Research Article
Evaluation of a Community-Based Intervention to Improve Dietary Patterns and Nutritional Self-Efficacy among Adolescents in Two Districts of Odisha
Priyanshu R1*, Santosh C2, Rohit P1, Sunil M1 and Shantanu S1
1Department of Maternal, Newborn and Child Health and Nutrition, MAMTA Health Institute for Mother and Child New Delhi, India.
2Department of Monitoring and Evaluation, MAMTA Health Institute for Mother and Child New Delhi, India.
*Corresponding author:Priyanshu Rastogi, Department of Maternal, Newborn and Child Health and Nutrition MAMTA Health Institute for Mother and Child New Delhi, India. Email Id: priyanshu@mamtahimc.in
Article Information:Submission: 07/12/2023; Accepted: 29/12/2023; Published: 03/01/2024
Copyright: © 2024 Priyanshu R, et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: A high prevalence of under nutrition and micronutrient deficiencies among adolescents has been observed in South Asia due to restricted dietary variety and unhealthy dietary habits. The present study aimed to assess the change in the health and nutrition practices of adolescents in the Bolangir
and Nuapada districts of Odisha after 2-year community-based intervention.
Methods: The baseline and endline were conducted using a quantitative cross-sectional research method with boys and girls (10-19 years). Predesigned, pretested, semi-structured questionnaires were developed to capture information on socio-demographic profiles, knowledge and practices related to diets and dietary patterns, access to Anganwadicenters, WASH habits, and self-efficacy. The intervention included four group-based structured education sessions and community-based events like role plays, video shows, games-based learning, and folk dances. In total, 673 boys and girls at baseline and 793 at end line participated in the surveys. We employed linear and logistic regression analysis to estimate the degree of change in outcomes at end line compared to the baseline and dose-response analysis to estimate the effect of the intervention.
Results: The median (interquartile range) age of boys and girls was 15 (12-16) years both at baseline and end line. There was a 3.97 unit and 4.70 unit increase in the self-efficacy score at the end line compared to the baseline (p<0.001) after adjusting for age, education, community, and monthly family income among boys and girls, respectively. Moreover, the dose-response analysis showed an increment in iron folic acid tablet consumption with an increasing number of sessions among boys and girls. Conclusions: The community-based interventions involving education sessions have a positive impact on improving nutritional self-efficacy and dietary practices among adolescents. Therefore, community-based interventions should be implemented on a broader scale to improve the nutritional status of adolescents.
Methods: The baseline and endline were conducted using a quantitative cross-sectional research method with boys and girls (10-19 years). Predesigned, pretested, semi-structured questionnaires were developed to capture information on socio-demographic profiles, knowledge and practices related to diets and dietary patterns, access to Anganwadicenters, WASH habits, and self-efficacy. The intervention included four group-based structured education sessions and community-based events like role plays, video shows, games-based learning, and folk dances. In total, 673 boys and girls at baseline and 793 at end line participated in the surveys. We employed linear and logistic regression analysis to estimate the degree of change in outcomes at end line compared to the baseline and dose-response analysis to estimate the effect of the intervention.
Results: The median (interquartile range) age of boys and girls was 15 (12-16) years both at baseline and end line. There was a 3.97 unit and 4.70 unit increase in the self-efficacy score at the end line compared to the baseline (p<0.001) after adjusting for age, education, community, and monthly family income among boys and girls, respectively. Moreover, the dose-response analysis showed an increment in iron folic acid tablet consumption with an increasing number of sessions among boys and girls. Conclusions: The community-based interventions involving education sessions have a positive impact on improving nutritional self-efficacy and dietary practices among adolescents. Therefore, community-based interventions should be implemented on a broader scale to improve the nutritional status of adolescents.
Keywords: Diet; Self-efficacy; Vegetables; Fruit; Iron; Adolescent
Abbreviations
FFQ: Food Frequency Questionnaire; WASH: Water, Sanitation
and Hygiene; IFA: Iron-Folic Acid; GLV= Green Leafy Vegetables;
UK: United Kingdom; USA: United States of America
Introduction
The World Health Organization defines an adolescent as 10-19
years of age, bridging the gap between childhood and adulthood.
