Case Report
Multifocal Ewing Sarcoma with Pancreatic and Cutaneous Metastasis-A Rare Case Report
SSM Zainul Abidin Sarmast1* and Amrit Kaur2
1Fellow in Onco-Imaging, Department of Radio Diagnosis, Kidwai Memorial Institute of Oncology, Bangalore, India
2Department of Pediatric Oncology, Kidwai Memorial Institute of Oncology, Bangalore, India
2Department of Pediatric Oncology, Kidwai Memorial Institute of Oncology, Bangalore, India
*Corresponding author: SSM Zainul Abidin Sarmast, Fellow in Onco-Imaging, Department of Radio Diagnosis, Kidwai Memorial Institute of Oncology, Bangalore, India Email: zain.sarmast.zs60@gmail.com
Copyright: © 2023 Zainul Abidin Sarmast SSM, et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 14/10/2023; Accepted: 16/11/2023; Published: 21/11/2023
Abstract
We present a rare case of Multifocal Ewing sarcoma with pancreatic and cutaneous metastasis in a 13-year-old boy who initially presented with unprovoked epistaxis and symptoms of chronic rhinosinusitis. Distinguishing Ewing sarcoma from similar sinonasal tumours is challenging through clinical
and radiological assessments alone, necessitating precise histopathological, immunohistochemical, and cytogenetic analyses. The involvement of multiple bones at the time of diagnosis is unusual, and the presence of cutaneous and pancreatic metastasis is exceptionally rare. These unique features pose
diagnostic complexities, highlighting the necessity of a comprehensive, multidisciplinary approach for both diagnosis and management.
Keywords: Ewings Sarcoma; Cutaneous Metastasis; Pancreatic Metastasis; Histopathology; Immunohistochemistry
Introduction
Ewing sarcoma is a malignant tumor that can develop in either
bones or soft tissues and has the potential to arise in various parts of
the body, although it primarily manifests in bones. Initially coined as
“diffuse hemangio-endothelioma of bone” by James Ewing in 1921, he
theorised that it originated from the endothelial cells lining the blood
vessels within the bone. However, the precise cell of origin remains
a subject of ongoing debate [1]. This cancer is highly aggressive,
especially in children, and ranks as the second most prevalent primary
bone tumor. While it can affect nearly any bone, the trunk and long
bones are the most frequently impacted.
Typically, Ewing sarcoma presents as a single bony abnormality. In
rare instances, it may involve multiple bones at the time of diagnosis.
In this paper, we report an unusual case of Multifocal Ewing sarcoma
presenting with bilateral scapular lesions, para-nasopharyngeal
mass lesion, pancreatic and cutaneous lesions. These combinations
of clinical findings are a very rare entity and, as far as we know, no
similar case has been documented in the English literature.
Case Report
A 13-year-old boy presented with history of frequent mild to
moderate unprovoked epistaxis from left nostril in the past 7 days.
His other complaints were intermittent nasal blockage and rhinorrhea
and pain in both legs. There was also history of weight loss and loss
of appetite. No fever, easy fatiguability, easy bruisability or blood
transfusion. Clinical examination showed a polyp-like mass with
crusting in left nostril and a 4 x 4 cm mass in oral cavity on the left
side in the posterior pharynx. His systemic examination was normal.
Basic hematological and biochemistry profile was normal.
As the patient is a13-year-old male with a nasal mass with
unprovoked epistaxis, the clinical diagnosis of juvenile nasopharyngeal
angiofibroma (JNA) was considered and the differential diagnoses
included, inverted papilloma and sinonasal carcinoma, which
were commoner for the unilateral sinonasal mass. CECT Neck and
PNS was advised for further evaluation.
