Research Article
CT Pulmonary Angiography in COVID-19 Pneumonia: A Retrospective Study of Relationship between Pulmonary Embolism and Disease Severity
Panchal V1, Desai P2 and Wadhwani U2*
1Consultant radiologist, Govt Medical College, New Civil Hospital, Surat India
2Department of Radiodiagnosis and Imaging, Govt Medical College, New Civil Hospital, Surat India
2Department of Radiodiagnosis and Imaging, Govt Medical College, New Civil Hospital, Surat India
*Corresponding author: Udita Wadhwani, Department of Radio Diagnosis and Imaging, Govt Medical College and New Civil Hospital, Surat India Email: dharasavaliya61@gmail.com
Copyright: © 2023 Panchal V, et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 20/04/2023; Accepted: 28/08/2023; Published: 30/08/2023
Abstract
Introduction: Coagulopathy has been commonly reported in patients with COVID positive status. We conducted this study relationship between pulmonary embolism and covid 19 disease severity. clear understanding of rate of embolism, correlation with D dimer levels and the degree of involvement
of thrombosis can be of great help in management of COVID positive patients.
Study design and methods: In this observational retrospective study, conducted over a period of 2 months, all the suspected COVID patients referred to our institute with complaints of breathlessness and suspected to be having thromboembolism were included. These patients were first subjected to HRCT chest and were followed up for CTPA after patient’s symptoms worsened and were assessed the presence or absence of arterial thrombosis
Results: Out of the evaluated 34 patients, none of them were seen to have pulmonary thromboembolism in main pulmonary trunk, while 14 patients were found to have thrombosis involving right and left pulmonary arteries and their ascending and descending branches and all 34 patients were found to have thrombosis in segmental and subsegmental branches.
Interpretation: Thromboembolism, including pulmonary embolism, is one of the known and frequent complications in COVID patients. In cases with sudden clinical worsening CT Pulmonary angiography should be done to confirm pulmonary embolism which is a life-threatening but potentially treatable condition.
Study design and methods: In this observational retrospective study, conducted over a period of 2 months, all the suspected COVID patients referred to our institute with complaints of breathlessness and suspected to be having thromboembolism were included. These patients were first subjected to HRCT chest and were followed up for CTPA after patient’s symptoms worsened and were assessed the presence or absence of arterial thrombosis
Results: Out of the evaluated 34 patients, none of them were seen to have pulmonary thromboembolism in main pulmonary trunk, while 14 patients were found to have thrombosis involving right and left pulmonary arteries and their ascending and descending branches and all 34 patients were found to have thrombosis in segmental and subsegmental branches.
Interpretation: Thromboembolism, including pulmonary embolism, is one of the known and frequent complications in COVID patients. In cases with sudden clinical worsening CT Pulmonary angiography should be done to confirm pulmonary embolism which is a life-threatening but potentially treatable condition.
Keywords: COVID 19; Pneumonia; Pulmonary Embolism; CT Angiography
AbbreviationsCOVID-19, HRCT, CTPA
Introduction
The novel Coronavirus disease began to take its course in
December 2019 and by March 2020 reaching the pandemic levels [1].
According to the current guidelines RT-PCR (reverse transcriptase
polymerase chain reaction) is considered confirmatory for COVID
testing. However those with negative test having positive findings
on CT are considered to have lung involvement which is analysed in
the form of CT severity classification system. However, CT can be
falsely negative early in the disease but HRCT reserved for evaluation
of complications in patients with COVID positive status [2].
Coagulopathy has been commonly reported in patients with
COVID positive status and has been associated with increased
mortality with lab findings of elevated D-dimer levels [3]. It was found
that patients who were empirically treated with low molecular weight
heparin had a lower morbidity and mortality as compared to those
that were not treated with LMWH [4,5]. A significance of embolism
is thus associated with worst clinical outcome in COVID-19 patients.
How-ever this seems to be challenging in evaluation of terminally
ill patients and possibly acute kidney injury as both the risk of
nephrotoxicity from IV contrast administration and potential benefit
of diagnosing pulmonary thromboembolism needs to be considered
[6]. Thus, clear understanding of rate of embolism, correlation with
D dimer levels and the degree of involvement of thrombosis can be of
great help in management of COVID positive patients.
It is necessary to look for embolism in main pulmonary artery,
its right or left main branches, the lobar branches and even the
proceeding segmental and sub segmental branches [7]. We conducted
this study relationship between pulmonary embolism and covid 19
disease severity.