[1,2] The transition phase involves rapid physical, cognitive, and
psychosocial growth and development.[2]Adolescents are recognized
as a significant asset at the family, societal, and national level and can
be considered as the second window of opportunity for nurturing
before adulthood.[2,3]
Globally, at present, 1.3 billion adolescents exist, constituting 16%
of the world’s population.[4]India is home to 253 million adolescents,
accounting for the largest adolescent population in the world.[5]
However, adolescent health and nutrition are major concerns all over
the world, especially in low- and middle-income countries.[6]A high
prevalence of under nutrition among adolescents has been observed
in South Asia, with an increasing burden of overweight and obesity.
[7] The burden of stunting and thinness among adolescents was 27.4%
and 24.4%, respectively. In contrast, the rates of overweight and obesity
were 4.8% and 1.1%, respectively[8]. Micronutrient deficiencies are
also prevalent among adolescents; 16-37% of adolescents had different
types of micronutrient deficiencies, such as Vitamin A, Vitamin D,
zinc, Vitamin B12, and folate.[9]In developing nations, adolescents
tend to have a restricted dietary variety, primarily relying on plant based
foods. However, their consumption of fruits and vegetables is
limited. Concurrently, there is a noticeable rise in the consumption
of high-calorie snacks and beverages, especially in urban regions.[10]
The uneven distribution of under nutrition and micronutrient
deficiencies varies based on geographical locations, ethnic groups,
genders, religious affiliations, and other socio-demographic
characteristics.[11] Evidence suggests that the socio-demographic
elements of adolescents are associated with malnutrition, such as
gender, religion, wealth index, and educational qualifications.[12]
For instance, adolescents with senior secondary grades or above had
lower odds of having low-mixed diets as compared to illiterate or had
obtained education up to primary or middle grades. Furthermore,
adolescents from marginalized communities were identified as
significant predictors of having low-diversity diets.[12,13]
As per the findings of the Comprehensive National Nutrition
Survey (2016-18), the majority (55.4%) of the adolescents followed a
vegetarian diet pattern, while more than one-third (36.4%) preferred a
non-vegetarian, and the rest were eggetarian.[9] A significant variation
in the dietary habits of adolescents (10-19 years) was observed across
various states in India. Notably, the consumption of milk and milk
products and fruits was less frequent among adolescents (10-19 years)
in Odisha; however, the majority (90.9%) included pulses or beans and
green leafy vegetables (88.9%) in their diet, followed by eggs (64.6%),
fish (58.1%), and chicken or meat (44.5%).[9] Research indicates that
diets in India primarily revolve around cereals and lack sufficient
inclusion of other essential nutritional components.[14] However, the
studies assessing dietary patterns among adolescents are limited.[15]
Existing evidence highlights unhealthy dietary habits among
adolescents in various Indian settings.[16] Adolescents often
consume unhealthy foods due to a lack of knowledge and awareness
about the associated health risks. Furthermore, gender plays a
significant role in the dietary behaviour of adolescents.[16] Indian
studies have reported a strong association between unhealthy eating
habits and peer influence, taste preferences, place of residence, gender,
and persuasive advertising.[16] For example, the consumption of
green leafy vegetables was far lower than that of unhealthy food
among adolescent boys and girls in Odisha.[16]On the contrary, the
consumption of green leafy vegetables was found to be excess in their
diet among the tribal women of Odisha.[18]
Research revealed that the studies implemented multi-faceted
intervention strategies to increase fruit and vegetable access or
consumption[17] An example of a multiple-intervention strategy is
an educational series delivered primarily in schools, supplemented
by a homework component to actively involve parents. Additional
interventions include nutrition programs, group discussions, health
education, peer-led approaches, and community gardens, among
others. Notably, only 10% of the interventions focused on individual
strategies aimed at increasing fruit and vegetable consumption.[17]
Furthermore, self-efficacy is considered necessary for behaviour
modification as well as the preservation of recently adopted
behaviours. Evidence reported a statistically significant correlation
between self-efficacy and perceived barriers towards healthy eating
habits among adolescents in Port Said city.[19]
Evaluating the eating habits of a population requires using
approaches, and among these, Food Frequency Questionnaires (FFQs)
are frequently used to assess nutrient intake in population-based
studies. This method is relatively inexpensive and puts less burden on
the respondents. However, maintaining accuracy and consistency in
measuring patterns continues to be a challenge.[20]
Considering the need, MAMTA designed a two-year intervention
on health and nutrition education promotion among adolescent boys
and girls in two districts of Odisha. The baseline study was conducted
to assess the baseline status of the intervention indicators. Then, after
two years of intervention, the end line was conducted to assess the
improvement in the indicators. The present study assessed the change
in the health and nutrition practices of adolescents’ post-intervention
residing in the Bolangir and Nuapada districts of Odisha.
