Research Article
Expert Opinion on the Prescription Practice of Statins in Lipid Management with a Specific Focus on Rosuvastatin Use in Indian Settings
Manjula S*and Krishna Kumar M
Department of Medical Services, Micro Labs Limited, Bangalore, Karnataka, India
*Corresponding author:Manjula S, Department of Medical Services, Micro Labs Limited, 31 Race Course Road, Bangalore, Karnataka, India- 560001 Email Id: drmanjulas@gmail.com
Copyright: ©2024 Manjula S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 16/04/2024; Accepted: 30/05/2024; Published: 07/06/2024
Abstract
Objective:The present survey-based study aims to gather the clinicians’ perspective regarding the prescription patterns of statins with a specific focus on the rosuvastatin for effective lipid management in comorbid conditions in Indian settings.
Methodology:The cross-sectional survey gathered expert opinions using a 24-item, multiple-response questionnaire related to current feedback, clinical observations, and specialists’ clinical experiences on lipid management, statins use, and prescription patterns of rosuvastatin.
Results:Fifty-three percent of clinicians noted that 20-30% of patients with dyslipidemia require combination therapy with statins. Moreover, 71% of clinicians recommended initiating statin therapy in patients with comorbidities such as diabetes or hypertension. Nearly 58% of clinicians agreed to the ACC/AHA 2019 lipid guidelines recommending the administration of the maximum tolerated dose of statins in individuals with LDL-C levels >190 mg/dl. Most clinicians recommended prescribing rosuvastatin for hyperlipidemia patients with hypertension or diabetes, and it was also the preferred statin for dyslipidemia patients. The 10 mg dosage was favored among those with diabetes, while the 20 mg dosage was recommended for patients with cardiovascular disease. Combinations of rosuvastatin and fenofibrate effectively reduced LDL/TG/hs-CRP, increased HDL, and decreased the risk of CVD. Clopidogrel was preferred to combine with rosuvastatin, and 20-30% of patients may have required this combination. The recommended duration of therapy for rosuvastatin + clopidogrel + aspirin in high CV-risk patients was 6-12 months.
Conclusion:The survey highlighted clinicians’ preferences for combination statin therapy in dyslipidemia, emphasizing early initiation in patients with diabetes or hypertension. Rosuvastatin emerged as the preferred choice, with dosages tailored to patient conditions. Additionally, respondents favored combination therapies with fenofibrate and clopidogrel, citing their additional benefits in reducing cardiovascular risk markers.
Methodology:The cross-sectional survey gathered expert opinions using a 24-item, multiple-response questionnaire related to current feedback, clinical observations, and specialists’ clinical experiences on lipid management, statins use, and prescription patterns of rosuvastatin.
Results:Fifty-three percent of clinicians noted that 20-30% of patients with dyslipidemia require combination therapy with statins. Moreover, 71% of clinicians recommended initiating statin therapy in patients with comorbidities such as diabetes or hypertension. Nearly 58% of clinicians agreed to the ACC/AHA 2019 lipid guidelines recommending the administration of the maximum tolerated dose of statins in individuals with LDL-C levels >190 mg/dl. Most clinicians recommended prescribing rosuvastatin for hyperlipidemia patients with hypertension or diabetes, and it was also the preferred statin for dyslipidemia patients. The 10 mg dosage was favored among those with diabetes, while the 20 mg dosage was recommended for patients with cardiovascular disease. Combinations of rosuvastatin and fenofibrate effectively reduced LDL/TG/hs-CRP, increased HDL, and decreased the risk of CVD. Clopidogrel was preferred to combine with rosuvastatin, and 20-30% of patients may have required this combination. The recommended duration of therapy for rosuvastatin + clopidogrel + aspirin in high CV-risk patients was 6-12 months.
Conclusion:The survey highlighted clinicians’ preferences for combination statin therapy in dyslipidemia, emphasizing early initiation in patients with diabetes or hypertension. Rosuvastatin emerged as the preferred choice, with dosages tailored to patient conditions. Additionally, respondents favored combination therapies with fenofibrate and clopidogrel, citing their additional benefits in reducing cardiovascular risk markers.
Keywords:Cardiovascular Diseases; Dyslipidemia; Hyperlipidemia; Statins; Rosuvastatin
Introduction
According to the latest special report on the Global Burden
of Disease published in the Journal of the American College of
Cardiology, the global death tolls attributable to cardiovascular
disease (CVD) surged from 12.4 million in 1990 to 19.8 million in
2022 [1].In India, CVD stands as the foremost cause of both death
and disability [2].This stark reality highlights the urgent need for
comprehensive strategies aimed at preventing and managing CVD.
