Case Report
Unicuspid Aortic Valve in an ElderlyMale: Preoperative Transthoracic and Transesophageal Echocardiographic Appraisal
Singh S1*, and Kumar Sethi K2
Corresponding author: Sukhvinder Singh, Department of Non-invasive cardiology, Delhi Heart and Lung Institute,Pachkuyian Road, New Delhi- 110003, India, Tel: 9717205832;E-mail: kuks145@yahoo.co.in
Citation: Singh S, Kumar Sethi K. Unicuspid Aortic Valve in an Elderly Male: Preoperative Transthoracic and Transesophageal Echocardiographic Appraisal. Indian J Cardio Biol Clin Sci. 2017;4(1): 109.
Copyright © 2017 Singh S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Cardio Biology & Clinical Sciences | Volume: 4, Issue: 1
Submission: 22/02/2017; Accepted: 30/03/2017; Published: 03/04/2017
Abstract
We present a case of unicuspid aortic valve in an elderly patient who had aortic stenosis, aortic regurgitation and dilated aortic root. Transthoracic and transesophageal echocardiographic profile of this rare entity is being discussed.
Keywords: Unicuspid aortic valve; Unicommissural; Acommissural; Aortic stenosis; Aortic regurgitation
Abbreviations: TTE: Transthoracic Echo; VTI: Velocity Time Integral; TEE: Transesphageal Echocardiography
Introduction
Unicuspid aortic valve is a rare congenital cardiac anomaly in adult population. It usually results in a combination of aortic stenosis with aortic regurgitation by 3rd to 5th decade of life. Diagnosis is commonly made on operative table or during autopsy [1].
Case Details
The patient was a male of 63 years of age who presented atoutdoor clinic with complaints of breathlessness on exertion for last3 months. On clinical examination there was a grade 4/6 mid systolicmurmur at right upper parasternal area which was radiating wellto carotids. There was a long diastolic murmur at left parasternalarea. Transthoracic echo revealed aortic valve stenosis with a meangradient of 38.24 mmHg and VTI ratio of 0.29 (Figures 1,2). There was moderate aortic regurgitation with pan-diastolic reversal of flow in descending thoracic aorta with end-diastolic velocity of 0.25 mmHg (Figure 3,Video 1). There was dilatation of aortic root at sinus level (41 mm) and that of ascending aorta (55 mm) (Figures 4,and 5). Parasternal long axis view revealed thickened and calcified aortic valve which was prolapsing in left ventricular outflow tract during diastole and two separate cusps, as normally visible in this view, were not being seen (Video 2). There was suspicion of bicuspid aortic valve on short axis view with heavily calcified edges (Video 3). Transesphageal echocardiography was performed for further evaluation. TEE revealed a unicommissural unicuspid aortic valve with a slit like opening and calcified edges (Videos 4 and 5).
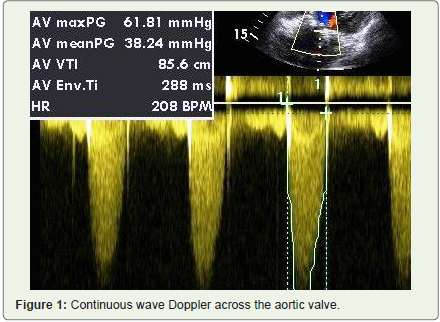
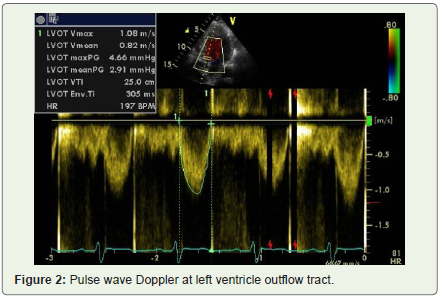
Figure 2: Pulse wave Doppler at left ventricle outflow tract.
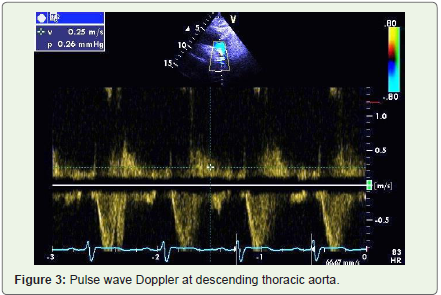
Figure 3: Pulse wave Doppler at descending thoracic aorta.