CT pulmonary angiography not only can assess the presence of
pulmonary embolus but also can assess the severity of the embolus as
well as heart function and strain on the right ventricle. Thus, we can
predict the need for ICU admission and patient outcome [8].
Material and Methods
In this retrospective study all the suspected COVID patients
referred to the department of radiology at government medical
college, Surat with complaints of breathlessness and suspected to be
having thromboembolism were included. The study was conducted
over a period of 2 months from including April and May 2021. These
patients were first subjected to HRCT chest and were followed up for
CTPA after patient’s symptoms worsened.
Written and informed consent of the patient taken with risk
factors explained to the relatives. Patient then were taken for CTPA
with all the necessary precautions as per the protocols and guidelines
on Philips’s brilliance 256 slice CT machine dedicated for Covid
patients at the department.
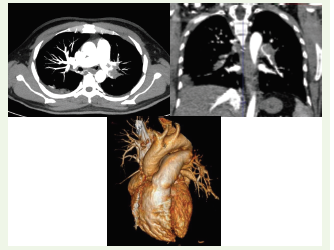
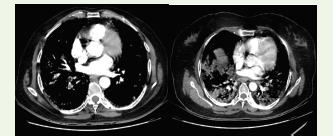
We assessed the presence or absence of arterial thrombosis i.e.,
filling defect in the form of is Odense to hypodense content within
pulmonary vasculature and reported presence, extent and location of
thrombus if any. The presence of thrombus was described in terms of
unilateral vs bilateral involvement, lobar, segmental or subsegmental
involvement.
CT Technique:
Patients’ preparation: Patients were required to fast for 6-8 h,
and normal kidney function was needed using serum creatinine as
a reference. Adequate hydration was instructed before and after the
procedure. An 18–20-gauge cannula was inserted into the antecubital
vein.CT Machine: Philips’s brilliance 256 slice:
CT machine. The infection control parameters were applied under
the guidance of the hospital infection control unit.The patients were scanned in a supine position with the arm
above the head. A breath-hold was requested from the patients
trying to avoid respiratory motion artifact. A region over interest was
drawn on the main pulmonary artery. Bolus IV injection of non-ionic
contrast medium 1.2 ml/kg was used at rate 4 ml/s using injector
pump followed by 40 ml saline at rate 4 ml/s.
CT parameters: The scan area extended from diaphragm to lung
apex with scan time used = 10 s. The tube voltage was 140/80 KVP
and tube current: 51/213 mAs. Rotation time was 0.33 s, 0.75mm
thickness, 0.7 reconstruction increment (mm), and 0.7 Pitch.
Image processing and interpretation: The images were transferred to the workstation where the axial cuts and multi-planar
reformation were examined.
The following items were fulfilled: Positive pulmonary embolism, site if unilateral or bilateral, and extent if segmental, lobar,
or main arterial.
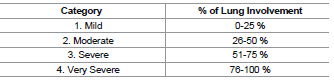
Based on a percentage of lung involvement on HRCT for changes
of covid pneumonitis, patients were divided as follows:
Presence or absence of CT progression comparing the CTPA with
the last available study regarding the parenchymal involvement.
Result
A total of 34 cases were included in this study. Out of 34 cases
there were 26 males and 8 females with a M:F ratio of 3.25:1.
The mean age of the patients was 51.3 ± 16.9 years with age range 20–75.
The mean age of the patients was 51.3 ± 16.9 years with age range 20–75.
From the above mentioned table::
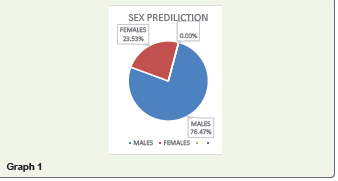
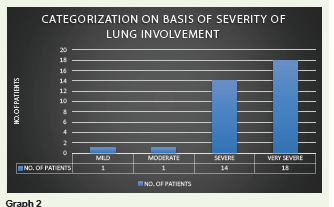
Out of the evaluated 34 patients with pulmonary
thromboembolism, one patient each fell under mild and moderate
category respectively.14 (41%) patients out of 34 fell under severe category and 18 (52.9
%) patients under very severe category.
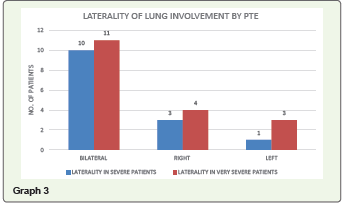
Of the 14 patients with severe lung involvement, 10 (71 %) patients
showed changes of pulmonary thromboembolism in bilateral lungs; 3
(22 %) patients in right lung and 1 (7%) patient in left lung.