CVD represents a significant contributor to both mortality and
morbidity across the Asia-Pacific region. The escalating prevalence
of CVD risk factors, including plasma lipid disorders, observed in
numerous Asian nations, is a major concern [3].
According to the World Health Organization, high cholesterol
levels contribute to approximately 4.5% of global mortality rates
and account for 2% of disability-adjusted life years (DALYs) in
individuals aged 18 and older, underscoring the profound impact
of dyslipidemia on public health [4]. Elevated serum triglyceride
(TG) levels exceeding 1000 mg/dL significantly elevate the risk of
acute pancreatitis. Globally, in 2019, the total numbers of deaths
and DALYs attributed to high low-density lipoprotein cholesterol
(LDL-C) were 1.47 and 1.41 times higher than that in 1990 [5].A
study involving 18,288 participants across four US cohorts reported
that elevated LDL-C has persisted as a leading modifiable risk
factor and is closely linked to atherosclerotic CVD. In 2021, it was
reported that 3.81 million CV deaths and 3.81 million deaths overall
were attributed to elevated LDL-C levels, with the all-cause DALYs
due to high LDL-C reaching 1,090 per 100,000. Exposure to lower
cumulative LDL-C levels in young and middle-aged adults has been
associated with reduced long-term CV risk [6].
Statins serve as the cornerstone of lipid management strategies.
These medications belong to a class of lipid-lowering drugs that
operate by inhibiting the enzyme 3-hydroxy-3-methyl-glutaryl
coenzyme A reductase, a crucial player in the key step of cholesterol
production. By targeting this enzyme, statins effectively lower levels
of total cholesterol and LDL-C, with modest effects on triglycerides.
Additionally, emerging evidence suggests that statins may exert antiinflammatory
properties and contribute to stabilizing arterial plaque
[7].Rosuvastatin is widely prescribed and recognized as one of the
most potent statins available. With rapid absorption, it achieves peak
plasma concentration within three hours of administration. The lipid lowering
efficacy of rosuvastatin remains consistent regardless of the
time of administration and this could be attributed to its relatively
long half-life, which spans approximately 20 hours. Rosuvastatin
demonstrated efficacy in reducing major vascular events across
various clinical studies [8,9].
Lipid management remains a persistent challenge, particularly
in patients with comorbid conditions, where tailored treatment
approaches are crucial. Understanding the prescription patterns
of statins is essential for optimizing patient care and improving
treatment outcomes The present survey-based study aims to gather
clinicians’ perspectives on the effectiveness of statins, with a particular
emphasis on the prescription pattern of rosuvastatin, for managing
lipids in Indian settings.
Methods
A cross sectional, questionnaire based survey was carried out
among clinicians with expertise in treating dyslipidemia in the major
Indian cities from June 2023 to December 2023.
Questionnaire:
The questionnaire booklet titled START (To Study The clinical
usAge of Rosuvastatin in dyslipidemia coexist with Diabetes,
HyperTeNsion or Cardiovascular disease in Indian Patients) study
was sent to the physicians who were interested to participate in the
study. The START study questionnaire comprised 24 questions
addressing current feedback, clinical observations, and specialists’
experiences regarding lipid management, as well as the use and
prescription patterns of statins, particularly rosuvastatin. The study
was conducted after receiving approval from Bangalore Ethics, an
Independent Ethics Committee which was recognized by the Indian
Regulatory Authority, Drug Controller General of India.Participants:
An invitation was sent to leading clinicians in managing
dyslipidemia in the month of March 2023 for participation in this
Indian survey. About 502 doctors from major cities of all Indian states
representing the geographical distribution shared their willingness to
participate and provide necessary data. Clinicians were provided the
option to skip any questions they did not wish to answer and were
instructed to complete the questionnaire independently, refraining
from consulting colleagues. Prior to the initiation of the study, written
informed consent was obtained from all study participants.Statistical analysis:
The data were analyzed using descriptive statistics. Categorical
variables were presented as percentages to provide a clear
understanding of their distribution. The frequency of occurrence and
the corresponding percentage were used to represent the distribution
of each variable. To visualize the distribution of the categorical
variables, pie, and bar charts were created using Microsoft Excel 2013
(version 16.0.13901.20400).Results
According to the survey data, 45% and 40% of clinicians
observed that 21-30% and 11-20% of young patients (<40 years) have
dyslipidemia, respectively. Additionally, 49% and 34% of clinicians
reported that 21-30% and 10-20% of the patients presenting to
routine practice have comorbid hyperlipidemia and hypertension,
respectively. Similarly, 48% of the clinicians noted that 21-30% of the
patients have comorbid hyperlipidemia and diabetes. Moreover, 48%
of clinicians indicated that 20-30% of patients with hypertension were
prescribed statins as an additional therapy for primary prevention.
