Research Article
Effects of an Additional Chicken Egg in the Octogenarian Persons: Malnutrition and Hypoalbuminemia Probably Due to Chronic Liver Damage
Sanai T1,2*, Sasaki H1, Eto T1, Nakaishi K1, Tamura T1 and Fukamizu N1
1Department of Internal Medicine, Mitsumi Long-term Care Heath Facility, 5-8-55 Saitozaki, Higashi-ku, Fukuoka-City, 811-0321
Fukuoka, Japan
2Department of Hemodialysis Center, Fukumitsu Clinic, 4-10-1 Kashiihama, Higashi-ku, Fukuoka-City, 813-0016 Fukuoka, Japan
*Corresponding author: Sanai T, Department of Internal Medicine, Mitsumi Long-term Care Heath Facility, 5-8-55 Saitozaki,
Higashi-ku, Fukuoka-City, 811-0321 Fukuoka, Japan; Tel: +81-92-603-6321. Fax: +81-92-603-6000; E-mail: sunny@
fukumitsuclinic.jp
Article Information: Submission: 03/03/2023; Accepted: 10/04/2023; Published: 14/04/2023
Copyright: © 2023 Sanai T, et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background & Objective: Hypoalbuminemia has become important with regard to mortality in the elderly people. Two - three / day additional chicken
egg (CE) are usually added to meal and is a potentially effective therapy for treating malnutrition in the elderly people.
Methods: Hypoalbuminemia (the serum albumin (Alb) < 3.1 g/dL) was observed in the eight (age: 88.6±4.2 [mean±standard deviation]) of 79 octogenarian
persons. The present study evaluates the efficacy of a/day additional CE was added in the improvement of the nutritional indices of people. We examined the
nutritional indices, anemia, renal and hepatic function, and muscle anthropometry markers for 6 weeks with a/day additional CE in comparison with the thirteen
ambulatory patients on chronic kidney disease (CKD) glomerular filtration rate (G) 2-4 used as a control.
Results: Although the serum total protein (TP) were not significantly different, the Alb were significantly lower in the octogenarian CE persons vs in the
CKD patients (before: 2.9±0.4g/dL vs 4.2±0.3g/dL, p<0.05, 6 weeks: 3.0±0.4g/dL, p<0.05). The Alb / (TP–Alb) (A/G) were significantly more decreased (before:
0.76±0.11 vs 1.44±0.24, p<0.05, 6 weeks: 0.73±0.11, p<0.05). The aspartate aminotransferase (AST) / alanine aminotransferase (ALT) were significantly more
increased in the CE vs the CKD groups (before: 1.78±0.37 vs 1.43±0.38, not significant [ns], 6 weeks after treatment: 1.83±0.44, p<0.05). The fatty mass were
significantly more increased (triceps skin-fold thickness [TSF]; before: 6.9±2.2mm vs 5.0±3.0 mm, ns, 6 weeks: 8.5±4.1mm, p<0.05).
Conclusion: A / day additional CE was added to meal and an ineffective therapy for treating malnutrition in the octogenarian persons which might have
the decrease of serum Alb and A / G, the elevation of AST / ALT, and the normal levels of TP probably due to chronic liver damage. In addition, the increase of
TSF may assess fatty mass in the octogenarian persons.
Keywords
Aspartate aminotransferase (AST) / alanine aminotransferase (ALT); Chicken egg; Chronic liver damage; Chronic kidney disease (CKD);
Hypoalbuminemia; Serum total protein; Triceps skin-fold thickness (TSF)
Introduction
The progression of cardiovascular disease, infection, and
the cerebrovascular disease remains a major clinical concern in the
hemodialysis is elderly patients [1]. Additionally, the incidence
of malnutrition, especially hypoalbuminemia is also frequently
encountered in the octogenarian persons.
Malnutrition (the low serum albumin [Alb], a decline in protein intake and fat masses), muscle wasting, cachexia, and inflammation
in chronic kidney disease (CKD) have been paid attention. The
International Society of Renal Nutrition and Metabolism has
proposed a new term protein - energy wasting (PEW) [2]. The concept
of “PEW” refers to the multiple nutritional and catabolic alterations
that occurred in the patients with CKD and associated with mortality.