Methods
Study design, study population, and study settings: A
quantitative cross-sectional research was conducted in four
intervention blocks of two districts of Odisha at the beginning and at
the end of the intervention. These study sites (Bolangir and Nuapada)
were included as they were a part of the intervention. The study
was conducted among adolescent boys and girls (10-19 years) who
were unmarried and residing in the areas for the past 1 year. All the
individuals who did not provide consent or assents (for adolescents)
to participate in the study or suffered a major illness in the past 1
year or migrated were excluded. The baseline study was conducted
in 2020 and end line in 2022. The sample size for two districts was
reported to be a minimum of 240 each for adolescent girls and boys,
respectively, both at the baseline and end line. The sample size was
equally distributed across the districts and divided equally between
early and late adolescents.
The sample size was calculated using the below-mentioned formula:

Where, n = required sample size
P1= Pre-study estimate of the proportional change in the
combined health, nutritional, and hygiene indicator value (calculated
from the previous project for each category of beneficiary)
P2= Post-study estimate of the proportional change in
the combined health, nutritional, and hygiene indicator value
(assumption)
P3= (p1+p2)/2; D= P1-P2; t = confidence level at 95% (standard
value of 1.96)
Zcrit = 1.96; standard normal deviate corresponding to 95% significant criteria
Zpwr = 0.842; standard normal deviate corresponding to 80% statistical power
Zcrit = 1.96; standard normal deviate corresponding to 95% significant criteria
Zpwr = 0.842; standard normal deviate corresponding to 80% statistical power
After adjusting for the design effect (1.2) and a non-response rate
(10%), the sample size per beneficiary turned out to be 240. A twostage
sampling technique was used for quantitative data collection of
the subjects in four intervention blocks of the two districts. Villages
were considered as the primary sampling units (PSUs) and households
as the secondary sampling units (SSUs) in a two-stage sampling
technique. Twelve villages in each block were selected for the study.
The adolescents at the baseline and end line were different as it was
not a panel study (or pre-post study).
Study tools:
A predesigned, pretested, semi-structured questionnaire was
developed to capture information on socio-demographic profiles
along with their knowledge and practices related to the diets and
dietary patterns of the subjects. The questionnaire was originally
formed in English and then translated into the local language (Odiya).
Same questionnaires were employed both at the baseline and end line,
except for a few additional about the intervention at the end line.
The questionnaire had four sections, including socio-demographic
characteristics, access to Anganwadi centers, WASH habits, and
dietary practices. WASH habits were accessed by asking questions like
place of defecation, washing hands after defecation, handling pets,
handling animal wastes, etc. In the dietary practices, we asked about
the frequency of the consumption of seven food groups, including
green leafy vegetables, fruits, roots and tubers, other vegetables, milk
and milk products, cereals, and pulses (lentils). There were eleven
options for food frequency, ranging from once a day, twice a day,
thrice a day to once a week, fortnightly, occasionally, and never. The
daily consumption of the food groups was calculated by replacing the
frequency with the appropriate number, such as, for those consuming
once a week, the daily consumption was 0.14. Similarly, the daily
consumption of those eating 2-3 times a week was 0.35, fortnightly
was 0.07, monthly was 0.03, quarterly was 0.01, and occasionally or
never was 0.We also asked about the self-efficacy of adolescents related to
resisting the consumption of foods rich in calories and planning a
healthy diet using a pretested questionnaire. There were five questions
based on a seven-point Likert scale, with responses varying from not
at all confident (scored 0) to very confident (scored 7). The individual
scores of all five questions were summed up to calculate the aggregate
score, the max and min values of which were 0 and 35. The scale had
been validated earlier (20). At the end line, we asked if the adolescents
attended sessions or events in the program as well as the rating for
different components of the program. The rating was based on a
three-point Likert scale with responses varying from agrees to neutral
to disagree.