Sedentary lifestyle, obesity (particularly visceral obesity), and cigarette
smoking were identified as the major reversible traditional risk factors
to be addressed to reduce the risk of cardiovascular disease by 29%,
27%, and 26% of clinicians, respectively.
As per 47% of the clinicians, nearly 20-30% of patients with
dyslipidemia have a risk attributable to ACS. The majority of
clinicians (62%) identified the increased prevalence of dyslipidemia
and ACS in the age group 45-60 years. Nearly 56% of the clinicians
recommended measuring the ‘lipid profile’ once in 3 months among
patients with ACS, whereas 40% recommended it once in 6 months.
According to 42% and 41% of the clinicians, 10-20% and 20-30% of
patients requiring dual antiplatelet therapy + statins. As per 30% of
the clinicians, statins are believed to reduce CV risk by less than 21-
30% in patients with diabetes.
The majority (57%) of clinicians strongly agreed that high doses
of potent statins reduce CV events to a greater extent than low-dose
statin therapy. More than half (57%) of the clinicians noted that a
combination of statins and fibrates results in a greater reduction in
CV events than statins alone. According to 53% of the clinicians,
20-30% of patients with dyslipidemia required combination therapy
with statins. Nearly 71% of clinicians recommended initiating statin
therapy in all comorbid patients with diabetes or hypertension. A
significant proportion (58%) of clinicians supported the American
College of Cardiology and American Heart Association (ACC/AHA)
2019 lipid guidelines, which advocated administering the maximum
tolerated dose of statins in individuals with LDL-C levels >190 mg/dl.
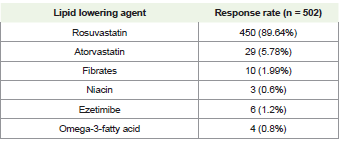
Majority (90%) of the clinicians advocated prescribing rosuvastatin
as a lipid-lowering agent for patients with hyperlipidemia who also
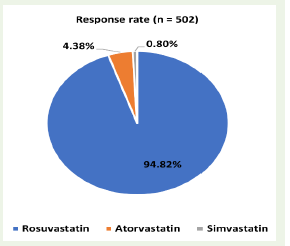
have hypertension or diabetes [Table 1]. Additionally, rosuvastatin
was preferred by a significant proportion of clinicians (95%) as the
recommended statin for patients with dyslipidemia [Figure 1]. A
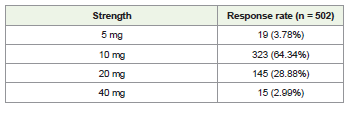
significant portion (64%) of clinicians favored the 10 mg dosage of
rosuvastatin among those with diabetes, regardless of their lipid levels
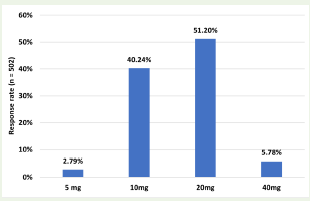
[Table 2]. When considering patients with CVD, regardless of their
lipid levels, 51% of clinicians preferred the 20 mg dosage, while 40%
favored the 10 mg dosage [Figure 2].
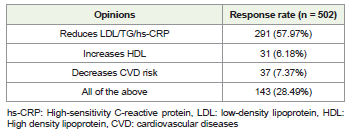
Around 58% of clinicians observed that the combination of
rosuvastatin and fenofibrate helps in reducing LDL/TG/high sensitivity
C-reactive protein (hs-CRP), offering a comprehensive
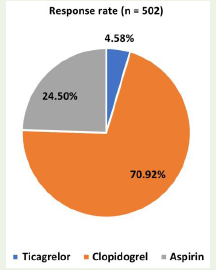
approach to managing the lipid triad [Table 3]. Majority (71%) of
the clinicians preferred clopidogrel as the antiplatelet agent to be
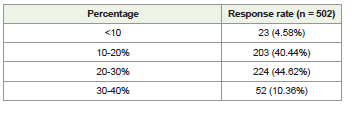
combined with rosuvastatin [Figure 3]. According to 45% and 44%
of clinicians, 20-30% and 10-20% of patients would require the
combination of rosuvastatin and clopidogrel [Table 4]. Moreover,
44% of clinicians suggested a therapy duration of 6-12 months with
rosuvastatin + clopidogrel + aspirin for secondary prevention in high
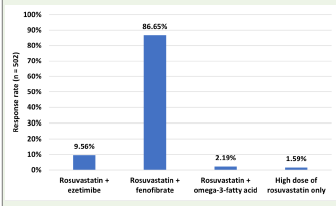
CV-risk patients. Majority (87%) of the clinicians favored adding
fenofibrate to rosuvastatin for patients with elevated triglyceride
levels [Figure 4].