Two - three / day additional chicken egg (CE) are usually added to
meal and is a potentially effective therapy for treating malnutrition in elderly people [3]. However, the serum cholesterol (Chol) levels
may be high in such people with two - three / day additional CE.
Furthermore, a / day additional CE may be added to meal in
the octogenarian persons. The effect of nutritional supplementation
with a / day additional CE have a beneficial effect on the serum total
protein (TP), Alb, Chol, aspartate aminotransferase (AST), alanine
aminotransferase (ALT) levels, arm circumference (AC), triceps
skin - fold thickness (TSF), and saturation of percutaneous oxygen
(SpO2) in the octogenarian CE persons in comparison with the CKD
ambulatory patients.
Methods
Patients:
A total of 79 octogenarian persons (the serum Alb levels: 3.5±0.5
[standard deviation (SD)] [2.6 - 4.3] mg/dL) at the Mitsumi Long -
term Care Heath Facility were examined. The effect of a additional
CE / day in the remaining eight octogenarian persons (10.1%, 2 case
male, 6 case female; mean age: 88.6 ± 4.2 years; age range: 84 - 96
years; stage glomerular filtration rate (G) 2 - 4 : G2: 1 case, G3: 5 cases,
G4: 2 cases; the CE group) with the presence of hypoalbuminemia
(the serum Alb levels < 3.1 mg/dL: 2.9±0.4 [2.6 - 3.0] mg/dL) and
the low geriatric nutritional risk index (GNRI) levels were performed,
however, all of 79 octogenarian persons were added and get nourished
by a / day additional CE (Figure 1).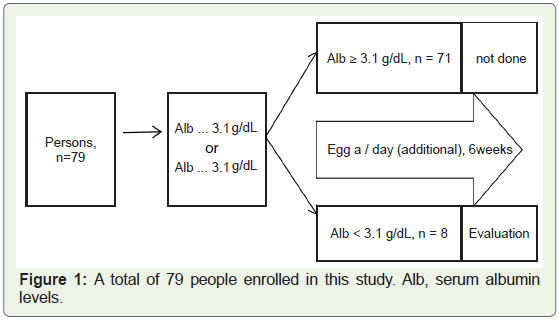
The thirteen ambulatory patients with stage G2 - 4 (G2: 5 cases,
G3: 7 cases, G4: 1 case) at the Fukumitsu Clinic (68.0±13.6 years;
aged range: 41 - 93 years, 3 cases male, 10 cases female; the serum Alb
levels: 4.2±0.3 [3.6 – 4.6] mg/dL; the CKD group) were included. The
G5 patients were excluded, because the serum AST and ALT levels are
very low in the G5, especially G5 (Dialysis) patients [4,5]. The thirteen
ambulatory CKD patients were used as a control except for age, body
weight (BW), and the serum Alb levels.
The serum Alb levels has a half - life of 21 days. A / day additional
CE in octogenarian persons with hypoalbuminemia was performed
for a period of 6 weeks between the overall study period of September
16, 2021 and October 28, 2021 (Figure 1). The serum nutritional
indices, renal and hepatic functional markers, and the presence of
anemia were assessed in these persons at the baseline characteristics
(the CE and CKD groups) and the 6 weeks after treatment (the CE
group) performed at the SRL Co. Ltd. (Fukuoka, Japan).
The present study was performed using a non - randomized
analysis with a prospective and controlled design. The study
procedures were carried out in accordance with the ethical standards
of the Human Investigation Committee at the Mitsumi Long - term
Care Heath Facility and the Fukumitsu Clinic (Fukumitsu Clinic No.
1 - 2023). All patients gave their written informed consent.
All procedures performed in the study involving human
participants were in accordance with the ethical standard of the
institutional and / or national research committee with the 1964
Helsinki declaration and its later amendments or comparable ethical
standard.
