Case Report
A Rare Case of Intrauterine Retained Foetal Bones Clinically Presenting with Pelvic Pain and Dysmenorrhea Following First Trimester Medical Termination of Pregnancy
Swati Kshirsagar1, Shreyas Masrani2, Pratima Patil2, Ajay Gupta2 and Debraj Saha2*
1Head of Department Bharat Ratna Dr Babasaheb Ambedkar Municipal Hospital, Kandivali (W), Mumbai, India
2Department Bharat Ratna Dr Babasaheb Ambedkar Municipal Hospital, Kandivali (W), Mumbai, India
2Department Bharat Ratna Dr Babasaheb Ambedkar Municipal Hospital, Kandivali (W), Mumbai, India
*Corresponding author: Dr. Debraj Saha MD, Radiodiagnosis, Senior Resident, Bharat Ratna Dr Babasaheb Ambedkar Municipal Hospital, Kandivali (W), Mumbai. Mob: 9830081757; Email: debrajdon7521@gmail.com
Copyright: © 2023 Kshirsagar S, et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 15/03/2023; Accepted: 04/05/2023; Published: 08/05/2023
Abstract: Background/Objective: There are various causes of dysmenorrhea and abnormal uterine bleeding; namely endometrial polyp, endometrial hyperplasia and carcinoma; bleeding diathesis; fibroid uterus; and hormonal dysfunctions. When a patient comes to the emergency with pelvic pain and abnormal uterine bleeding, these causes must be ruled out. However, in a patient who has undergone first-trimester abortion recently, there is another cause which we need to keep in mind and that is intrauterine retention of foetal bones.
Materials and Methods/Learning Objective: She was advised CECT pelvis and MRI pelvis outside (in a private diagnostic centre) for evaluation of the abdominal pain. Once referred to our institute, transvaginal ultrasound was performed by the head of the department of radiodiagnosis of the institute.
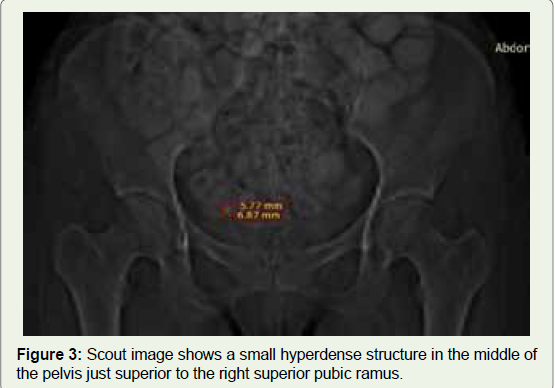
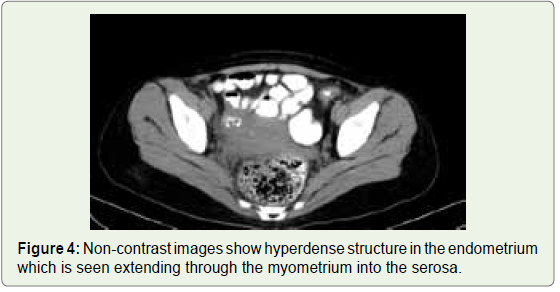
Results/Imaging findings: Contrast-enhanced Computed Tomography scan of the Pelvis revealed a bulky uterus with hyperdense content seen extending from the endometrium to the serosa through the myometrium; with associated collection in the right adnexa; suggesting sealed-off perforation. MRI pelvis confirmed the findings mentioned in the CECT scan.
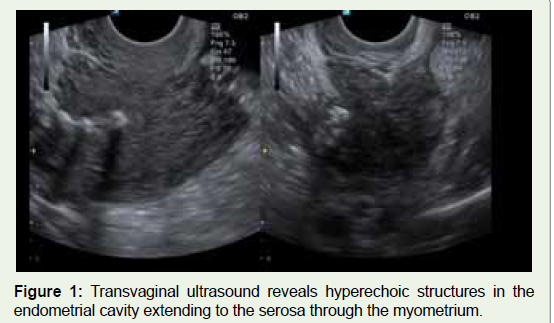
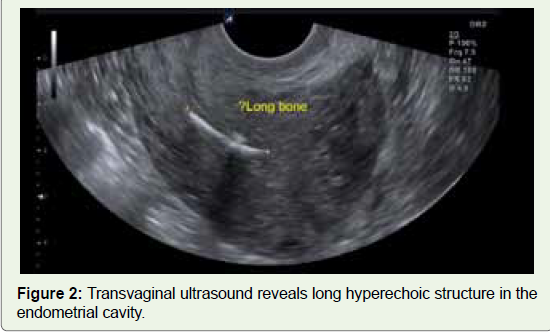
Transvaginal Ultrasound- It was reported as linear calcific structures seen in the endometrium with posterior acoustic shadowing in the lower and middle part of the body of the uterus. It was seen extending to the myometrium with possible perforation through the right lateral wall into the right adnexa.
