Case Report
Eccrine Angiomatous Hamartoma of the Ankle Since Infancy: A Recurrent Case Successfully Managed with Sclerotherapy
Shatanik Bhattacharya*
Department of Dermatology, Venereology & Leprosy, Prafulla Chandra Sen Government Medical College, Arambag, India
*Corresponding author:Dr. Shatanik Bhattacharya, Department of Dermatology, Venereology & Leprosy, Prafulla Chandra Sen Government Medical College, Arambag, India E-mail Id: shatanik.bhattacharya.97@gmail.com
Copyright: © 2026 Bhattacharya S. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 10/02/2026; Accepted: 30/03/2026; Published: 04/04/2026
Abstract
Eccrine angiomatous hamartoma is an uncommon benign cutaneous lesion composed of proliferating eccrine structures associated with vascular channels. It usually appears during infancy or childhood and most often affects distal parts of the limbs. We describe a 13-year-old boy who presented to
the dermatology clinic in March 2023 with a slowly enlarging swelling on the medial aspect of the right ankle that had been present since early childhood. The lesion measured approximately 7 × 7 cm and had become painful over the preceding two years. The patient had previously undergone surgical removal
in 2020, but the lesion reappeared within six months. Clinical examination revealed a violaceous irregular plaque extending towards the plantar surface. Histopathology demonstrated numerous eccrine coils within the dermis associated with multiple thin-walled vascular channels, consistent with eccrine
angiomatous hamartoma. Intralesional 3% polidocanol sclerotherapy was administered, resulting in marked reduction in lesion size and tenderness during follow-up.
Introduction
Eccrine angiomatous hamartoma (EAH) represents a rare benign
adnexal malformation characterized by an increased number of
eccrine glands accompanied by vascular proliferation in the dermis.
The condition was initially reported in the nineteenth century and
later defined histologically as a hamartomatous growth containing
eccrine and vascular elements.
In most reported cases, lesions are present at birth or develop during early childhood. Clinically, EAH typically manifests as a localized plaque or nodular lesion that may appear erythematous, violaceous, or skin colored. Pain and localized sweating are frequently reported because of the presence of functioning eccrine glands and vascular structures.
In most reported cases, lesions are present at birth or develop during early childhood. Clinically, EAH typically manifests as a localized plaque or nodular lesion that may appear erythematous, violaceous, or skin colored. Pain and localized sweating are frequently reported because of the presence of functioning eccrine glands and vascular structures.
The lower limbs, especially the feet and ankles, are the most
frequently affected anatomical locations. Histopathological
examination remains essential for confirmation of diagnosis, as the
clinical appearance may mimic other vascular or adnexal lesions.
Case Report
A 13-year-old male presented with swelling over the medial aspect
of the right ankle since infancy. The lesion had an insidious onset and
gradually increased in size over several years, reaching approximately
7 × 7 cm. Pain developed over the preceding two years, described as
intermittent and aggravated by prolonged standing or walking.
The patient had undergone surgical excision three years prior; however, recurrence occurred within six months. There was no history of bleeding, ulceration, or systemic symptoms.
The patient had undergone surgical excision three years prior; however, recurrence occurred within six months. There was no history of bleeding, ulceration, or systemic symptoms.
On examination, a solitary irregular reddish-violaceous plaque
was noted over the medial right ankle extending onto the plantar
surface [Figure 1]. The surface showed crusting, scaling, and
surrounding hyperpigmentation [Figure 2]. The lesion was firm,
tender, non-compressible, and non-pulsatile. No bruit was audible.
Local temperature was raised. Regional lymph nodes were palpable
but benign.
Routine laboratory investigations were within normal limits except mild elevation of ESR and CRP.