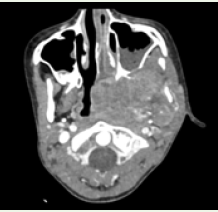
CECT neck and paranasal sinuses showed a large heterogeneously
enhancing mass lesion involving the left para-nasopharyngeal,
masticator and pharyngeal mucosal spaces bulging into the
nasopharynx. The lesion did not show arterial phase enhancement as
would be expected in JNA, showed heterogeneous enhancement in
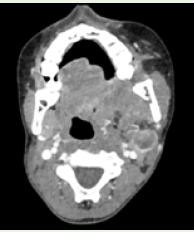
venous phase, involving the muscles of the masticator space [Figure 1]. There was an enlarged peripherally enhancing necrotic left level
II lymph node as well [Figure 2]. Considering age and the above
features, the imaging diagnosis of a small round cell tumor, likely
rhabdomyosarcoma was proposed.Inverted papilloma is a benign
tumour and would not have metastatic deposits, hence was ruled out.
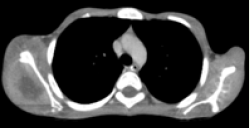
The differentials included sinonasal carcinoma. Metastasis was also
given as a differential as the lower CT cuts at the thoracic inlet showed
a heterogeneously enhancing lesion in the visualised portions of left
scapula with adjacent abundant soft tissue. CECT thorax was advised
for complete evaluation of the scapular mass.
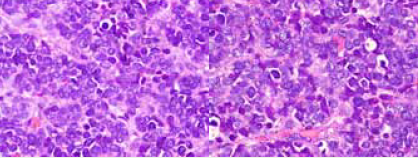
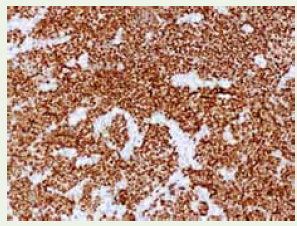
Mean while biopsy was done from the oral cavity mass as the
possibility of JNA was ruled out. The biopsy was suggestive of poorly
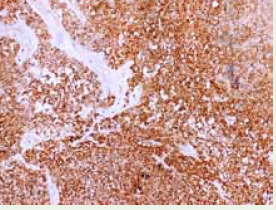
differentiated round cell malignancy [Figure 3]. Given the various
differential diagnosis of small round blue cell tumors in nasopharynx,
an immunohistochemical test was carried out. To our surprise
neoplastic cells were positive for CD99, NKX2.2 and negative for
CK, LCA, P63, CK5/6, CD56, desmin, chromogranin, myogenin and
INSM1 [Figure 4] and [Figure 5].
FISH for EWSR1 gene was sent and was positive and confirmed the diagnosis of Ewing Sarcoma.
Further, CECT thorax, was done which showed multiple skeletal
lesions with large soft tissue components exhibiting aggressive
periosteal reaction involving bilateral scapulae, multiple ribs and
vertebral bodies. [Figure 6] and [Figure 7]. Enhancing subcutaneous
nodule in the left anterior chest wall was seen [Figure 8] and
heterogeneously enhancing pancreatic lesions involving the head,
uncinate process and tail regions were also noted [Figure 9] and
[Figure 10]. Ultrasound images of the subcutaneous nodule in the
right anterior chest wall and the pancreatic tail region are depicted


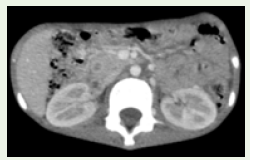
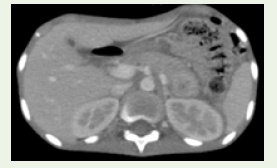


in [Figure 11] and [Figure 12]. FNAC from the subcutaneous nodule
and the pancreatic lesion was done under ultrasound guidance which
showed malignant small round blue cells suggesting cutaneous and
pancreatic metastasis.
Bone marrow biopsy was done to rule out marrow
involvementand showed intertrabecular spaces replaced by infiltrating
neoplasm displaying similar morphology. Patient was started on
standard chemotherapy with VAC (vincristine, adriamycin, and
cyclophosphamide) alternating with IE (ifosfamide and etoposide).
Patient showed stable response after 3 cycles of chemotherapy.