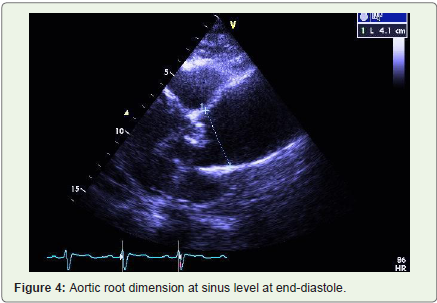
Figure 4: Aortic root dimension at sinus level at end-diastole.
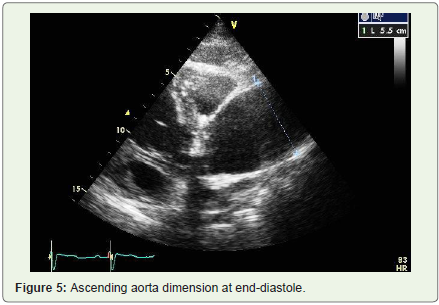
Figure 5: Ascending aorta dimension at end-diastole.
Discussion
Mechanism of Action
Unicuspid aortic valve is a rare congenital cardiac anomaly in adult population. In a systemic review, only 231 adult patients with this anomaly could be identified over a period of 42 years [1]. In another single center study, the incidence was found to 0.02% in adult population [2]. However, in a recent single center study, 42 adult cases of the entity were found over a period of 5 years [3]. It is predominantly found in male patients [2]. Age of presentation is typically 3rd to 5th decade of life [1]. However, our patient presented inseventh decade of life.
Morphologically there are two varieties of unicuspid aortic valve. It may be acommissural or unicommissural. Acommissural unicuspid aortic valve has a central tiny opening (pin hole). It has no commissure or attachment to the lateral aortic wall at level of orifice [4,5]. It presents early in life typically in infancy. However, in a large surgical study, 4 out of 46 cases of unicuspid aortic valve in adult patients had acommissural valves [6]. Unicommissural unicuspid valve has one commissure and it is attached to the lateral wall of aorta at the level of orifice. It has a slit shaped opening which has been described as “teardrop†shaped orifice. It typically has a lot of calcification which makes its assessment difficult on transthoracic echo. It usually presents as a combination of aortic stenosis with aortic regurgitation. Aortic root dilatation is commonly associated [4,5].
As compared to bicuspid aortic valve disease, patients present early, have predominantly mixed stenotic and regurgitant lesions and have higher incidence of aortic annulus dilatation vis-a-vis ascending aorta dilatation [3].
Commonest presenting feature is breathlessness. Though, patients may present with syncope or angina. Pre-operative diagnosis of this entity is uncommon and as per a systematic review, pre-operative diagnosis could be established only in 40% of the cases [1].
Hence, we present pre-operative echocardiogprahic profile of a rare adult congenital heart disease which is difficult to diagnose preoperatively and was unusual by the virtue of older age of patient and severe dilatation of ascending aorta.
References
- Mookadam F, Thota VR, Garcia-Lopez AM, Emani UR, Alharthi MS, et al. (2010) Unicuspid aortic valve in adults: a systematic review. J Heart Valve Dis 19: 79-85.
- Novaro GM, Mishra M, Griffin BP (2003) Incidence and echocardiographic features of congenital unicuspid aortic valve in an adult population. J Heart Valve Dis 12: 674-678.
- Noly PE, Basmadjian L, Bouhout I, Viet Le VH, Poirier N, et al. (2015) New insights into unicuspid aortic valve disease in adults: Not just a subtype of bicuspid aortic valves. Can J Cardiol 32: 110-116.
- Anderson RH (2003) Understanding the structure of the unicuspid and unicommissural aortic valve. J Heart Valve Dis 12: 670-673.
- Brantley HP, Nekkanti R, Anderson CA, Kypson AP (2012) Three-dimensional echocardiographic features of unicuspid aortic valve stenosis correlate with surgical findings. Echocardiography 29: E204-E207.
- Roberts WC, Ko JM (2005) Frequency by decades of unicuspid, bicuspid, and tricuspid aortic valves in adults having isolated aortic valve replacement for aortic stenosis, with or without associated aortic regurgitation. Circulation 111: 920-925.