
a varied diet. The insufficient consumption of adequate protein
from eggs and milk, along with a deficiency in fruit intake among
children aged 24-59 months in the community, bears profound
implications for their health and development. The amalgamation
of protein inadequacy and nutritional gaps from eggs, milk, and
fruits contributes to an overall nutritional deterioration, posing
multifaceted risks to health and well-being. Furthermore, these earlylife
nutritional deficiencies can have enduring health ramifications,
predisposing individuals to chronic diseases in adulthood and
perpetuating public health challenges. These findings align with
similar research conducted in various regions, all of which highlight
a common dietary pattern among children characterized by a high
consumption of carbohydrate-rich foods and limited intake of foods
of animal origin, fruits, and vegetables [6,4,15].
The low prevalence of meeting minimum DDS (30.2%) is
somehow consistent with previously reported prevalence of 32% in
other parts of Zambia (Luapula Province)[16].
The study found that the prevalence of wasting, stunting,
underweight, and obesity were 11%, 26.5%, 15.0%, and 5%,
respectively. This implies that just over a quarter of the children
were short for their age (stunted). Similarly, UNICEF reported that
stunting was 30% (23% stunting and 7% severely stunted) in children
under-5 years [17]. In addition, Nti and Lartey in their study of
under-5 children in Manya Krobo District in the Eastern region of
Ghana revealed a stunting rate of 20% lower than the national rate of
prevalence[18].
The study’s findings indicated variations in the prevalence of
malnutrition indicators based on age and sex, with stunting more
common in males, wasting highest among the youngest children,
and underweight showing no significant sex difference. These results
emphasize the need for targeted nutritional interventions for specific
age groups and gender to address the nutritional challenges faced by
young children in the study population.
The analysis of the association between dietary practices and
the nutritional status of children under five in this study did not
reveal a statistically significant relationship (p>.05). Results of this
study are consistent with the findings of a study done in Indonesia
in which also found no association between feeding practices and
the nutritional status of under-five children based on Weightfor-
Age (WAZ), Height-for-Age (HAZ), and Weight-for-Height
(WHZ) [19]. However, findings from this study differ from those
of a survey conducted by Darkwa in Ghana, which identified a
significant association between children’s nutritional status and
their feeding practices [20]. Additionally, another study found that
feeding practices did impact the nutritional status of under-five
children in Simanjiro District, Tanzania [21]. In summary, this study
did not establish a significant link between dietary practices and the
nutritional status of children under five in the study area. This could
be due to the homogenous distribution of the study the population.
Nevertheless, results highlight the variability of such relationships,
which can vary across different studies and populations.
Conclusion
This study provides valuable insights into dietary practices and
anthropometric status of children under five, as well as the potential
relationship thereof. The findings highlighted both positive dietary
practices and areas that require attention. The findings showed
that dietary practices/diversity was low. It was established that
consumption of starchy staples was common with low consumption
of protein rich foods required for growth by under 5 children.
Furthermore, no relation between dietary practices/diversity and
anthropometric status. This study offers valuable insights into the
dietary practices and anthropometric status of children under five,
shedding light on potential relationships between the two. While
positive dietary practices were identified, the study also pinpointed
areas that demand attention. This suggests a dissociation between
the diversity of dietary practices and the measured anthropometric
indicators, emphasizing the need for targeted interventions to address
nutritional gaps in the studied population.
Author Contributions:The following statements should be used
“Conceptualization, ON.; methodology, ON, GC, PE.; validation,
GC, PE.; formal analysis, ON, GC, PE; investigation, ON.; resources,
ON.; data curation, ON.; writing—original draft preparation, ON.;
writing—review and editing, ON.; visualization, ON.; supervision,
GC, PE; project administration, ON.;. All authors have read and
agreed to the published version of the manuscript
Acknowledgments:The authors would like to acknowledge the
contributions of all participants and support rendered by Mukuba
University staff and post-graduate students
Conflicts of Interest:The authors declare no conflict of interest
Conflicts of Interest:The authors declare no conflict of interest
References
Citation
Nkhoma O, Chipili G, Ukegbu PO. The Relationship between Dietary Practices and Nutritional Status of Children Aged 24-59 Months in Chitokoloki Ward, Zambezi District, Zambia. Indian J Nutri. 2024;11(1): 286.