Furthermore, a team of data investigators were trained for
two days on the data collection techniques and carried out mock
surveys under the supervision of the district coordinator and field
supervisors before initiating the survey. Continuous supervision and
random monitoring were also conducted by the field team and the
head office team during data collection. All the questionnaires were
developed into an Android-based mobile application using Open
Data Kit (ODK). About 5% of the filled performs were screened for
the completeness, consistency, and coherence of the data. The data
collection during the baseline and end line study was conducted for
over 2-3 months.
Intervention:
It was a 2-year community-based intervention aimed at
improving knowledge, attitude, and practices related to nutrition,
health, and hygiene among adolescents across two districts of Odisha,
namely Bolangir and Nuapada. The intervention included four group based
structured education sessions and community-based events
like role plays, video shows, games-based learning, and folk dances.
The intervention was delivered by the project staff with a minimum
education of bachelor’s and trained on the topics to be delivered. The
structured education sessions were delivered using a flipbook and
posters in a group of 20-25 adolescents, separately for boys and girls.
The attendance of the sessions was obtained by the staff and maintained
in the online management information system. Adolescents and their
parents were invited to the community events held regularly over a
period of two years. Pamphlets were also distributed towards the end
of the events or sessions for self-reading. The content of the flipbooks,
posters, sessions, events, and pamphlets was in the local language
(Odiya).Ethical clearance:
The ethical clearance of the study was obtained from the MAMTA
Internal Ethical Review Board for the project. Informed written
consent was obtained from all study subjects ≥18 years, while assent
was obtained from subjects <18 years and informed consent from
their parents. No pressure or coercion was exerted on subjects for
participation in the study. Moreover, the information obtained from
the subjects was kept confidential to avoid risks associated with the
disclosure of sensitive information.Statistics:
The data were presented as percentages and frequencies or mean
(Standard Deviation, SD) and median (Interquartile Range). We
employed linear regression analysis to find an association for three
of the four outcomes, including daily consumption of green leafy
vegetables, fruits, and self-efficacy scores, and logistic regression to
find an association for the fourth outcome, i.e., the consumption of
iron folic acid tablets. The independent variables included baseline or
end line status, age, monthly family income, community, religion, and
education status of the adolescents. All the outcomes were normally
distributed. In addition, we analyzed the dose-response association
between the number of sessions attended by the adolescent and the
consumption of iron folic acid (IFA) tablets without adjustment for
any other factor (only based on the end line data). The effect size
was expressed as a beta coefficient (95% Confidence Interval; CI) for
general linear regression and odds ratio (OR) (95% CI) for logistic
regression. All the analyses were done separately for boys and girls.
We used STATA version 17.0 for all the analysis. P-value <0.05 was
considered a statistically significant value in all the analyses.Results
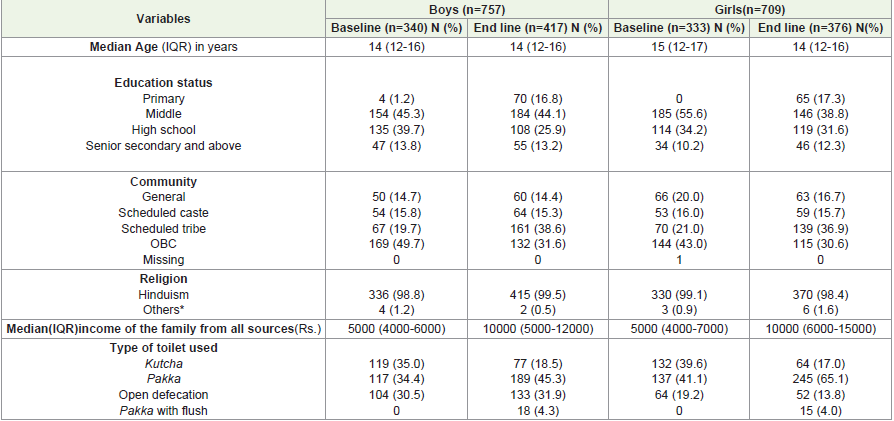
There were 4 blocks and 51 villages in total where surveys were
done. The median age of boys and girls was similar both at the end
line and baseline. Most of the adolescents had studied until the
middle school at the time of the surveys. Around 86% of adolescents
at baseline and 80-85% at the end line belonged to marginalized
families. The predominant religion among the families was Hinduism,
comprising 98.8% of the population. Around 14% of girls defecated in
the open compared to 19% at the baseline as shown in [Table 1].