Discussion
The present study adds to the growing body of evidence
supporting the use of statins for lipid management across various
comorbid conditions, including diabetes or hypertension, as well
as among individuals with LDL-C levels exceeding 190 mg/dl.
Additionally, it suggests that 20-30% of patients with dyslipidemia
may require combination therapy involving statins. Furthermore,
clinicians noted that combining statins with fibrates leads to a greater
reduction in CV events compared to statins alone. According to
the 2019 ACC/AHA guideline on the primary prevention of CVD,
statin therapy is recommended as the initial treatment for primary
prevention of atherosclerotic cardiovascular disease (ASCVD) in
several patient groups, including individuals with elevated LDL-C
levels (≥190 mg/dL), those aged 40 to 75 years with type 2 diabetes
mellitus (T2DM), and those assessed to be at increased ASCVD risk
following a clinician-patient risk discussion [10].
A review by Catapano et al. emphasized that for individuals
who fail to achieve sufficient reduction in LDL-C, especially those
at elevated risk or those unable to tolerate maximum statin therapy,
combination therapy involving a low-dose statin and other lipid modifying
agents may be an effective option [11].Agouridis et al.
found that, according to current evidence, combination therapy
involving statins and fibrates positively modifies the lipid profile
of patients with T2DM. This treatment approach is particularly
effective in addressing the high TG and low HDL-C profile, a pattern
associated with increased CVD risk [12].
In the present study, a significant proportion of clinicians
recommended rosuvastatin as a lipid-lowering agent and
recommended statin in patients with hyperlipidemia who also
have hypertension or diabetes. Furthermore, the majority of the
clinicians recommended a 10 mg dosage of rosuvastatin among those
with diabetes and a 20 mg dosage in CVD patients. Barakat et al.
found that rosuvastatin effectively reduced LDL-C levels in diabetic
patients with dyslipidemia [13]. A pooled analysis of data from five
trials demonstrated that rosuvastatin had consistent efficacy across
various patient subgroups, including those aged 65 years and older,
female individuals, postmenopausal individuals, hypertensive
patients, those with atherosclerosis, individuals with T2DM, and
obese individuals [14].A comparative study conducted by Berne
et al. found that rosuvastatin demonstrated superior efficacy over
atorvastatin in reducing LDL-C levels and attaining European LDL-C
targets in patients diagnosed with T2DM [15].In a comprehensive
systematic review and network meta-analysis comprising 50
randomized controlled trials involving 51,956 participants with
dyslipidemia, CVD, or T2DM, researchers investigated the lipid lowering
or increasing efficacy of seven statins. The study concluded
that rosuvastatin demonstrated superior performance, ranking first
in lowering LDL-C and Apo lipoprotein B, as well as increasing
Apolipoprotein A-1levels compared to simvastatin, fluvastatin,
atorvastatin, lovastatin, pravastatin, and pitavastatin [16].A
comparative study conducted by Berne et al. found that rosuvastatin
demonstrated superior efficacy over atorvastatin in reducing LDL-C
levels and attaining European LDL-C targets in patients diagnosed
with T2DM [15].
Among dyslipidemia diabetic patients, rosuvastatin at a dosage
of 10 mg was found to be the most effective in reducing LDL-C levels
[13].The URANUS study found that a significantly higher proportion
of patients achieved the 1998 LDL-C goal when treated with
rosuvastatin 10 mg compared to those treated with atorvastatin 10
mg in individuals with T2DM [15]. Aleem et al. compared the efficacy
of rosuvastatin at doses of 5 mg and 10 mg in patients with T2DM
and dyslipidemia and found that 10 mg of rosuvastatin demonstrated
greater reductions in lipid levels [17]. In high-risk patients with
hypercholesterolemia, rosuvastatin 10 mg demonstrated superior
efficacy compared to atorvastatin 20 mg in reducing LDL-C, thereby
facilitating the achievement of LDL-C goals and enhancing other
lipid parameters [18]. In a post-marketing study conducted by Shah et
al., which assessed the lipid-modifying efficacy and safety of approved
dose ranges of rosuvastatin among Indian hyperlipidemia patients in
routine clinical settings, it was revealed that rosuvastatin at doses of
5 mg, 10 mg, and 20 mg effectively improved lipid parameters and
enabled the attainment of lipid goals in a diverse cohort of Indian
hyperlipidemic patients. Additionally, for individuals with a higher
CV risk profile, starting doses of rosuvastatin at 10 mg and 20 mg
were found to be more effective [19].