Blood Sampling, Body Mass Index (BMI), AC, TSF, Arm Mucle Circumference (AMC), Arm Muscle Area (AMA), SpO2 and GNRI:
The serum TP, Alb, Alb / TP - Alb (A / G), AST, ALT, fibrosis -
4 index (FIB - 4 index), low density lipoprotein (LDL) - Chol, high
density lipoprotein (HDL) - Chol, uric acid, corrected cacium (c -
Ca), blood urea nitrogen (BUN), creatinine (Cr), hematcrit (Ht),
hemoglobin (Hb), platelet (Plt) levels, BMI, AC, TSF, AMC, AMA,
SpO2 in evening or morning, and GNRI levels were measured in
the non - fasted blood samples drawn immediately before and the 6
weeks after treatment.The five indexes equation are calculated using the following
equation:
BMI (kg / m2) = BW (kg) / (Height [m])2
A/G = Alb (g/dL) / (TP [g/dL] – Alb [g/dL])
FIB-4 index = Age × AST (IU/L) / (Plt [104/μL] × √ALT [IU/L]
AMC (cm) = AC (cm) - π TSF (mm) / 10
AMA (cm2) = (AMC [cm])2 / 4π
The GNRI levels were developed by modifying the nutritional risk
index for elderly people [6]. This index is calculated from the serum
Alb levels and BW using the following equation:
GNRI=14.89×Alb (g/dL) + 41.7×BW/ideal body weight (IBW)
BW / IBW were set to 1 when the patient’s BW exceeded the IBW.
The IBW in the present study was defined as the value calculated from
the height and a body mass index of 22, because of its validity [7].
Statistical Analysis:
The data are expressed as mean±standard deviation. Statistical
differences were computed using the unpaired t test. A p value of <
0.05 was considered statistically significant.Results
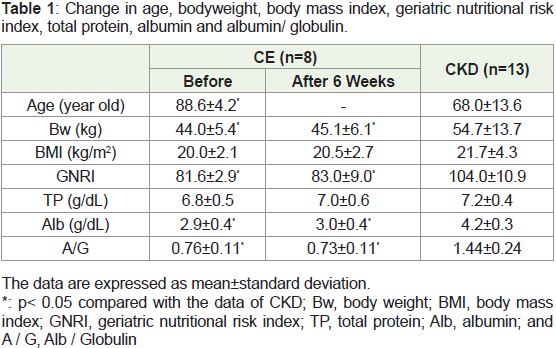
In shown as Table 1, the BW were significantly altered by CE
treatment and the BMI was lower upon treatment with CE (before:
20.0±2.1 kg/m2 vs 21.7±4.3 kg/m2, not significant [ns], and the 6 weeks
after treatment: 20.5±2.7 kg/m2, ns). The GNRI was significantly
lower upon treatment with CE (before: 81.6±2.9 vs 104.0±10.9 g/dL,
p<0.05 and the 6 weeks after treatment: 83.0±9.0, p<0.05).
The serum TP levels were not significantly different in the CE vs
the CKD groups (before: TP; 6.8±0.5 g/dL vs 7.2±0.4 g/dL, ns, and the 6 weeks after treatment: TP; 7.0±0.6 g/dL, ns). The serum Alb levels
significantly more decreased in the CE group (before: 2.9±0.4 g/dL vs
4.2±0.3 g/dL, p<0.05, and the 6 weeks after treatment: 3.0±0.4 g/dL,
p<0.05). The serum A / G levels significantly more decreased in the
CE group (before: 0.76±0.11 vs 1.44±0.24, p<0.05, and the 6 weeks
after treatment: 0.73±0.11, p<0.05) (Table 1).
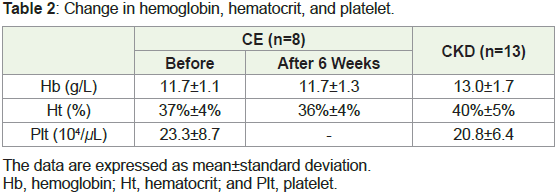
The observed increase in the Hb and Ht levels from before
treatment to the 6 weeks after treatment was not significantly different
in the CE group (Table 2). The Plt levels were not significantly
different in the CE and the CKD groups before treatment.