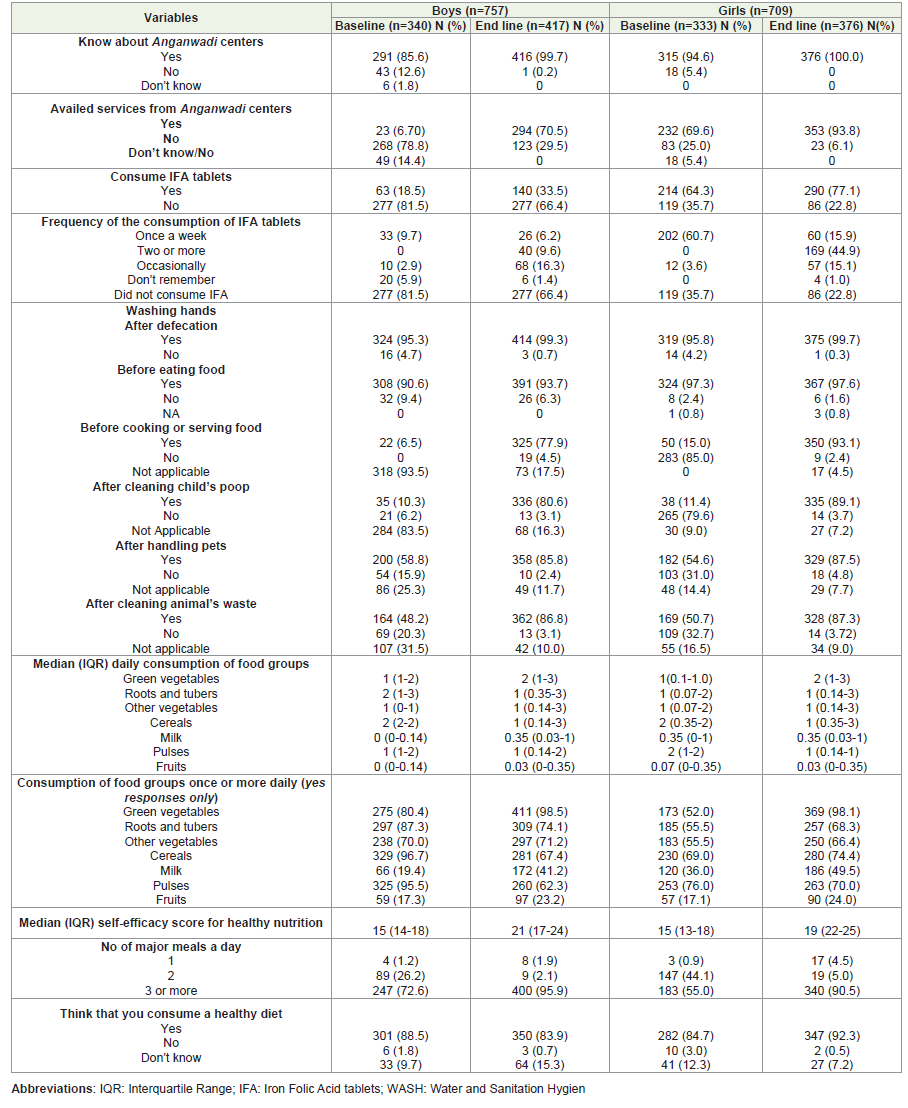
Almost all of the adolescent boys and girls knew about anganwadi
centres. It is interesting to note that there was 63.8% increase among
boys and 24.2% increase among girls in availing services among
anganwadi centres. There was a 15% increase among boys and 13%
among girls consuming IFA tablets. Though the consumption of green
leafy vegetables increased by 18% from baseline to the end line, the
consumption of fruits increased by a mere 5% among boys. Similarly,
the consumption of green leafy vegetables increased by 46% from
baseline to the end line and the consumption of fruits increased by
a mere 7% among girls. More than 90% of the adolescents reported
to be consuming 3 or more meals in a day during end line as shown
in [Table 2].