Most of the current survey respondents recommended
combining rosuvastatin with fenofibrate to lower LDL/TG/hs-CRP,
elevate HDL, and reduce CVD risk. Clopidogrel was the preferred
choice for combination therapy with rosuvastatin. Clinicians also
favored supplementing rosuvastatin with fenofibrate for patients with
elevated TG levels. Furthermore, clinicians advocated for a treatment
duration of 6-12 months for rosuvastatin + clopidogrel + aspirin
therapy for the secondary prevention of high CV risk.
Machado-Duque et al. found that the combination of rosuvastatin
and fenofibric acid is an effective treatment option for patients
diagnosed with mixed dyslipidemia and at high risk for CV events
with reduced LDL-C and TG level [20]. In a comprehensive review
comprising 46 articles, conducted by Biswas et al., it was observed that
combination therapy involving rosuvastatin and fenofibric acid was
advantageous and well-tolerated, exhibiting a safety profile similar to
that of statin monotherapy. Moreover, the combination of moderate
dose rosuvastatin with fenofibric acid resulted in a reduction of CV
risk factors [21].
Gao et al. reported that the combination of rosuvastatin
and clopidogrel bisulfate has proven to be effective in treating
elderly patients with coronary heart disease (CHD). This regimen
demonstrates the ability to enhance cardiac function, as well as to
lower blood lipid levels and reduce inflammatory factors [22].Deng
et al. found that intensive rosuvastatin therapy combined with 7-day
dual antiplatelet therapy using aspirin and clopidogrel significantly
reduced the risk of recurrent ischemic stroke within 90 days for
patients with mild to moderate acute ischemic stroke, compared to
rosuvastatin plus single antiplatelet therapy. This treatment approach
did not lead to an increase in bleeding events, statin-induced liver
injury, or systemic anticoagulant medication-associated myopathy.
These benefits were more pronounced in subgroups with highrisk
factors, such as elderly patients (>68 years old), those with
hypertension, diabetes, hyperlipidemia, prior stroke history, or those
not receiving antiplatelet therapy before the study [23]. Pillai et al.
examined the prescription practices of fixed-dose drug combinations
(FDCs) containing rosuvastatin, clopidogrel, and aspirin in Indian
patients diagnosed with ACS. The findings revealed that a significant
portion of patients were prescribed the FDC of rosuvastatin,
clopidogrel, and aspirin primarily for the treatment of unstable
angina/ACS [24].
The current survey provides more insights into prescription
practices tailored to Indian contexts, aiding both clinicians and
researchers in making informed decisions. This research seeks to
enhance patient care strategies and contribute to the development
of evidence-based guidelines and recommendations for optimizing
treatment outcomes. The findings of the current study underscore
the importance of statins, particularly rosuvastatin, in managing lipid
levels in patients with comorbid conditions. One notable strength
of the study lies in the utilization of a meticulously designed and
validated questionnaire for collecting expert data. However, it is
important to acknowledge that personal viewpoints and preferences
may have influenced the conclusions drawn from the study,
introducing the possibility of bias. Therefore, interpreting the results
while considering these limitations is crucial. Further research efforts
should be directed towards confirming and expanding upon the
findings presented in this study.
Conclusion
The present survey further corroborated the significance of statin
combination therapy, with notable benefits observed when combined
with fibrates for reducing cardiovascular events. Rosuvastatin
emerged as a favored lipid-lowering agent, especially in patients
with hyperlipidemia, hypertension, or diabetes. Combination
therapy, particularly with fenofibrate, is favored to address multiple
lipid parameters and reduce cardiovascular risk. Clopidogrel is the
preferred choice for combination therapy with rosuvastatin, and a
treatment duration of 6-12 months is recommended for secondary
prevention in high cardiovascular risk patients.
References
Citation
Manjula S, Krishna Kumar M. Expert Opinion on the Prescription Practice of Statins in Lipid Management with a Specific Focus on Rosuvastatin Use in Indian Settings. Indian J Cardio Biol Clin Sci. 2024;7(1): 114.