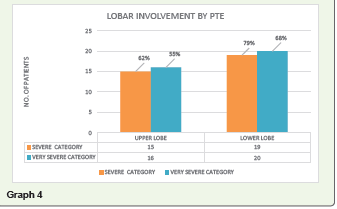
Among patients in severe category, irrespective of the laterality
of lung involvement, total of 24 each upper and lower lobe were
evaluated. The changes of thromboembolism were seen in 15 (62 %)
upper lobes and 19 (79 %) lower lobes.
Of the 18 patients with very severe lung involvement, 11 (61%)
patients showed changes of pulmonary thromboembolism in bilateral
lungs; 4 (22%) patients in right lung and 3 (17 %) patients in left lung.
Among patients in very severe category, irrespective of the
laterality of lung involvement, total of 29 each upper and lower lobe
were evaluated. The changes of thromboembolism were seen in 16 (55
%) upper lobes and 20 (68%) lower lobes.
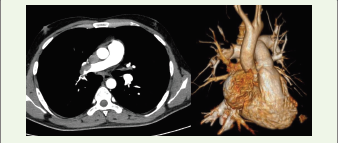
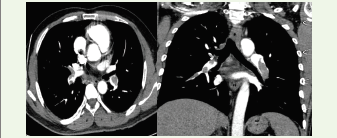
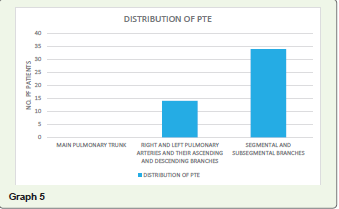
None of the patients out of the evaluated 34 were seen to have
pulmonary thromboembolism in main pulmonary trunk, while
14 patients were found to have thrombosis involving right and left
pulmonary arteries and their ascending and descending branches
and all 34 patients were found to have thrombosis in segmental and
subsegmental branches.
Discussion
Our study of 34 patients with changes of pulmonary
thromboembolism shows that the embolism was predominantly
involving segmental and sub segmental branches of pulmonary
artery and more so in bilateral lung fields which correlates with
studies of Bompard F et al who conducted a retrospective study of
137 patients with confirmed SARS-Cov-2 infection and COVID-19
pneumonia [9]. All these patients underwent computerized
tomographic angiography. In this study a total of 32 Pulmonary
embolism cases were identified resulting in a 24%incidence. Out of
these 32 cases there were 10 proximal pulmonary embolism cases and
22 peripheral Pulmonary embolism cases 18 of which were involved
segmental pulmonary arteries and 4 were involved in multiple
subsegmental pulmonary arteries.
Alonso-Fernández A et al also conducted a study in which 30
consecutive confirmed cases of COVID-19 pneumonia with D-dimer
>1 μg/mL underwent computed tomography pulmonary angiography
(CTPA) to find out presence of pulmonary embolism, the authors
found that out of 30 studied cases 15 had pulmonary embolism on
CTPA resulting in the incidence of 50%.[10] The authors reported
that embolism was found predominantly In peripheral and bilateral
(60%) distribution, affecting mainly segmental and subsegmental
arteries. Similar finding were also reported by the authors such Desai
R as et al [11] and Shi L et al. [12].
A major limitation in our study was relatively small sample
size. Additionally due to retrospective study many patients lacked
laboratory testing of coagulation and inflammatory markers during
their workup. Future investigation with larger number of sample size
may aid in further evaluation of the influencing factors for pulmonary
embolism.
Another interesting fact to be noted was that as the percentage
of lung involvement on HRCT for changes of covid pneumonitis
increases, there is an increase in incidence of thromboembolic events.
Conclusion
Thromboembolism, including pulmonary embolism is one of the
known and frequent complication in COVID patients. In cases with
sudden clinical worsening CT Pulmonary angiography should be
done to confirm pulmonary embolism which is a life threatening but
potentially treatable condition.
Ethical Statement:: ”The study was conducted in accordance with
the declaration of Helsinki, and the protocol was approved by the
Human Research Ethics committee of Government college, Surat”
References
Citation
Panchal V, Desai P, Wadhwani U. CT Pulmonary Angiography in COVID-19 Pneumonia: A Retrospective Study of Relationship between Pulmonary Embolism and Disease Severity. Indian J Appl Radiol. 2023;9(1): 185.