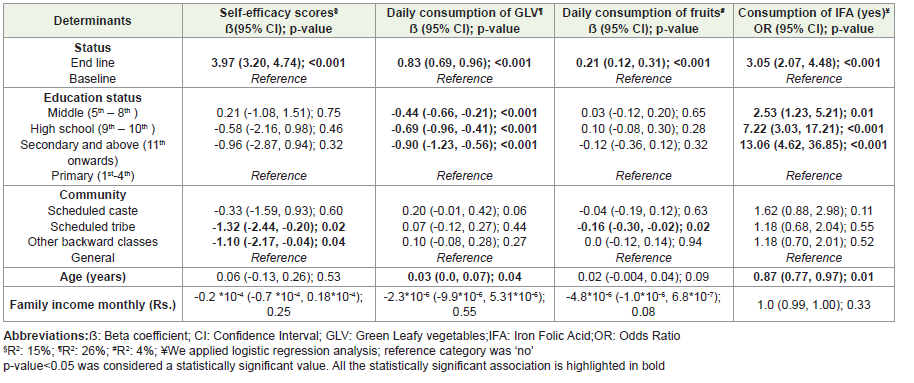
There was a 3.97-unit increase in the self-efficacy score at the
end line compared to the baseline (p<0.001) after adjusting for age,
education, community, and monthly family income. Similarly, the
increase was noted for the daily consumption of green leafy vegetables
and fruits among boys (p<0.001). There were three times the odds of
consuming IFA at the end line compared to the baseline (OR, 95%CI:
3.05, 2.07-4.48). The adolescent boys with higher grades of education
reported an increased daily consumption of green leafy vegetables and
IFA tablets as compared to their counterparts as shown in [Table 3].
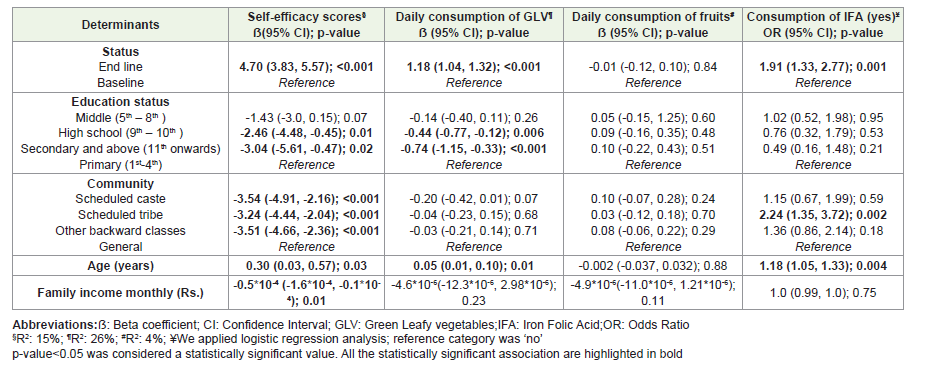
Like boys, girls had 1.91 times the odds of consuming IFA at the
end line compared to the baseline (p=0.001). There was a 4.7-unit
increase in the self-efficacy scores and a 1.18 unit increase in the daily
consumption of green leafy vegetables at the end line among girls
(p<0.001). However, no statistically significant difference was noted at
the end line in the consumption of fruits among girls. The self-efficacy
score was observed to be higher among adolescent girls belonging to
the marginalized communities in comparison to their counterparts.
Age emerged as a significant determinant influencing the self-efficacy
score, as well as the daily consumption of green leafy vegetables and
IFA tablets among girls as shown in [Table 4].