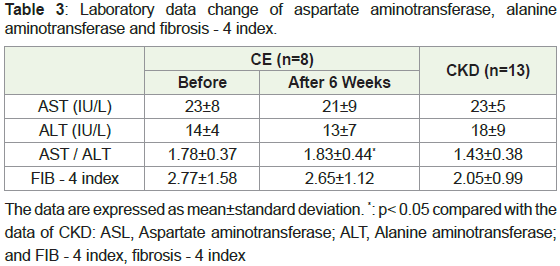
In Table 3, the serum AST, ALT levels and FIB - 4 index were not
significantly different. The serum AST / ALT ratio increased in the
CE vs the CKD groups (before: 1.78±0.37 vs 1.43±0.38, ns, and the 6
weeks after treatment: 1.83±0.44, p<0.05).
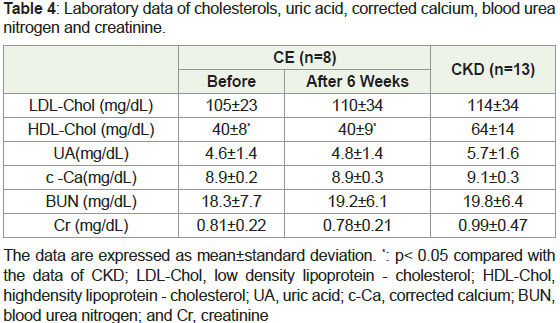
The serum uric acid, c - Ca, BUN and Cr levels were not
significantly altered by CE treatment. The observed decrease in the
LDL - Chol levels from before treatment to the 6 weeks after treatment
were not significantly different in the CE than in the CKD groups,
however, serum HDL - Chol levels from before to the 6 weeks after
treatment were significantly lower (before: 40±8 mg/dL vs 64±14
mg/dL, p<0.05, and the 6 week after treatment: 40±9 mg/dL, p<0.05)
(Table 4).
As shown Table 5, the TSF levels significantly more increased in
the CE vs the CKD groups (before: 6.9±2.2 mm vs 5.0±3.0mm, ns,
and the 6 weeks after treatment: 8.5±4.1 mm, p<0.05). The observed
decreased in the AC, AMA and AMC levels from before to the 6
weeks after treatment were not significantly different in the CE group.
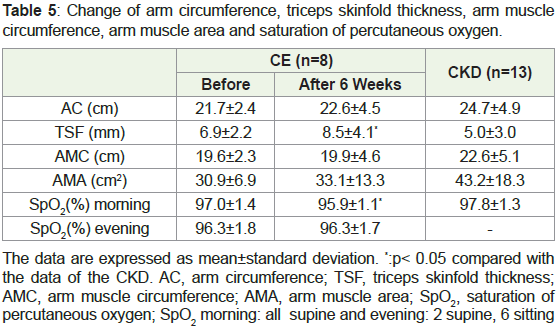
The SpO2 levels more decreased in the CE vs the CKD groups
(morning; before: 97.0±1.4% vs 97.8±1.3%, ns, and the 6 weeks after
treatment: 95.9±1.1%, p<0.05, evening; before: 96.3±1.8%, ns, and the
6 weeks after treatment: 96.3±1.7%, ns) (Table 5).
No acute adverse or chronic adverse effects associated with a /
day additional CE were observed during the treatment (6 weeks) and
follow-up period.
Discussion
The present findings clearly indicate that CE might be an effective
and well - tolerated nutritional supplement, and might improve the
serum Alb levels and GNRI in the octogenarian people. Two - three
/ day additional CE are usually added to meal and is a potentially
effective therapy for treating malnutrition in the elderly people [3].
On the other hand, this research study also demonstrates that a / day
additional CE was ineffective, especially the serum Alb levels and A /
G low, in the octogenarian CE persons.
Surveys using classic measures of nutritional status indicate
that approximately 18 - 75% of patients with CKD undergoing
maintenance hemodialysis therapy show evidence of wasting [2,8-10]. Thus, PEW (Protein-energy wasting) is the state of decreased
body stored of protein and energy fuels, and four main and established categories are recognized for the diagnosis of PEW: 1)
Serum chemistry, 2) Reduced body mass, 3) Decease in muscle mass,
and 4) Low protein or energy intake [2]. At least three out of the four
listed categories must be satisfied for the diagnosis of kidney disease
- related PEW [2]. This research study could not improve, however,
the serum Alb levels, GNRI, AC, AMA and AMC in the octogenarian
CE group.