Conclusion: These days, when there are alternative medical methods of performing medical termination of pregnancy, procedures like dilation and curettage must be avoided as much as possible. However, in a case of a female patient presenting with abnormal uterine bleeding post-medical termination of pregnancy, a high degree of suspicion must be raised to look out for intrauterine retained foetal bones. A transvaginal scan done by a trained radiologist should be enough to confidently diagnose the condition if it happens.
Introduction
There are various causes of dysmenorrhea and abnormal uterine
bleeding; namely endometrial polyp, endometrial hyperplasia
and carcinoma; bleeding diathesis; fibroid uterus; and hormonal
dysfunctions. [1] When a patient comes to the emergency with pelvic pain and abnormal uterine bleeding, these causes must be ruled out.
However, in a patient who has undergone first-trimester abortion
recently, there is another cause which we need to keep in mind and
that is intrauterine retention of foetal bones. [2] Intrauterine foetal
bones may present with dysmenorrhea, abnormal uterine bleeding,
pelvic pain and secondary infertility.
Case Report
A 27-year-old female (P1L1A1) with a previous history of fullterm
vaginal delivery underwent first-trimester Medical Termination
of Pregnancy (by dilation and curettage) at 3 months of amenorrhea.
She came to the gynaecological department with complaints of
post-procedural discharge and bleeding for 2 weeks; and pain in the
abdomen for 1 week.
She was advised CECT pelvis and MRI pelvis outside (in a private
diagnostic centre) for evaluation of the abdominal pain.
Contrast-enhanced Computed Tomography scan of the Pelvis
revealed a bulky uterus with hyperdense content seen extending
from the endometrium to the serosa through the myometrium;
with associated collection in the right adnexa; suggesting sealed-off
perforation. The hyperdense content was mentioned as a possible
organized hematoma. MRI pelvis confirmed the findings mentioned
in the CECT scan.
She was admitted to our hospital for its management and the
patient was sent to our department for ultrasonography.
Transvaginal ultrasound was performed by the head of the
department of radiodiagnosis of the institute. It was reported as linear
calcific structures seen in the endometrium with posterior acoustic
shadowing in the lower and middle parts of the body of the uterus.
It was seen extending to the myometrium with possible perforation
through the right lateral wall into the right adnexa. The diagnosis was
given as retained intra-uterine foetal bones; with associated sealed-off
perforation (Figure 1-6).
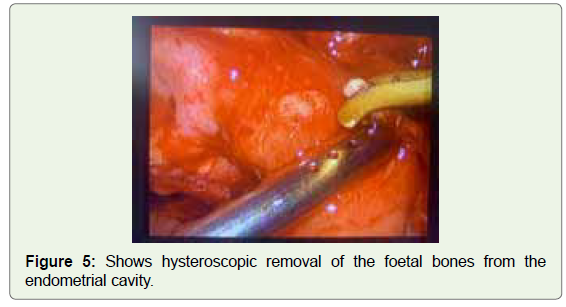
Management:
Under all aseptic guidelines and proper consent, the patient
was posted for surgical removal of the foetal bone through the
hysteroscopy route. 3 bones were retrieved and the diagnosis made
by transvaginal ultrasound was confirmed.
No complications occurred during the procedure and the patient
was discharged after 7 days. The complaints of dysmenorrhea, chronic
pelvic pain and abnormal uterine bleeding have stopped.Discussion
Medical termination of pregnancy is one of the most neglected
problems in our country. [3] Retained foetal bones in a rare
complication of unsafe abortion. The incidence is 0.15% in patients
undergoing diagnostic hysteroscopy. [4]
Menstrual blood volume and prostaglandin concentration were
measured by Lewis et al; before and after the removal of retained
foetal bones.[5] The menstrual blood volume and total prostaglandin
concentration were reduced to half after the removal of foetal bones.
In our case, abnormal uterine bleeding probably occurred through
the same mechanism.[6]
After 12 weeks of gestation, any foetus is capable of enchondral
ossification.[7] The bones appear as hyperechogenic areas with
posterior shadowing. This is important as deeply embedded bones are
likely to be missed on hysteroscopy.[8] Treatment of retained foetal
bone is removal either through evacuation by conventional method
or under hysteroscopic guidance. Relief of symptoms is dramatic.[9]
Conclusion
These days, when there are alternative medical methods of
performing medical termination of pregnancy, procedures like
dilation and curettage must be avoided as much as possible. However,
in a case of a female patient presenting with abnormal uterine bleeding post-medical termination of pregnancy, a high degree of suspicion
must be raised to look out for intrauterine retained foetal bones. A
transvaginal scan done by a trained radiologist should be enough to
confidently diagnose the condition if it happens. Often in these cases,
cross-sectional imaging is not as helpful as a transvaginal ultrasound.
Acknowledgement
Department of Radiodiagnosis and Department of Obstetrics
and Gynaecology, Bharat Ratna Dr Babasaheb Ambedkar Municipal
Hospital.
References
Citation
Kshirsagar S, Masrani S, Patil P, Gupta A, Saha D. A Rare Case of Intrauterine Retained Foetal Bones Clinically Presenting with Pelvic Pain and Dysmenorrhea Following First Trimester Medical Termination of Pregnancy. Indian J Appl Radiol. 2023;9(1): 183.