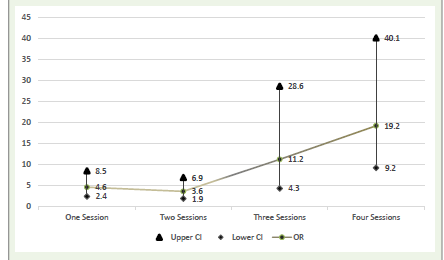
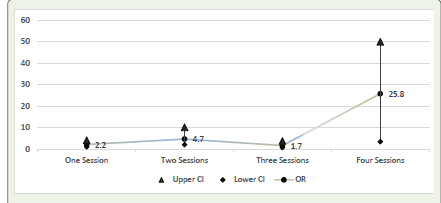
Out of 417 boys, 208 attended any session, and out of 376 girls,
241 attended any session. A dose-response association was noted in
the number of sessions and the odds of consuming IFA among boys
and girls [Figure 1] and [Figure 2]. There were 25 times the odds of
consuming IFA among girls who attended 4 sessions compared to 2.2
times the odds of consuming IFA among girls who attended 1 session
without any adjustment for covariates or confounders. More than
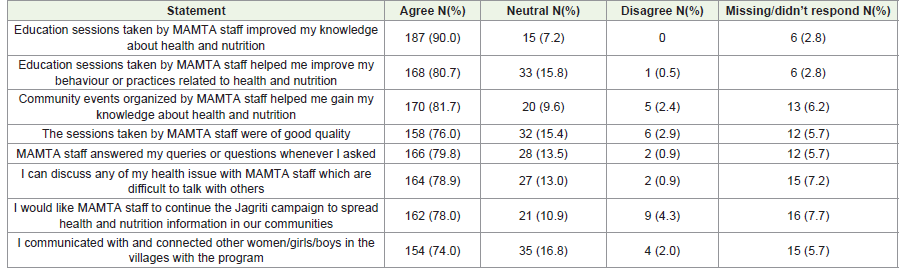
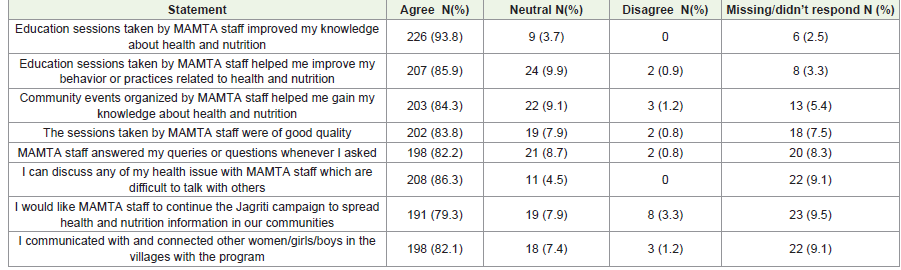
3/4th of the adolescent girls and boys agreed that the sessions taken by
the staff helped them improve their nutritional knowledge and change
their behaviour, and they could share their issues with them as shown
in [Table 5,6].
Discussion
We found that our community-based intervention was effective
in improving the consumption of IFA tablets among girls and boys.
Besides, an improvement in the median daily consumption of green
leafy vegetables and fruits, self-efficacy towards eating healthy foods,
and perception about eating healthy food was noted from baseline
to the end line. We noted an improvement in the hand wash habits
before cooking or serving food at the end line from the baseline.
The dose-response analysis showed an increment in the IFA tablet
consumption with an increasing number of sessions. The boys and
girls who participated in MAMTA’s education sessions gave good
feedback on the quality of sessions and events.
Our findings agree with the results of a systematic review that
evaluated community-based interventions aiming to improve the
accessibility to or intake of fruits and vegetables among children and
adolescents aged 5-18 years and their parents. The review primarily
encompassed studies conducted in the UK, USA, and Finland.
[22] Diverse methodologies were employed, including healthrelated
education programs targeting increased fruit and vegetable
consumption, the establishment of kitchen gardens, and utilization
of the internet, telephone, and media across multiple settings such as
schools, communities, homes, and online platforms[22]. The studies
conducted in Uttar Pradesh, West Delhi, Nagpur, and Chandigarh
used similar approaches as ours to improve the self-efficacy among
adolescents.[23]
In our intervention, self-efficacy emerged as a crucial outcome.
This is noteworthy as previous studies have indicated that, in addition
to nutrition knowledge and preferences, self-efficacy is linked to
an increased consumption of fruits and vegetables.[22] In India,
schools have been a common location for conducting interventions
among adolescents using audio-visual aids, print media, and
educational sessions to significantly enhance both knowledge and the
consumption of fruits and vegetables.[24,25] This is in concordance
with our findings at the community level. We found a statistically
significant difference (p<0.001) in the self-efficacy scores and the
daily consumption of green leafy vegetables among adolescents in
our study. One of the plausible explanations for an increase in the
consumption of green leafy vegetables among adolescents could be
seasonal availability, particularly since the end line was conducted in
winter (December, 2022). However, we did not find any dose-response
association between the number of sessions and the consumption of
fruits and vegetables among adolescents.
Furthermore, findings of the previous studies suggest that
adolescent’s age, family income, education status, and gender are
correlated with the intake of fruits and vegetables.[26,27]Consistent
with these findings, our study also observed similar associations.