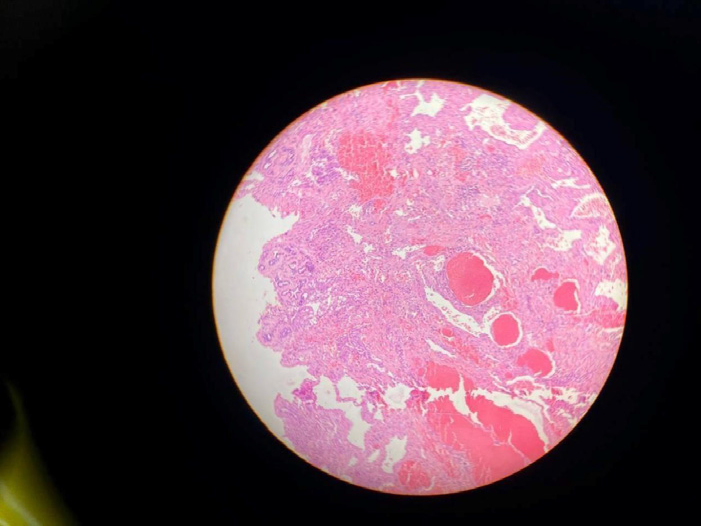
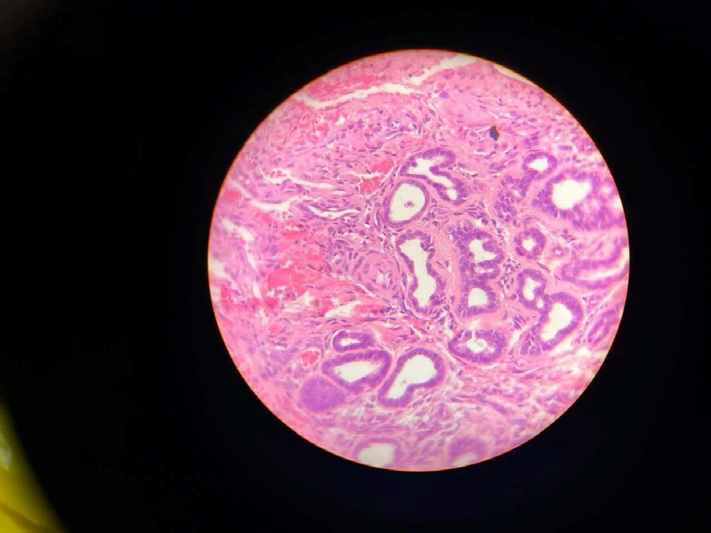
Histopathological examination revealed increased eccrine glandular structures within the dermis along with numerous thinwalled capillary-sized vascular channels embedded in fibrous stroma [Figure 3]. Higher magnification demonstrated eccrine coils intimately admixed with vascular channels without cytological atypia [Figure 4]. These findings were consistent with eccrine angiomatous hamartoma.
Routine laboratory investigations were within normal limits except mild elevation of ESR and CRP.
Histopathological examination revealed increased eccrine glandular structures within the dermis along with numerous thinwalled capillary-sized vascular channels embedded in fibrous stroma [Figure 3]. Higher magnification demonstrated eccrine coils intimately admixed with vascular channels without cytological atypia [Figure 4]. These findings were consistent with eccrine angiomatous hamartoma.


Considering prior recurrence and cosmetic concerns, intralesional
sclerotherapy with 3% polidocanol was administered weekly for
twelve sessions. Significant reduction in lesion size, tenderness, and
vascular prominence was observed. No adverse effects occurred
during follow-up.
Discussion
EAH is considered a developmental anomaly involving abnormal
induction of eccrine and vascular elements during embryogenesis. It
typically presents at birth or during early childhood, although delayed
presentation has been reported.
Pain in EAH may be attributed to vascular congestion or involvement of small nerve fibers. Hyperhidrosis occurs due to proliferation and functional activity of eccrine structures. Clinically, lesions may vary from asymptomatic plaques to painful nodules with sweating.
The differential diagnosis includes tufted angioma, arteriovenous malformation, glomus tumor, and adnexal tumors. Clinical features alone are often insufficient, making histopathological confirmation essential.
Surgical excision remains the conventional treatment and is usually curative. However, recurrence may occur, especially in incompletely excised or large lesions. Alternative modalities include laser therapy, botulinum toxin injections, and sclerotherapy. In the present case, recurrence following surgical excision highlights the limitations of surgery in extensive lesions. Intralesional polidocanol sclerotherapy resulted in marked clinical improvement without complications, supporting its role as a minimally invasive and effective treatment option.
Pain in EAH may be attributed to vascular congestion or involvement of small nerve fibers. Hyperhidrosis occurs due to proliferation and functional activity of eccrine structures. Clinically, lesions may vary from asymptomatic plaques to painful nodules with sweating.
The differential diagnosis includes tufted angioma, arteriovenous malformation, glomus tumor, and adnexal tumors. Clinical features alone are often insufficient, making histopathological confirmation essential.
Surgical excision remains the conventional treatment and is usually curative. However, recurrence may occur, especially in incompletely excised or large lesions. Alternative modalities include laser therapy, botulinum toxin injections, and sclerotherapy. In the present case, recurrence following surgical excision highlights the limitations of surgery in extensive lesions. Intralesional polidocanol sclerotherapy resulted in marked clinical improvement without complications, supporting its role as a minimally invasive and effective treatment option.
Conclusion
Eccrine angiomatous hamartoma should be considered in
congenital or early-onset vascular-appearing plaques associated with
pain or hyperhidrosis. Histopathological examination is essential for
diagnosis. This case emphasizes the possibility of recurrence after
surgical excision and demonstrates that sclerotherapy can be an
effective and safe alternative in recurrent or cosmetically sensitive
cases.
References
Citation
Bhattacharya S. Eccrine Angiomatous Hamartoma of the Ankle Since Infancy: A Recurrent Case Successfully Managed with Sclerotherapy. Indian J Dermatol Res. 2026;4(1): 107.