Aspiration pneumonia was due to decreased muscle strength
of swallowing and the ratio of aspiration pneumonia patients
dramatically increased with aging [11,12]. Futhermore, the serum
Alb levels seemed to be important for the management of aspiration
pneumonia [13]. This study could not improve the serum Alb levels.
On the contrary, the data of the 6 weeks after treatment in the SpO2
(morning) was seemed to decrease in the octogenarian CE persons in
this research study (Table 5).
Various nutritional screening tools have been described in the
literature for the end – stage renal disease patients on maintenance
hemodialysis [14]. These include the serum Alb levels and geriatric
nutritional risk index developed by modifying the nutritional risk
index for elderly patients [6], the malnutrition - inflammation score
(MIS) [15], the nutritional screening tools objective score of nutrition
on dialysis (OSND) [16], the malnutrition screening tool (MST)
[17], the malnutrition universal screening tool (MUST) [18], the
nutritional screening tools nutritional risk score (NRS) [19] and the
mini nutritional assessment (MNA) [20]. This research study could
not improve the serum Alb levels and GNRI in the octogenarian CE
persons (Table 1).
This research study demands mass of skeletal muscle, function of
skeletal muscle, skeletal fatty mass [16], bone, and cardiac muscle to
assess the effect for sarcopenia baseline characteristics (the CE and
CKD groups) and the 6 weeks after treatment (the CE group). The data
of skeletal muscle areas, function, and bone (BMI, the serum AST, c
- Ca levels, AC, AMA, and AMC), and the data of cardiac muscle
(the serum AST levels) were not significantly investigated (Table 1,
Table 3-5). In contrast, the data of TSF might demand only skeletal fatty
mass at the 6 weeks after treatment in the octogenarian CE persons.
However, the observed decrease of the serum LDL - Chol levels was
not significant in the octogenarian CE persons. This clinical and
research study indicates on the assumption that the elevated AST /
ALT ratio is predictive of long terms of chronic liver disease including
the non - alcoholic fatty liver disease with the decrease levels of the
HDL - Chol levels [21].
In general, the serum Alb levels may be low and the serum TP
levels may be high or normal in liver dysfunction. Furthermore,
our findings suggested that the decrease of the serum Alb and A / G
levels, and the normal levels of the serum TP had liver dysfunction
probably due to chronic liver disease in the octogenarian CE persons.
Moreover, the serum AST / ALT ratio were significantly increased
at the 6 weeks after treatment [21] (Table 3). Consequently, we had
found chronic liver damage in the octogenarian CE persons in this
research study.
This study is associated with several potential limitations. A
limitation of the present study was the observational nature of the
study performed in a prospective and controlled design with small sample size at the Mitsumi Long-term Care Heath Facility with neither
x - ray photography nor ultrasonography. Thus, this study was an
observational study of daily clinical practice. The need for the two –
three / day additional CE may partially reflect the physiological senile
changes that are commonly found in the octogenarian individuals.
Conclusion
The administration of a / day additional CE was proved to be
an ineffective therapy for treating malnutrition in the octogenarian
CE persons. In fact, TSF mass at the 6 weeks after treatment was
significantly increased with the decrease of the serum HDL - Chol
levels. Finally, we can safely assume that chronic liver damage was
due to the decrease of the serum Alb levels and A / G, the elevation of
the serum AST / ALT ratio, and the normal levels of the serum TP in
the octogenarian CE persons in this clinical study.
Acknowledgment
We are grateful to the staff members, especially the hospital nurses
(Ms. N. Inoue, Ms. H. Nishimura, Ms. K. Satoh, and Ms. M. Ando),
the caregiver (Mr. Z. Kawashima and Mr. Y. Yoshinaga), the medical
clerks (Ms. A. Shibata, Ms. M. Sakamoto, and Ms. R. Miyazaki), and
the cooks (Mr. E. Imabayashi), at the Mitsumi Long-term Care Heath
Facility and the Fukumitsu Clinic.
References
Citation
Sanai T, Sasaki H, Eto T, Nakaishi K, Tamura T, et al. Effects of an Additional Chicken Egg in the Octogenarian Persons: Malnutrition and Hypoalbuminemia Probably Due to Chronic Liver Damage. Indian J Nutri. 2023;10(1): 274.