Discussion
Ewing sarcoma, peripheral primitive neuroectodermal tumor
(PNET), and Askin tumor are grouped as a single entity due to their
common genetic characteristics. These tumors are now collectively
referred to as the Ewing sarcoma family and are distinguished by
distinct genetic fusions involving FUS, EWSR1, TAF15 (FET), and
E26-specific (ETS) FET-ETS genes [2,3]. While these tumors typically
arise in bones, they can also manifest in the nasal and sinus regions,
often causing vague symptoms. Ewing sarcoma in the head and neck
is rare, accounting for only 1-4% of cases, and it’s even rarer in the
nasal and sinus areas [4,5].
In this case, as the patient presented with symptoms of frequent
mild to moderate unprovoked epistaxis and features of chronic
rhinosinusitis, our initial differential diagnosis included juvenile
angiofibroma, sinonasal carcinoma andinverted papilloma which
were more commoner for the unilateral sinonasal mass.
However,after the imaging and biopsy investigations,we were
convinced we were dealing with something else.
Distinguishing Ewing sarcoma from similar sinonasal
tumours based solely on clinical and radiological assessments is
challenging. Therefore, an accurate diagnosis typically requires
histopathological, immunohistochemical and cytogenetic analyses.
Immunohistochemistry usually shows strong CD99 expression while
lacking markers associated with muscles and blood cells. In this
instance, CD99 and NKX2.2 were positive, while other markers were
negative, confirming the diagnosis of Ewing sarcoma.
The imaging finding that hints towards the diagnosis is the bone
centric appearance of the lesions with exuberant soft tissue on either
sides of bilateral scapulae with aggressive periosteal reaction and not
much of cortical destruction. Ewing sarcomas are usually found in
the shafts of long bones and tend to extend into nearby soft tissues.
Bilateral scapular involvement in a case of Ewing sarcoma as seen in
this case is quite unusual.
Cutaneous metastasis is rarely reported in literature [6]. The
lesions appear as solitary dermal nodules and they show predilection
for young individuals. In our case patient had cutaneous nodules over
right side of anterior chest wall and FNAC of which was suggestive of
neoplastic small round blue cells.
Our case highlights the rarity of Ewings Sarcoma metastasis to
the pancreas as well and till now only 4 cases of Ewings Sarcoma are
reported with pancreatic metastasis [7]. It is to be noted that there is
no evidence that ESFT is associated with any familial predisposition
syndrome or environmental factors [8].
Overall survival rates vary based on whether the cancer has
spread at the time of diagnosis. Patients with localized disease tend to
have a better prognosis than those with metastatic disease. Prognostic
factors include the patient’s age, cancer stage, tumour size, and its
location. Patients under 15 years of age without metastasis generally
have a more favourable outcome compared to those with metastasis.
In summary, Ewing sarcoma occurring in the head and neck is a
rare occurrence, and its accurate diagnosis depends on histopathology
and immunohistochemistry. Prognosis is significantly influenced by
factors such as the presence of metastasis and the patient’s age.
Conclusion
Ewing sarcoma presents a wide histological variety,
leading to complex diagnostic issues that demand expertise in
immunohistochemistry and cytogenetics. Ewing sarcoma in the head
and neck is infrequent, and its presence in the sinonasal region is
even more rare. Our case highlights the rare presentation of Ewings
Sarcoma with cutaneous and pancreatic metastasis making the
diagnosis more challenging. It is a multimodality approach which is
required for the diagnosis and management for Ewing sarcoma, which
involves various investigations. An effective treatment plan including
chemotherapy and surgery or chemoradiotherapy is needed for local
remission and healing with a better survival rate.
Acknowledgements
Dr Madhu S D, Professor and HOD, Department of Radio
Diagnosis, Kidwai Memorial Institute of Oncology, Bangalore.
Dr Nuthan Kumar, Associate Prof, Department of Pediatric
Oncology, Kidwai Memorial Institute of Oncology, Bangalore.
Dr Suma Mysore Narayana, Associate Professor, Department of
Pathology, Kidwai Memorial Institute of Oncology, Bangalore.
The patient’s guardian (Mother) consent was taken for the study.
References
Citation
Zainul Abidin Sarmast SSM, Kaur A. Multifocal Ewing Sarcoma with Pancreatic and Cutaneous Metastasis-A Rare Case Report. Indian J Appl Radiol. 2023;9(1): 187.