The purpose of our community-based interventions was to improve
the existing knowledge and dietary practices of adolescents. After
adjusting the socio-demographic determinants, we found that
adolescents with higher grades of education (p<0.001) had an
increased consumption of green leafy vegetables. Contrarily, we did
not find any significant association between social class and the daily
consumption of fruits and vegetables among adolescents, except for
adolescent boys belonging to the scheduled tribe, who exhibited
decreased daily consumption of fruits compared to the general
category. This is in concordance with the previous research indicating
a concerning trend in the consumption of fruits within the Indian
population, with lower castes demonstrating significantly lower
intake of fruits and vegetables compared to upper castes.[27]
Our intervention also centered on educating adolescents on
anaemia identification, prevention, and management through
various community-based interventions. Notably, we found a
significant increase in the consumption of iron-folic acid tablets from
baseline to end line among adolescents. Various community-based
interventions such as educational programs using audio-visual aids,
IFA supplementation through trained peer educators along with
nutritional education, community-based meetings, audio messages,
and automated phone calls were conducted to educate adolescents to
increase the consumption of IFA tablets.[28-31] The duration of the
intervention period varied from 3 months to 12 months.[28-31]
Implementations such as the consumption of IFA tablets, nutrition
education, and deworming tablets every 6 months had significantly
improved anaemia status among adolescents (10-19 years) in Uttar
Pradesh.[31] The study highlighted that counseling sessions on the
positive effect of IFA intake contributed to a high compliance rate of
over 85%.[31] Furthermore, a study conducted in Telangna showed
that nutrition education has significantly increased the knowledge,
attitude, and practice scores among adolescent girls (13-17 years).[28]
To the best of our knowledge, there is limited evidence on community based
interventions to increase IFA consumption among adolescents
in India. A school-based study conducted in Karnataka involving
adolescents aged 11-14 years revealed that educational sessions
not only enhanced knowledge and attitudes but also increased the
demand for IFA tablets.[32] Similar findings were also observed in
our study that attending education sessions significantly increased
the consumption of IFA tablets among adolescents. Moreover, the
frequency of consumption of IFA tablets has also increased from
baseline to end line.
Furthermore, the reasons could be attributed to higher education,
which is associated with an increase in self-efficacy. Linear and
logistic regression analysis adjusted for potential socio-demographic
determinants found a statistically significant correlation (p<0.001)
between higher grades of education among boys and increased
consumption of IFA tablets in our study. On the contrary, we did not
find any significant impact of the education status on the consumption
of IFA tablets among girls.
One of the major strengths of our study was the use of educational
materials along with engaging activities as well as the involvement
and support of local stakeholders for organizing the activities at
the community level. Strength was having field staff from the local
communities who could effectively communicate and deliver
interventions in the communities. The present study should be seen
in the light of some limitations. The COVID-19 pandemic had a
differential impact on our intervention; due to lockdown and mobility
restrictions in the early stages of COVID-19, there were delays in
sessions. In addition, the adolescents were hesitant to attend sessions,
so convincing and encouraging them was one of the challenges. The
geography of the intervention districts was quite scattered and hard to
reach as well. Therefore, to sustainably improve knowledge and dietary
patterns and improve engagement of adolescents in our sessions, we
approached their parents, frontline workers, and school teachers.
Lastly, we limited our outcome indicators to the consumption of fruits
and vegetables and IFA consumption because of time and resource
constraints. Studies have looked at the influence of intermittent
iron and folic acid supplementation on cognitive abilities among
adolescent girls.[33]
We conclude that community-based interventions involving
education sessions have a positive impact on improving nutritional
self-efficacy and dietary practices among adolescents. Therefore,
implementing community-based interventions on a broader scale
holds the potential to enhance the nutritional status of adolescents.
However, to our knowledge, there is limited evidence on communitybased
interventions among adolescent boys and girls in India.
Hence, we need to do post-hoc evaluations to prove the effectiveness
of many community-based interventions implemented by other
civil society organizations. Engaging communities in the design
and implementation of interventions promotes health, addresses
nutritional deficiencies, and establishes healthy behaviours to ensure
sustainability.
Acknowledgements
We want to extend our thanks to field staff who executed the
intervention and our beneficiaries who participated in the sessions
and events.
References
Citation
Priyanshu R, Santosh C, Rohit P, Sunil M, Shantanu S. Evaluation of a Community-Based Intervention to Improve Dietary Patterns and Nutritional Self-Efficacy among Adolescents in Two Districts of Odisha. Indian J Nutri. 2024;11(1): 282.